

Abstract
The personality-related construct of behavioral disinhibition is hypothesized to confer a generalized risk for alcohol and drug dependence. On average, rates of substance use and scores on measures of disinhibition peak in adolescence and decline as people mature into adulthood. The present study investigated this developmental change by evaluating the relationship between disinhibition and substance use disorders using a longitudinal study of 2,608 twins assessed at ages 17, 24, and 29. These ages include the period of highest risk for substance use disorders (ages 17-24) as well as when substance dependence symptoms typically decline (ages 24-29). Disinhibition was measured with the Multidimensional Personality Questionnaire higher-order scale of Constraint, as well as its constituent facet scales of Harm Avoidance, Control, and Traditionalism. Constraint’s relationship with substance dependence was statistically significant but small and largely genetic, with the genetic relationship declining from adolescence into adulthood. However, this result appeared to be almost entirely driven by Traditionalism, a propensity to hold traditional moral and social values, and not an obvious component of behavioral disinhibition. The results suggest that personality measures of Control and Harm Avoidance play only a small role in the development of substance dependence during late adolescence, and previous findings linking personality measures of disinhibition and substance use may be driven significantly by social and moral values than deficits in impulse control.
A wealth of research has shown that substance use disorders tend to co-occur with one another and with antisocial behavior. Dispositional traits such as sensation seeking, impulsivity, and low constraint have also been shown to be associated with the psychopathological symptoms that load on what has been termed an ‘externalizing’ spectrum (Kotov, Gamez, Schmidt, & Watson, 2010; Krueger et al., 2002; Sher & Trull, 1994; Young, Stallings, Corley, Krauter, & Hewitt, 2000). Prior research using cross-sectional data has revealed that both the externalizing spectrum and personality traits associated with it are heritable (Kendler, Prescott, Myers, & Neale, 2003; McGue, Bacon, & Lykken, 1993) and can be modeled together as a highly heritable externalizing factor (Krueger et al., 2002). This idea has gained momentum, considering recent proposals to re-organize the Diagnostic and Statistical Manual of Mental Disorders (DSM; (American Psychiatric Association, 2000)) in terms of the empirical covariance structures observed through factor analysis of disorder co-occurrences. In addition, there has been increasing interest in linking Axis I and Axis II disorders through various continuum models of psychopathology, where specific symptoms or disorders are conceptualized as manifestations of a few underlying spectra of vulnerability. Among these is the externalizing spectrum (Krueger, Markon, Patrick, & Iacono, 2005), which is hypothesized to link disinhibitory personality traits and antisocial personality disorder with substance use pathology.
It remains to be thoroughly investigated how the traditionally distinct domains of personality and substance dependence co-evolve from adolescence to adulthood. The purpose of this study was to examine the associations between the personality construct of constraint (related to behavioral disinhibition) and the co-occurrence of substance use disorders longitudinally using a large population-representative twin sample followed from the age of 17 until 29.
Although the trends for males and females are different, rates of substance use disorders in the U.S. tend to increase from adolescence to young adulthood, and decline thereafter. Male rates of dependence climb faster and higher than female rates and the correlations between common substances decline faster in females after age 17 (Vrieze, Hicks, Iacono, & McGue, 2012). Adolescence is also a time of increased impulsiveness and decreased planfulness. It is thought that these heightened levels of impulsivity contribute to the increased rates of experimentation with, and misuse of, common substances during the late teens and early twenties (Iacono, Malone, & McGue, 2008).
It has long been proposed that there are significant links between personality traits and substance dependence diagnoses (Cloninger, 1987), and that this link has a substantial genetic basis. In a meta-analysis, Kotov et al. (2010) found a correlation of .24 between personality measures of disinhibition and alcohol dependence. In a large twin sample Slutske et al. (2002) found a slightly larger phenotypic correlation of .38, and calculated that 50% of the correlation was due to additive genetic factors in males (70% in females), implicating a shared genetic etiology among disinhibition and alcohol dependence. Others have found similar genetic covariances among measures of disinhibition and substance use or dependence (Krueger et al., 2002; Young et al., 2000), where common factors extracted from the measures of SUDs and personality disinhibition in these studies were over 80% heritable. There is recent evidence using genome-wide association studies that the relationship can be detected at the molecular genetic level of single nucleotide polymporphisms (SNPs), in that SNP-based genetic scores developed on an indicator of disinhibition is predictive of scores on substance use measures (Vrieze, McGue, Miller, Hicks, & Iacono, 2013).
Additional traction for understanding adolescent change and its impact on addiction can be gained with longitudinal studies of adolescent substance use and personality. While early adolescent disinhibition is known to predict later substance use and dependence (Caspi et al., 1997; Chassin, Flora, & King, 2004; Elkins, King, McGue, & Iacono, 2006; Sher & Trull, 1994; Zucker, Heitzeg, & Nigg, 2011), it is less clear how the relationship between disinhibition and substance use/dependence unfolds during the transition from adolescence to adulthood. One way to tackle the problem is simply to evaluate how the correlations among substance use disorders change with age. If disinhibition—a vulnerability factor predicted to affect risk for all substances—is more important in causing substance use disorders at young ages then one would expect those disorders to be more highly correlated at young ages, and less correlated at older ages, all else being equal. This was supported by a recent study of twins measured longitudinally from 14 to 29, where Vrieze et al. (2012) found that at ages 14 and 17, a common factor loading onto symptom counts of alcohol, nicotine, and marijuana accounted for 51-57% of the variance in the symptom counts. By ages 24 and 29, however, the variance accounted for by the common factor was cut in half, indicating that some general liability to substance use—such as disinhibition—is very important for the development of substance use and conduct problems in adolescence, and its influence declines with age.
Here we describe a more direct test of the disinhibitory hypothesis, by evaluating patterns of change in the correlations among measures of personality disinhibition and substance use. We use substance dependence symptoms along with the Multidimensional Personality Questionnaire (MPQ; (Tellegen & Waller, 2008)) superfactor of Constraint. The Constraint scale is itself composed of facet-level scales of behavioral control, harm-avoidance, and adherence to traditional values. If adolescent substance use and abuse is driven by disinhibition then we expect measures of constraint to be more highly correlated with substance use in adolescence (i.e., at age 17 in this sample) and for this relationship to abate as the adolescents mature into their twenties. To test for this hypothesized trend, we fit a longitudinal factor model wherein symptom counts of alcohol, nicotine, and marijuana dependence, as well as the MPQ superfactor Constraint loaded on a single factor. We then tested whether the loadings for the substance use disorder symptom counts and constraint on the general factor declined over time. We further evaluated the relationship by testing for decline with each of Constraint’s component subscales of Traditionalism, Harm Avoidance, and Control. Facet-level analysis, in this case, has the potential to provide a more nuanced perspective on the nature of the known relationship among SUDs and constraint.
