

Abstract
Background:
Menopausal health demands priority in Indian scenario due to increase in life expectancy and growing population of menopausal women. Most are either unaware or do not pay adequate attention to these symptoms.
Aims:
To find the prevalence of menopausal symptoms and perceptions regarding menopause among menopausal women of Kerala.
Settings and Design:
A community based cross-sectional house to house survey was conducted at Anjarakandy a field practice area under Kannur Medical College, Anjarakandy.
Materials and Methods:
The study was conducted among 106 postmenopausal women staying more than 6 months at Anjarakandy with the help of pretested questionnaire administered by a trained social worker from January to October 2009. Before that a pilot study was conducted and required sample size of 100 was calculated. Random sampling of houses was done.
Statistical Analysis:
Data was coded, entered, and analyzed using SPSS 15. Chi-square test, proportions, and percentages were used.
Results:
The mean age of attaining menopause was 48.26 years. Prevalence of symptoms among ladies were emotional problems (crying spells, depression, irritability) 90.7%, headache 72.9%, lethargy 65.4%, dysuria 58.9%, forgetfulness 57%, musculoskeletal problems (joint pain, muscle pain) 53.3%, sexual problems (decreased libido, dyspareunia) 31.8%, genital problems (itching, vaginal dryness) 9.3%, and changes in voice 8.4%. Only 22.4% of women knew the correct cause of menopause.
Conclusions:
Thus study stated that all the ladies were suffering from one or more number of menopausal symptoms. Ladies should be made aware of these symptoms, their causes and treatment respectively.
Keywords: Kerala, menopause, rural, survey
INTRODUCTION
Menopause is an unspoken, unattended, reality of life, the cause of which is still undeciphered completely by man. Menopause is one such midlife stage which might be overcome easily or make a lady miserable depending on her luck. This phase of life is shrouded with lots of myths and taboos.[1] Early recognition of symptoms can help in reduction of discomfort and fears among the women. World Health Organization (WHO) has defined post-menopausal women as those women who have stopped menstrual bleeding one year ago or stopped having periods as a result of medical or surgical intervention (Hysterectomy/Oophorectomy) or both.
With increasing life expectancy, women spend 1/3rd of life in this phase.[2] It is estimated that by the end of 2015 there will be 130 million elderly women in India, necessitating substantial amount of care.[3] Menopausal symptoms, though well tolerated by some women, may be particularly troublesome in others. Severe symptoms compromise overall quality of life for those experiencing them. There is under-reporting of symptoms among Indian women due to socio cultural factors.
According to literature, at least 60% of ladies suffer from mild symptoms and 20% suffer severe symptoms and 20% from no symptoms.[4] The present study was undertaken in a village called Anjarakandy Field practice area (FPA) of Kannur Medical college (KMC), located at Kannur district of North Kerala with a service approach to give health-care advice to the needy. So the current study was conducted to know the prevalence of post-menopausal symptoms at Anjarakandy village in year 2009.
MATERIALS AND METHODS
A community based prospective cross-sectional house to house survey was conducted among 106 postmenopausal women residing for more than 6 months at the FPA of KMC with the help of pretested questionnaire administered by a trained medico social worker. Study was undertaken to know the symptomatology of menopause and perception of reasons for menopause.
FPA is an area which is adopted by a Medical college for the purpose of training its medical students and interns in the Department of Community Medicine. Prior to that permission was taken from Anjarakandy Panchayat and Ethical clearance from KMC was obtained. The Malayalam (local language) questionnaire was not self-administered; the information was collected by an interview after informed written consent by a trained medico-social worker. The data collection was done for 10 months (January to October 2009) by using a structured pre tested questionnaire. The questionnaire was tested among 10 ladies in a pilot study. The sampling frame was obtained from the Panchayat office. The total houses which lodged the post-menopausal women (menopausal > 1 year) were included in the sampling frame.
Sample size was calculated by doing a pilot study on 10 ladies and prevalence of symptoms found was 80%. Furthermore, the same was found by the literature search.[4] According to the formula sample size = n = 4 pq/l2
P = 80 (crude prevalence), q = 100 – P = 20, and l = 10% of P = (Allowable error) = 8.
The required sample size was found to be 100. The sampling frame was obtained from the health workers of Anjarakandy Primary Health Centre. Systematic random sampling (no randomization but random sampling was done) of every 10th house from a list of houses that lodged the postmenopausal women was chosen.