There already exists some evidence in the literature for a decline in the strength of association between personality-measured disinhibition and substance use behavior. Littlefield, Sher, and Wood (2009), for example, reported correlations between impulsivity measured by a mix of items from the Eyesenck Personality Questionnaire and the Tridimensional Personality Questionnaire and a problematic drinking sumscore from a brief questionnaire of drinking behavior. They found a correlation of .28 at age 18 that dropped to .17 at age 35, although the decline was not tested for statistical significance in their sample of 483. The present sample of over 2600 twins, with MPQ personality measures and in-person diagnostic interviews, is well suited to address this question with high power and clinically relevant diagnostic measures.
Finally, as posited by the disinhibitory hypothesis, since we expect the relationship between constraint and substance dependence to be genetically influenced, we decomposed the correlations into their genetic, shared environmental, and non-shared environmental contributions. Based on the high genetic covariance among measures of disinhibition and substance use (Krueger et al., 2002; Young et al., 2000), we expect that any observed correlation is genetically influenced, and that decline in the relationship between constraint and substance dependence is due to a decline in genetic correlation among these measures.
Method
Sample
The present sample was taken from the Minnesota Center for Twin and Family Research (Iacono, McGue, & Krueger, 2006), a population representative sample of families of twins. The sample consists of two cohorts initially assessed in adolescence and followed at 3-5 year intervals. The first cohort (N = 1252; 54% female) was initially assessed at age 17 and re-assessed for personality and substance use at ages 24 and 29. The second cohort (N = 2510; 51% female) was also assessed for personality and substance use at ages 17, 24, and 29. The age-17 assessment was lifetime; follow-up assessments covered events occurring in the last 3-4 years. Cohorts were collapsed for all analyses. The results did not change after statistical correction for cohort status. Zygosity was initially assessed through questionnaire, which has since been validated through genome-wide genotyping. The sample is primarily (>90%) composed of individuals of European descent who self-identify as White (M. B. Miller et al., 2012). Attrition in the sample has been modest; participation rates ranged from 87.3% to 93.6% across all follow-up assessments. To examine the effect of attrition on substance use, we compared 17-year-olds who were eligible for and completed later waves of assessment versus those who did not. For males, Cohen’s d for mean differences in age 17 substance dependence symptoms between those who did versus did not complete the later assessments were .00, −.08, and .09 for nicotine, alcohol, and marijuana, respectively. For females, Cohen d’s for similar comparisons were −.19, −.01, and .13 (all p’s>.05). A similar analysis with the personality measures revealed Cohen’s d’s of .08, .12, −.25, and .01 for females for Traditionalism, Control, Harm Avoidance, and Constraint, respectively. Disregarding multiple testing, the only significant difference was for Harm Avoidance (p=.04), in that females lower on harm avoidance were less likely to return for follow-up. For males, we observed Cohen’s d’s of .17, −.27, −.11, and −.17 for Traditionalism, Control, Harm Avoidance, and Constraint, respectively (all p’s>.05).
Measures
Participants were assessed for DSM-III-R (American Psychiatric Association, 1987) symptoms of nicotine dependence, alcohol dependence/abuse and marijuana dependence/abuse during in-person interviews with trained interviewers. While intake interviews diagnosed the presence of lifetime symptoms (i.e., up to the age of 17), follow-up assessments covered symptoms present since the last assessment (in the case of the age-24 assessment this covers approximately the last three years because twins were also clinically assessed at age 21, but personality was not measured at this age).
In-person clinical assessments used a modified version of the Substance Abuse Module (SAM; (Robins, Babor, & Cottler, 1987)) of the Composite International Diagnostic Interview (CIDI; (Robins et al., 1988)). The SAM had been modified only to provide sufficient coverage of DSM-IV criteria, while retaining all coverage of DSM-3R criteria. Diagnoses were verified in a consensus process, wherein graduate students and staff with advanced training in clinical assessment reviewed cases to verify symptom presence. Inter-rater reliability of substance use disorder diagnosis was greater than .91 (Iacono, Carlson, Taylor, Elkins, & McGue, 1999).
The personality trait of constraint was assessed using the MPQ (Tellegen & Waller, 2008). The MPQ is psychometrically sound, and has been described in great detail elsewhere (Johnson, Krueger, Bouchard, & McGue, 2002; Tellegen & Waller, 2008). Briefly, it consists of 3 superfactors – Positive Emotionality, Negative Emotionality, and Constraint. For the purposes of the current study, we focused on the Constraint superfactor, which has been linked to externalizing disorders (Krueger et al., 2002), and represents our best personality measure of behavioral disinhibition. It consists of three subscales – Control which measures the tendency to plan one’s actions as opposed to acting impulsively; Harm Avoidance, which indexes the propensity to prefer safe but tedious activities rather than thrilling but potentially dangerous activities; and Traditionalism, which assesses the degree to which an individual endorses and engages in conventional beliefs and behaviors. Constraint on the MPQ is calculated as a weighted sum of all the MPQ subscales (where the weights have been derived through factor analysis). While all subscales load onto Constraint, the loadings for Harm Avoidance, Control, and Traditionalism were by far the most heavily weighted scales, and loadings for the other subscales are very close to zero.
Analysis
We focused on two primary analyses to examine the developmental association between substance use disorders and the MPQ personality scales. All analyses took advantage of the twin sample, and corrected for within-family covariance as a function of twin zygosity according to standard methods (Martin & Eaves, 1977). First, for each age of assessment (17, 24, and 29), we estimated the 4×4 correlation matrix among nicotine, alcohol, marijuana, and personality, separately for each of the four personality measures. Using knowledge of twin zygosity (monozygotic versus dizygotic) we decomposed the correlation matrix into A, C, and E components, where A is the additive genetic, C the shared environmental, and E the non-shared environmental component. Summing the A, C, and E component matrices (A+C+E) provides the expected phenotypic correlation matrix based on the model (i.e., the same expected correlation matrix you would get in a non-twin sample of unrelated individuals, if the twin model is correct). For each ACE model we assumed that means and variances were equal across both members of twin pair.
Next, we fit confirmatory factor models to the longitudinal data. An example path diagram is portrayed in Figure 1. As can be seen in the figure, a longitudinal factor model was fit, with one factor loading onto each of the three substance dependence symptom counts, as well as a single MPQ scale, at each age of assessment. A separate model was fit for each of the four MPQ scales (Constraint, Harm Avoidance, Control, and Traditionalism), separately for males and females, resulting in a total of 8 models. Figure 1 is intentionally incomplete; if all estimated paths are drawn the figure becomes unwieldy. Factor variances were decomposed into the A, C, and E components, which were allowed to covary across time at the factor level. Further, the within-measure residual factors were also decomposed into A, C, and E, and were allowed to covary across time, to avoid artifactual inflation of the factor loadings and/or covariances by residual non-independence. For example, nicotine at time 1 will correlate with nicotine at time 2 for reasons not associated with the common factor (e.g., addictive properties of smoking), and this is accounted for by allowing the nicotine residuals to correlate.
Figure 1.
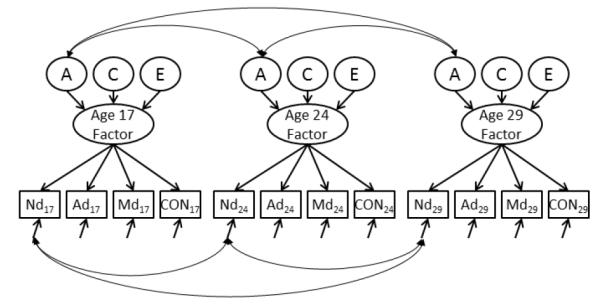
Longitudinal Factor Model. Part of the longitudinal factor model is shown here. Nd = Nicotine Dependence; Ad = Alcohol Abuse/Dependence; Md = Marijuana Abuse/Dependence; CON is the MPQ subfactor of Control. Separate models were fit for each of constraint, Traditionalism, Control, and Harm Avoidance. Manifest variables are shown in boxes, factors are in ovals, and the ACE components are in circles. For each age the covariance among measures were modeled by a single factor. The variance of the factor is then decomposed into A, C, or E, and those are allowed to covary across all ages. To keep the figure legible, we show covariances only for the A component; in reality the C and E components also covaried over time. Within-measure residuals are also allowed to covary. Again, for simplicity we show only one within-measure across-age covariance, that for Nicotine Dependence. The same residual covariances were estimated for alcohol, marijuana, and the MPQ measure.
As a preliminary step, we tested for measurement invariance (Widaman, Ferrer, & Conger, 2010) in Constraint, by fitting a similar longitudinal factor model to the facet MPQ scales of Control, Harm Avoidance, and Traditionalism. This model is equivalent to that displayed in Figure 1, except there are only three manifest variables at each age, and those manifest variables are the three MPQ facet scales. To test for weak invariance, we constrained loadings to be equivalent across the three ages of assessment, for each MPQ facet scale. Even weak measurement invariance is known not to hold for the nicotine, alcohol, and marijuana symptom counts (Vrieze et al., 2012); hence we did not explicitly test for it.
Longitudinal factor models were compared to longitudinal saturated models for fit. All models used Cholesky decompositions of the variance-covariance matrices, and were fit by full information maximum likelihood, which allows likelihood ratio tests. Likelihood ratio tests, and their resulting χ2 distributions are known to be overly sensitive to sample size, such that useful models are routinely rejected at high levels of significance. Additionally, the likelihood ratio test is known from theory and simulation to be suboptimal in many ways, and other criteria have been developed to improve upon the likelihood ratio test (Vrieze, 2012). We therefore used the Akaike Information Criterion (AIC) to determine model fit, as it is expected to select the model that will minimize common error statistics, such as mean error of estimation, upon cross-validation (Vrieze, 2012). We note that in our particular case other fit indices, such as the Bayesian Information Criterion (BIC), produced the same results. When reporting the AIC, we report the null model AIC minus the alternative model AIC. Positive values indicate evidence for the alternative model.
Finally, as a direct test of the change in relationship between personality constraint and substance use comorbidity, we tested for decline in the squared MPQ factor loading over time. The squared loading represents the amount of variance in the MPQ measure accounted for by the common factor. Alternatively, it can be interpreted as the coefficient of determination (R2) between the common factor and the MPQ measure. If the loading declines with age, it demonstrates that the relationship between the personality measure and substance dependence common variance is declining as well, suggesting that etiological processes common to both SUDs and personality are diminishing over time. The factor loading can also be decomposed, in a sense, into additive genetic, shared environmental, and non-shared environmental contributions, by multiplying the squared MPQ factor loading at each age by the corresponding factor A, C, or E contribution. To test for change over time, we refit each longitudinal factor model constraining the squared factor loading (or its A, C, or E contribution) to be equal at all available ages. This constrained model was then compared to the original model for fit using a likelihood ratio test. The null hypothesis here is that there is no decline in covariance, with a resulting one-tailed test. We also examined these tests with an AIC test for no change in covariance. This test was always consistent with the likelihood ratio test results reported here, except that the female phenotypic decline for Constraint was determined significant by the AIC. The corresponding likelihood ratio p-value for this decline was .06, as reported in the Results.
Results
Both substance use and personality showed mean-level change from age 17 to 29, as can be seen in Table 1 and Figure 2. The trajectory of change is very different between SUDs and personality. The mean SUD symptoms rose from 17 to 24, and declined thereafter, with the exception of marijuana dependence symptom counts in females, which declined continuously after 17. MPQ scales, on the other hand, increased monotonically from age 17 to age 29. Note, however, that the assessment points are not entirely comparable, as the SUDs were measured over the past ~3 years, whereas no such time frame was specified for the MPQ. The MPQ therefore represents a more contemporaneous snapshot of each individual’s personality at his or her age-of-assessment.
Table 1.
Sample size, means, and standard deviations for the DSM−3R substance use symptom counts and MPQ personality measures.
| Sex | Cohort | Age | DSM-3R Dependence/Abuse Symptom Counts | Multidimensional Personality Questionnaire | |||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
| |||||||||||||||||||||||
| Superfactor | Subfactors | ||||||||||||||||||||||
|
| |||||||||||||||||||||||
| Nicotine | Alcohol | Marijuana | Constraint | Traditionalism | Harm Avoidance | Control | |||||||||||||||||
|
| |||||||||||||||||||||||
| N | M | SD | N | M | SD | N | M | SD | N | M | SD | N | M | SD | N | M | SD | N | M | SD | |||
| Male | 1 | 17.5 | 578 | .7 | (1.6) | 578 | .6 | (1.4) | 578 | .3 | (1.2) | 501 | 129.7 | (15.3) | 503 | 51.0 | (7.2) | 505 | 42.5 | (9.7) | 507 | 46.4 | (7.1) |
| 24.3 | 525 | 1.3 | (1.9) | 525 | 1.5 | (1.8) | 524 | .5 | (1.4) | 431 | 135.7 | (15.6) | 432 | 52.9 | (7.5) | 434 | 44.6 | (10.7) | 433 | 48.9 | (7.5) | ||
| 29.7 | 532 | 1.2 | (1.8) | 532 | 1.0 | (1.5) | 530 | .4 | (1.2) | 511 | 139.4 | (15.0) | 513 | 53.3 | (6.6) | 517 | 47.3 | (10.3) | 517 | 50.4 | (7.3) | ||
| 2 | 18.0 | 661 | 1.2 | (1.9) | 663 | .9 | (1.7) | 664 | .8 | (1.9) | 635 | 130.6 | (14.8) | 638 | 51.2 | (6.7) | 643 | 42.7 | (9.4) | 642 | 47.1 | (7.0) | |
| 25.3 | 640 | 1.3 | (1.8) | 639 | 1.3 | (1.7) | 640 | .5 | (1.30) | 581 | 134.6 | (15.3) | 587 | 51.3 | (7.5) | 595 | 43.8 | (10.1) | 595 | 49.6 | (7.4) | ||
| 29.3 | 425 | 1.4 | (1.9) | 425 | .8 | (1.5) | 425 | .8 | (1.3) | 428 | 138.3 | (15.2) | 429 | 52.1 | (7.3) | 432 | 45.5 | (10.5) | 431 | 51.3 | (7.8) | ||
| Female | 1 | 17.5 | 674 | .7 | (1.7) | 674 | .4 | (1.3) | 674 | .2 | (.9) | 614 | 137.1 | (16.1) | 616 | 52.3 | (7.1) | 622 | 49.0 | (10.3) | 620 | 47.5 | (7.7) |
| 25.0 | 633 | 1.0 | (1.6) | 634 | .5 | (1.2) | 634 | .2 | (.9) | 590 | 146.2 | (14.1) | 592 | 53.0 | (6.9) | 597 | 54.7 | (9.4) | 596 | 52.4 | (7.3) | ||
| 29.6 | 636 | .8 | (1.6) | 636 | .3 | (1.0) | 635 | .1 | (.5) | 609 | 149.0 | (14.8) | 614 | 53.1 | (7.2) | 619 | 56.9 | (9.4) | 621 | 53.6 | (7.5) | ||
| 2 | 18.3 | 692 | .8 | (1.6) | 692 | .3 | (.9) | 692 | .2 | (.9) | 684 | 139.2 | (15.3) | 692 | 52.5 | (6.6) | 699 | 50.7 | (9.8) | 697 | 48.7 | (7.7) | |
| 25.2 | 579 | .9 | (1.6) | 578 | .6 | (1.3) | 576 | .2 | (.7) | 637 | 144.4 | (14.7) | 642 | 51.8 | (6.6) | 652 | 53.5 | (9.8) | 653 | 52.1 | (7.7) | ||
Note: Cohorts were combined for all analysis. A third wave of data collection is ongoing for the 2nd female cohort.
Figure 2.

Longitudinal Means for All Measures. Note: all measures are standardized within-measure by the age 17 mean and standard variation.
Correlations among MPQ scales and SUDs are reported in Table 2. Correlations are reported separately for males and females, as the longitudinal correlation matrices were quite different for males and females, according to the chi square test (χ2(78) = 210.2, p=4.4×10−14), as well as the AIC difference between the models (−54.2). In Table 2 we find that, for the most part, shared environmental and non-shared environmental correlations between SUDs and MPQ scales were negligible—i.e., with absolute values generally less than .1—and showed no discernibly consistent pattern with age. Phenotypic correlations, and the genetic components, were relatively larger in magnitude. There is no consistent decline in the magnitude of correlation between alcohol dependence and any personality measure. Correlations with marijuana dependence and nicotine dependence, on the other hand, do show decline for Traditionalism in males (p<.05, respectively) and for Constraint and Traditionalism for females (both p’s<.05), as tested by a likelihood ratio test constraining the substance-personality correlations to be equal at each age. Note that all genetic and environmental contributions are scaled such that summing them produces the phenotypic correlations.
Table 2.
Correlations of Substance Use Disorder Symptom Counts with Constraint, Traditionalism, Harm Avoidance, and Control
| Sex | Personality Measure |
Age | Phenotypic Correlation | Genetic Contribution | Shared Environmental Contribution |
Non-shared Environmental Contribution |
||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Md | Ad | Nd | Md | Ad | Nd | Md | Ad | Nd | Md | Ad | Nd | |||
|
| ||||||||||||||
| Male | Constraint | 17 | −.20 | −.23 | −.20 | −.16 | −.10 | −.09 | −.01 | −.03 | −.05 | −.04 | −.10 | −.06 |
| 24 | −19 | −.24 | −.19 | −.17 | −.18 | −.15 | .01 | .02 | .02 | −.03 | −.08 | −.06 | ||
| 29 | −.16 | −.23 | −.15 | −.08 | −.10 | −.03 | −.03 | −.04 | −.05 | −.05 | −.09 | −.07 | ||
| Traditionalism | 17 | −.20a | −.17 | −.18b | −.16 | −.15 | −.11 | −.01 | .01 | −.03 | −.02 | −.03 | −.04 | |
| 24 | −.15a | −.18 | −.14b | −.13 | −.15 | −.13 | .01 | .05 | .00 | −.02 | −.07 | −.01 | ||
| 29 | −.09a | −.14 | −.06b | .02 | .02 | .16 | −.07 | −.08 | −.16 | −.04 | −.07 | −.06 | ||
| Harm Avoidance |
17 | −.04 | −.08 | −.08 | −.04 | −.03 | −.03 | −.02 | −.02 | −.03 | .02 | −.04 | −.01 | |
| 24 | −.06 | −.15 | −.10 | −.07 | −.17 | −.11 | .02 | .06 | .05 | .00 | −.04 | −.03 | ||
| 29 | −.10 | −.18 | −.13 | −.06 | .00 | −.08 | −.02 | −.06 | −.01 | −.02 | −.12 | −.04 | ||
| Control | 17 | −.19 | −.23 | −.18 | −.10 | −.09 | −.03 | −.04 | −.05 | −.07 | −.05 | −.09 | −.08 | |
| 24 | −.18 | −.20 | −.20 | −.13 | −.13 | −.13 | .01 | .01 | .01 | −.06 | −.08 | −.07 | ||
| 29 | −.14 | −.18 | −.18 | −.07 | −.09 | −.01 | −.04 | −.02 | −.09 | −.04 | −.07 | −.08 | ||
| Females | Constraint | 17 | −.26c | −.24 | −.25a | −.19 | −.17 | −.18 | .02 | .01 | −.01 | −.09 | −.08 | −.06 |
| 24 | −.20c | −.20 | −.19a | −.19 | −.15 | −.11 | .01 | .01 | −.05 | −.02 | −.06 | −.03 | ||
| 29 | −.10c | −.23 | −.17a | −.09 | −.07 | −.08 | −.04 | .01 | −.02 | −.02 | −.18 | −.07 | ||
| Traditionalism | 17 | −.19 | −.14 | −.22b | −.07 | −.03 | −.05 | −.04 | −.05 | −.10 | −.07 | −.06 | −.06 | |
| 24 | −.15 | −.13 | −.13b | −.16 | −.18 | .02 | .04 | .06 | −.12 | −.03 | .00 | −.03 | ||
| 29 | −.09 | −.12 | −.10b | −.02 | −.02 | −.05 | −.04 | .03 | −.05 | −.03 | −.12 | .00 | ||
| Harm Avoidance |
17 | −.16a | −.12 | −.06 | −.12 | −.12 | −.11 | .01 | .02 | .07 | −.05 | −.02 | −.02 | |
| 24 | −.12a | −.11 | −.04 | −.11 | −.14 | −.01 | .01 | .03 | −.02 | −.02 | 0 | −.01 | ||
| 29 | −.04a | −.13 | −.10 | −.03 | −.11 | −.02 | −.06 | .01 | −.04 | .05 | −.02 | −.04 | ||
| Control | 17 | −.22b | −.25 | −.25 | −.16 | −.16 | −.15 | 0 | 0 | 0 | −.07 | −.09 | −.10 | |
| 24 | −.17b | −.24 | −.25 | −.16 | −.12 | −.16 | 0 | 0 | −.02 | −.01 | −.12 | −.07 | ||
| 29 | −.09b | −.28 | −.26 | −.12 | −.09 | −.14 | −.01 | .02 | −.02 | .04 | −.20 | −.10 | ||
Note: Md = Marijuana abuse/dependence symptom count; Ad = Alcohol abuse/dependence symptom count; Nd = Nicotine abuse/dependence symptom count. Bold indicates that the observed longitudinal decline is significant.
p < .05,
p<.01,
p<.001.
Note that the genetic, shared environmental, and non-shared environmental contributions are scaled such that summing them provides the phenotypic correlation (except for some rounding error).
We next tested for factorial invariance in a longitudinal factor model of Control, Harm Avoidance, and Traditionalism. The male model was weakly invariant (invariance of factor loadings) according to the AIC difference (0.7) and a chi square difference test (male model χ2(6)=11.35, p=.08); the female model was not, with an AIC difference of −7.1, and a significant chi square test (χ2(6)=19.07, p = .004). Strong invariance requires equivalence of means and loadings, which we know based on prior research is not true for personality during adolescence, and indeed, strong invariance did not hold in this sample for males (χ2(6)=531.2, p=5×10−106) or females (χ2(6)=634.64, p=4×10−128). These results indicate that Constraint, composed of Control, Harm Avoidance, and Traditionalism, is not entirely etiologically stable during these ages, for males or females.
Fit statistics for the eight longitudinal factor models of substance dependence symptom counts and personality are given in Table 3. For each model, the longitudinal factor model was preferable to the saturated model, as judged by the AIC. Tests of age-related decline in the squared MPQ loading over time are displayed in Figure 3. Phenotypically, only Traditionalism showed any decline in its relationship to the other SUDs over time (p=.002 for males and p=.003 for females). Both Traditionalism and Constraint showed decreases in the additive genetic relationship with SUDs (p=.0005 and p=.04 for males; p=.002 and p=.04 for females, respectively). No significant decrease was found for any shared or non-shared environmental relationship.
Table 3.
Longitudinal Factor Model Fit
| Sex | MPQ Scale | Ages | Saturated Variance- Covariance |
Longitudinal Factor Model | Goodness of Fit | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
|
| |||||||||||
| −2LL | k | AIC | −2LL | k | AIC | X2 (df) | p-value | ΔAIC | |||
| Male | Constraint | 17, 24, 29 | 58081.2 | 246 | 31721.2 | 58295.8 | 114 | 31665.8 | 214.6(135) | 1.6e-5 | 55.4 |
| Traditionalism | 17, 24, 29 | 53759.4 | 246 | 27369.4 | 53934.8 | 114 | 27274.8 | 175.4 (135) | .01 | 94.6 | |
| Harm Avoidance | 17, 24, 29 | 55868.1 | 246 | 29430.1 | 56042.2 | 114 | 29334.2 | 174.0 (135) | .01 | 95.9 | |
| Control | 17, 24, 29 | 54325.5 | 246 | 27889.5 | 54504.8 | 114 | 27798.8 | 179.4 (135) | .006 | 90.7 | |
| Female | Constraint | 17, 24, 29 | 50760.7 | 246 | 25332.7 | 51016.8 | 114 | 25318.8 | 256.1 (135) | 1.5e-9 | 13.9 |
| Traditionalism | 17, 24, 29 | 46021.8 | 246 | 20549.8 | 46268.2 | 114 | 20526.2 | 246.4 (135) | 1.6e-8 | 23.6 | |
| Harm Avoidance | 17, 24, 29 | 48425.3 | 246 | 22887.3 | 48668.6 | 114 | 22860.6 | 243.2 (135) | 3.3e-8 | 26.7 | |
| Control | 17, 24, 29 | 47162.3 | 246 | 21628.3 | 47413.8 | 114 | 21609.8 | 251.6 (135) | 4.7e-9 | 18.5 | |
MPQ = Multidimensional Personality Questionnaire; k = number of estimated parameters in the model; AIC = Akaike Information Criterion. −2LL = negative two times the log of the likelihood. The X2 statistic here is the difference between the −2LL for the factor model and the saturated model. It is asymptotically distributed as X2 on degrees of freedom equal to the difference in number of estimated parameters. ΔAIC = saturated AIC minus factor model AIC. Provides the relative evidence for factor model over saturated model; positive values indicate support for longitudinal factor model.
Figure 3.

Age-Related Change in MPQ Loadings on the Substance Use Factor. Males are shown in the left column and females in the right column. Numbers within each panel are p-values corresponding to the change observed across age. The p-values are color-coded (e.g., a green p-value gives the significance of decline in Traditionalism). The additive genetic contribution is scaled such that adding it to the shared environment and non-shared environment contributions produces the phenotypic correlation. Non-shared and shared environmental contributions showed no significant declines, and therefore are not shown here.
Discussion
The current study examined genetic and environmental contributions to the relationship between the personality trait of MPQ Constraint and its subscales, and substance dependence symptoms from the ages of 17 to 29 in a large twin sample from the general population. In general, mean level substance dependence symptoms increased until the mid-twenties then declined over time (Figure 2). Personality measures of constraint continued to increase with age consistent with previous literature (Hopwood et al., 2011; Littlefield et al., 2009). Traditionalism was the only facet that showed relatively less mean-level change than the other personality scales, indicating that individuals on average do not shift to the same extent in their level of conformity or adherence to traditional moral values. Despite the trend for Traditionalism, the findings indicate that individuals, on average, are becoming increasingly constrained, controlled, harm avoidant, and traditional with age, during which time nicotine, alcohol, and marijuana symptoms are increasing and then declining. While these mean-level trends are interesting, the main hypothesis tested here is whether the magnitude of the correlation between personality measures of constraint and substance dependence symptom counts decreased over time. Such a result would suggest the relative importance of disinhibition, as measured here by Constraint, in early- to mid-adolescence for substance problems that abates with maturation into adulthood, regardless of any mean-level changes, as predicted by the disinhibitory theory.
On the phenotypic level, only the Traditionalism subfactor showed a decreasing correlation with substance dependence symptoms as the youths aged. However, both Constraint and Traditionalism showed a decreasing genetic relationship with substance dependence, consistent with the notion that as individuals age into adulthood the shared etiology among the substance dependence symptoms is less influenced by genes relevant to personality constraint and traditionalism. The effects for Constraint were marginally statistically significant, but reflect an almost 50% decrease in shared additive genetic variance. Despite this, the substance-specific results reported in Table 2 indicate that these global trends apply most strongly to marijuana and nicotine symptom counts, and do not appear to apply at all to alcohol symptom counts.
The most evidence for decline was evident for Traditionalism, which is a bipolar measure of conformity and religiosity at one pole, and rebelliousness and non-conformist behavior on the other pole. Harm Avoidance and Control did not show any consistent decline in their relationship with substance dependence, either to individual substances or to the substance dependence factor, despite the Control subfactor being more relevant to behavioral disinhibition as commonly defined (deficits in impulse control). Traditionalism also correlates with measures of political conservatism (r=.58), whereas Harm Avoidance and Control do not (r=.05 and .13 (Bouchard et al., 2003)). One interpretation of this finding is that substance use is one way to be non-conformist, but only really during adolescence or, in our case, during the age-17 assessment. Adult substance use is normative, especially for nicotine and alcohol, but possibly for marijuana too, as a more traditional outlook on marijuana has been changing. Thus, in adolescence, those high on Traditionalism see it as inappropriate to use these substances, and this plays a role in whether or not they actually use them. Conversely, adolescents low on Traditionalism see substances as yet another way to express their non-conformist attitude. As individuals age, substance use and abuse is no longer a way to express nonconformity, as the use of alcohol, nicotine, and marijuana is within normal limits. While intriguing, this interpretation is limited because we did not observe decline between Traditionalism and alcohol dependence (as seen in Table 2).
While suggestive, the present results do not uniformly support the notion that Constraint or its constituent scales are differentially relevant for adolescent, compared to adult, substance use and dependence. Indeed, others (Cyders et al., 2007; Dick et al., 2010; Whiteside & Lynam, 2001) have suggested that the constraint or impulsivity construct represents an amalgamation of different traits such as sensation seeking, novelty seeking, boredom proneness, impulsivity, and so on, and have a number of uncorrelated facets to them including lack of planning, lack of perseverance, need for stimulation or sensation seeking, and impulsive actions based on extremely positive or negative moods (or urgency). These facets may have different correlates as well. For example, while urgency predicted problematic behaviors such as drinking, gambling and binge eating, sensation seeking was associated with frequency of gambling and drinking (Cyders, Flory, Rainer, & Smith, 2009; Smith et al., 2007). Results from the animal literature support a similar, though not necessarily identical, distinction between the various constructs under the broad umbrella of impulsivity as well. For example, Belin et al. (2008) suggest that while novelty-seeking is related to the tendency to initiate cocaine use, that it is specifically high levels of impulsivity that leads to addiction in rats. Others make a distinction between response inhibition and delay aversion as well (see Dick et al., 2010 for a review). Similar to the results of this study, disinhibition does not appear to reflect a single underlying propensity towards externalizing behaviors. It is not apparent however where MPQ Traditionalism fits, since it does not appear to have a direct equivalent in the factor model outlined immediately above, or in the animal literature. It may perhaps be more similar to mood-related impulsivity facets, rather than others such as sensation seeking or lack of planning, though it is not clear why this should the case.
What is clear, however, is that personality measures of constraint, whether super- or sub-factor, are only a small part of the etiological picture in the onset and offset of common substance use disorders, at least at a population level. Looking only at the phenotypic model, the largest correlation between a personality measure and a SUD symptom count factor was for Control, which ranged from −.24 to −.27 for males, and for females from −.33 to −.35. Squaring this, we can calculate that Control accounts for 6% to 13% of the variance in the SUD common factor (displayed in the top panels of Figure 3), leaving 87-94% of the variance unexplained.
Ignoring the longitudinal factor model we see the phenotypic correlations reported in Table 2 lie between −.10 and −.25, indicating that Constraint, Control, Harm Avoidance, and Traditionalism account for between 1% and 7% of the variance in SUD symptom counts in this population sample. One issue highlighted in previous studies (Cyders & Smith, 2007; Krueger et al., 2002) is that the low correlation may be due to method-specific variance. That is, the high observed correlations between nicotine dependence and alcohol dependence (e.g., .70), for example, is due in part to method artifacts because they are both assessed by interview. Since the MPQ is a self-report questionnaire, it may be that this method of measurement is substantially different from interview, and these differences attenuate observed correlations between MPQ and SUD symptoms. In one study of the effect of method variance, Cyders and Smith (2007) found an average attenuation of r=.01 between interview and questionnaire-based impulsivity measures, suggesting method artifacts may not play a large role. Another explanation for the low correlations is that normal-range personality measures, including scales on the MPQ, are not measuring disinhibitory behavior or impulse control. It is clear, for example, that antisocial personality disorder correlates quite highly with alcohol, nicotine, and marijuana dependence (Regier et al., 1990). Researchers might consider using measures of pathological dis-constraint (e.g., the PSY-5; (Harkness, Finn, McNulty, & Shields, 2012)) or experimental paradigms of behavioral control (Bickel, Odum, & Madden, 1999; Green & Myerson, 2004; Holt, Green, & Myerson, 2003; J. Miller, Flory, Lynam, & Leukefeld, 2003) to more directly test the role of disinhibition in the development of substance use. Alternatively, it may be that the etiological overlap between personality and substance use psychopathology is modest at best. As noted earlier, many other studies (Kotov et al., 2010; Krueger et al., 2002; Littlefield et al., 2009) have found that personality measures correlate to approximately the same extent observed here, whether in population or patient samples, indicating that small correlations, with absolute values often much less than .30, are expected between the domains of substance use and disinhibitory personality.
ACKNOWLEDGMENTS
The research was supported by grants DA 05147, DA 13240, DA 024417, and DA 025868 of the National Institute on Drug Abuse; AA 09367 of the National Institute on Alcohol Abuse and Alcoholism; and MH 017069 of the National Institute of Mental Health. Brian M. Hicks was supported by DA 025868.
Footnotes
DISCLOSURES: No author had any competing interests with respect to the present work.
References
- American Psychiatric Association . Diagnostic and statistical manual of mental disorders. 3rd. Author; Washington, D.C.: 1987. rev. [Google Scholar]
- American Psychiatric Association . Diagnostic and Statistical Manual of Mental Disorders. 4th. Author; Washington, DC: 2000. text rev. [Google Scholar]
- Belin D, Mar AC, Dalley JW, Robbins TW, Everitt BJ. High Impulsivity Predicts the Switch to Compulsive Cocaine-Taking. Science. 2008;320(5881):1352–1355. doi: 10.1126/science.1158136. doi: 10.1126/science.1158136. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bickel WK, Odum AL, Madden GJ. Impulsivity and cigarette smoking: delay discounting in current, never, and ex-smokers. Psychopharmacology (Berl) 1999;146(4):447–454. doi: 10.1007/pl00005490. [DOI] [PubMed] [Google Scholar]
- Bouchard TJ, Segal NL, Tellegen A, McGue M, Keyes M, Krueger R. Evidence for the construct validity and heritability of the Wilson-Patterson conservatism scale: a reared-apart twins study of social attitudes. Personality and Individual Differences. 2003;34(6):959–969. [Google Scholar]
- Caspi A, Begg D, Dickson N, Harrington H, Langley J, Moffitt TE, Silva PA. Personality differences predict health-risk behaviors in young adulthood: evidence from a longitudinal study. Journal of Personality and Social Psychology. 1997;73(5):1052–1063. doi: 10.1037//0022-3514.73.5.1052. [DOI] [PubMed] [Google Scholar]
- Chassin L, Flora DB, King KM. Trajectories of alcohol and drug use and dependence from adolescence to adulthood: The effects of familial alcoholism and personality. Journal of Abnormal Psychology. 2004;113(4):483–498. doi: 10.1037/0021-843X.113.4.483. doi: 10.1037/0021-843x.113.4.483. [DOI] [PubMed] [Google Scholar]
- Cloninger CR. Neurogenetic adaptive mechanisms in alcoholism. Science. 1987;236:410–416. doi: 10.1126/science.2882604. [DOI] [PubMed] [Google Scholar]
- Cyders MA, Flory K, Rainer S, Smith GT. The role of personality dispositions to risky behavior in predicting first-year college drinking. Addiction. 2009;104(2):193–202. doi: 10.1111/j.1360-0443.2008.02434.x. doi: 10.1111/j.1360-0443.2008.02434.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cyders MA, Smith GT. Mood-based rash action and its components: Positive and negative urgency. Personality and Individual Differences. 2007;43(4):839–850. doi: DOI 10.1016/j.paid.2007.02.008. [Google Scholar]
- Cyders MA, Smith GT, Spillane NS, Fischer S, Annus AM, Peterson C. Integration of impulsivity and positive mood to predict risky behavior: Development and validation of a measure of positive urgency. Psychological Assessment. 2007;19(1):107–118. doi: 10.1037/1040-3590.19.1.107. doi: 10.1037/1040-3590.19.1.107. [DOI] [PubMed] [Google Scholar]
- Dick DM, Smith GC, Olausson P, Mitchell SH, Leeman RF, O'Malley SS, Sher K. Understanding the construct of impulsivity and its relationship to alcohol use disorders. Addiction Biology. 2010;15(2):217–226. doi: 10.1111/j.1369-1600.2009.00190.x. doi: 10.1111/j.1369-1600.2009.00190.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Elkins Irene J., King Serena M., McGue Matt, Iacono William G. Personality traits and the development of nicotine, alcohol, and illicit drug disorders: Prospective links from adolescence to young adulthood. Journal of Abnormal Psychology. 2006;115(1):26–39. doi: 10.1037/0021-843X.115.1.26. doi: 10.1037/0021-843x.115.1.26. [DOI] [PubMed] [Google Scholar]
- Green L, Myerson J. A discounting framework for choice with delayed and probabilistic rewards. Psychological Bulletin. 2004;130(5):769–792. doi: 10.1037/0033-2909.130.5.769. doi: Doi 10.1037/0033-2909.130.5.769. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Harkness AR, Finn JA, McNulty JL, Shields SM. The Personality Psychopathology-Five (PSY-5): Recent Constructive Replication and Assessment Literature Review. Psychological Assessment. 2012;24(2):432–443. doi: 10.1037/a0025830. doi: Doi 10.1037/A0025830. [DOI] [PubMed] [Google Scholar]
- Holt DD, Green L, Myerson J. Is discounting impulsive? Evidence from temporal and probability discounting in gambling and non-gambling college students. Behavioural Processes. 2003;64(3):355–367. doi: 10.1016/s0376-6357(03)00141-4. [DOI] [PubMed] [Google Scholar]
- Hopwood CJ, Donnellan MB, Blonigen DM, Krueger RF, McGue M, Iacono WG, Burt SA. Genetic and Environmental Influences on Personality Trait Stability and Growth During the Transition to Adulthood: A Three-Wave Longitudinal Study. Journal of Personality and Social Psychology. 2011;100(3):545–556. doi: 10.1037/a0022409. doi: Doi 10.1037/A0022409. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Iacono WG, Carlson SR, Taylor J, Elkins IJ, McGue M. Behavioral disinhibition and the development of substance use disorders: Findings from the Minnesota Twin Family Study. Development and Psychopathology. 1999;11:869–900. doi: 10.1017/s0954579499002369. [DOI] [PubMed] [Google Scholar]
- Iacono WG, Malone SM, McGue M. Behavioral disinhibition and the development of early-onset addiction: Common and specific influences. Annual Review of Clinical Psychology. 2008;4:325–348. doi: 10.1146/annurev.clinpsy.4.022007.141157. doi: DOI 10.1146/annurev.clinpsy.4.022007.141157. [DOI] [PubMed] [Google Scholar]
- Iacono WG, McGue M, Krueger RF. Minnesota Center for Twin and Family Research. Twin Res Hum Genet. 2006;9(6):978–984. doi: 10.1375/183242706779462642. doi: 10.1375/183242706779462642. [DOI] [PubMed] [Google Scholar]
- Johnson Wendy, Krueger Robert F., Bouchard Thomas J., McGue Matt. The personalities of twins: Just ordinary folks. Twin Research. 2002;5(2):125–131. doi: 10.1375/1369052022992. [DOI] [PubMed] [Google Scholar]
- Kendler Kenneth S., Prescott Carol A., Myers John, Neale Michael C. The structure of genetic and environmental risk factors for common psychiatric and substance use disorders in men and women. Archives of general psychiatry. 2003;60(9):929–937. doi: 10.1001/archpsyc.60.9.929. doi: 10.1001/archpsyc.60.9.929. [DOI] [PubMed] [Google Scholar]
- Kotov R, Gamez W, Schmidt F, Watson D. Linking "Big" Personality Traits to Anxiety, Depressive, and Substance Use Disorders: A Meta-Analysis. Psychological Bulletin. 2010;136(5):768–821. doi: 10.1037/a0020327. doi: Doi 10.1037/A0020327. [DOI] [PubMed] [Google Scholar]
- Krueger RF, Hicks BM, Patrick CJ, Carlson SR, Iacono WG, McGue M. Etiologic connections among substance dependence, antisocial behavior, and personality: Modeling the externalizing spectrum. Journal of Abnormal Psychology. 2002;111(3):411–424. [PubMed] [Google Scholar]
- Krueger RF, Markon KE, Patrick CJ, Iacono WG. Externalizing psychopathology in adulthood: A dimensional-spectrum conceptualization and its implications for DSM-V. Journal of Abnormal Psychology. 2005;114(4):537–550. doi: 10.1037/0021-843X.114.4.537. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Littlefield AK, Sher KJ, Wood PK. Is "Maturing out" of Problematic Alcohol Involvement Related to Personality Change? Journal of Abnormal Psychology. 2009;118(2):360–374. doi: 10.1037/a0015125. doi: Doi 10.1037/A0015125. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Martin NG, Eaves LJ. Genetical Analysis of Covariance Structure. Heredity. 1977 Feb;38:79–95. doi: 10.1038/hdy.1977.9. doi: Doi 10.1038/Hdy.1977.9. [DOI] [PubMed] [Google Scholar]
- McGue Matt, Bacon Steven, Lykken David T. Personality stability and change in early adulthood: A behavioral genetic analysis. Developmental Psychology. 1993;29(1):96–109. doi: 10.1037/0012-1649.29.1.96. [Google Scholar]
- Miller J, Flory K, Lynam D, Leukefeld C. A test of the four-factor model of impulsivity-related traits. Personality and Individual Differences. 2003;34(8):1403–1418. [Google Scholar]
- Miller MB, Basu S, Cunningham J, Eskin E, Malone SM, Oetting WS, McGue M. The Minnesota Center for Twin and Family Research genome-wide association study. Twin Research and Human Genetics. 2012;15(6):767–774. doi: 10.1017/thg.2012.62. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Regier DA, Farmer ME, Rae DS, Locke BZ, Keith SJ, Judd LL, Goodwin FK. Comorbidity of Mental-Disorders with Alcohol and Other Drug-Abuse - Results from the Epidemiologic Catchment-Area (Eca) Study. Jama-Journal of the American Medical Association. 1990;264(19):2511–2518. [PubMed] [Google Scholar]
- Robins LN, Babor TF, Cottler LB. Composite International Diagnostic Interview: Expanded Substance Abuse Module. Authors; St. Louis: 1987. [Google Scholar]
- Robins LN, Wing J, Wittchen HU, Helzer JE, Babor TF, Burke J, et al. The Composite International Diagnostic Interview. An epidemiologic Instrument suitable for use in conjunction with different diagnostic systems and in different cultures. Archives of General Psychiatry. 1988;45(12):1069–1077. doi: 10.1001/archpsyc.1988.01800360017003. [DOI] [PubMed] [Google Scholar]
- Sher KJ, Trull TJ. Personality and Disinhibitory Psychopathology - Alcoholism and Antisocial Personality-Disorder. Journal of Abnormal Psychology. 1994;103(1):92–102. doi: 10.1037//0021-843x.103.1.92. [DOI] [PubMed] [Google Scholar]
- Slutske WS, Heath AC, Madden PAF, Bucholz K, Statham DJ, Martin NG. Personality and the genetic risk for alcohol dependence. Journal of Abnormal Psychology. 2002;111:124–133. [PubMed] [Google Scholar]
- Smith GT, Fischer S, Cyders MA, Annus AM, Spillane NS, McCarthy DM. On the Validity and Utility of Discriminating Among Impulsivity-Like Traits. Assessment. 2007;14(2):155–170. doi: 10.1177/1073191106295527. doi: 10.1177/1073191106295527. [DOI] [PubMed] [Google Scholar]
- Tellegen A, Waller NG. Exploring personality through test construction: Development of the multidimensional personality questionnaire (Vol. 2) Sage; Thousand Oaks, CA: 2008. [Google Scholar]
- Vrieze SI. Model selection and psychological theory: A discussion of the differences between the Akaike Information Criterion (AIC) and the Bayesian Information Criterion (BIC) Psychological Methods. 2012;17(2):228–243. doi: 10.1037/a0027127. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vrieze SI, Hicks BM, Iacono WG, McGue M. Decline in Genetic Influence on the Co-Occurrence of Alcohol, Marijuana, and Nicotine Dependence Symptoms From Age 14 to 29. American Journal of Psychiatry. 2012 doi: 10.1176/appi.ajp.2012.11081268. doi: 10.1176/appi.ajp.2012.11081268. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vrieze SI, McGue M, Miller MB, Hicks BM, Iacono WG. Three Mutually Informative Ways to Understand the Genetic Relationships Among Behavioral Disinhibition, Alcohol Use, Drug Use, Nicotine Use/Dependence, and Their Co-occurrence: Twin Biometry, GCTA, and Genome-Wide Scoring. Behavior Genetics. 2013;43(2):97–107. doi: 10.1007/s10519-013-9584-z. doi: 10.1007/s10519-013-9584-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Whiteside SP, Lynam DR. The Five Factor Model and impulsivity: using a structural model of personality to understand impulsivity. Personality and Individual Differences. 2001;30(4):669–689. doi: http://dx.doi.org/10.1016/S0191-8869(00)00064-7. [Google Scholar]
- Widaman KF, Ferrer E, Conger RD. Factorial Invariance Within Longitudinal Structural Equation Models: Measuring the Same Construct Across Time. Child Development Perspectives. 2010;4(1):10–18. doi: 10.1111/j.1750-8606.2009.00110.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Young SE, Stallings MC, Corley RP, Krauter KS, Hewitt JK. Genetic and environmental influences on behavioral disinhibition. Am J Med Genet. 2000;96(5):684–695. doi: 10.1002/1096-8628(20001009)96:5<684::AID-AJMG16>3.0.CO;2-G [pii] [PubMed] [Google Scholar]
- Zucker RA, Heitzeg MM, Nigg JT. Parsing the Undercontrol/Disinhibition Pathway to Substance Use Disorders: A Multilevel Developmental Problem. Child Development Perspectives. 2011;5(4):248–255. doi: 10.1111/j.1750-8606.2011.00172.x. doi: 10.1111/j.1750-8606.2011.00172.x. [DOI] [PMC free article] [PubMed] [Google Scholar]