Inclusion criteria
All post-menopausal ladies (menopause for > 1 year).
Exclusion criteria
Lady with un-natural menopause, e.g., surgical or radiotherapy for cervix cancer.
Ladies on medications such as anxiolytics, anti-depressants, to avoid treatment-related effects.
Ladies having serious disease or mental retardation.
Ladies not giving consent for the data collection due to own reasons (The response rate in the current study was 80%. Non-response was primarily due to shy attitude, no interest, or lack of time).
We have also ruled out any recent mishap/trauma in the woman's life before ascribing these symptoms to menopause. The selection bias was minimized by following the inclusion and exclusion criteria strictly. The ladies with severe symptoms were given reference slips to meet the gynecologist and the ladies with mild symptoms were given advice at primary care level.
The symptoms as told by the subjects were recorded and analyzed. The symptoms studied were broadly classified into following categories lethargy, forgetfulness, headache, musculoskeletal problems (joint pain, muscle pain), sexual problems (decreased libido), dysuria, genital problems, emotional problems (crying spells, depression, irritability, sleep disturbances), change in voice, etc.
The demographic factors studied were age, religion, education, occupation. The ladies were asked what was the cause of the symptoms according to them, whether they felt the need to visit the doctor for the symptoms, how should they clean their external genitalia, do they think that any other external factors affects the time of attainment of menopause. The lady was thought to know the correct cause of menopause if she knew that it is due to some physiological or a hormonal change that happens in the body. If a women was unable to give a scientific explanation, her knowledge about these symptoms was considered to be inappropriate. If she said it was due to God or age exclusively or due to nature/holy reason she was interrogated again since these are explanations given by lay people and cannot be considered entirely incorrect. If a lady used soap and water to clean the external genitalia and also dried it properly with a clean cloth after cleaning she was considered to have adequate knowledge regarding the hygiene of the external genitalia. We also asked them if they knew that their symptoms could be possibly controlled by hormone replacement therapy (HRT).
Statistical analysis
Data was coded, entered, and analyzed using SPSS 15. Chi-square test, proportions, and percentages were used.
Findings
Total 106 women were studied. The current study, which was undertaken to understand the symptomatology of menopause and perception of reasons for menopause shows that the mean age of the study subjects was 56.7 years and standard deviation (SD) was 8.514. The age of the study subjects ranged from 32 years to 82 years. The mean duration since stoppage of menstruation was 8.45 years and SD was 6.91. The mean age of subjects at menopause was 48.26 years with a SD of 4.86 years. The mean number of symptoms that a lady suffered from ranged from 4.94 years and SD of 2.07 years.
Table 1 shows that in the current study setting the community is well educated, but most ladies are unemployed.
Table 1.
Demographic characteristic of the study subjects
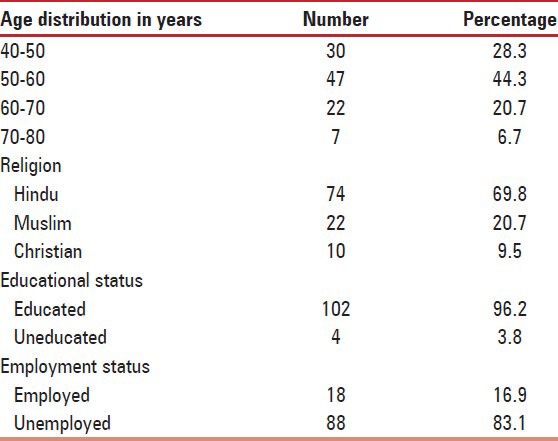
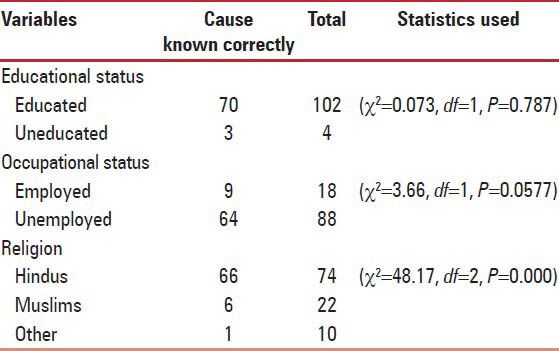
Table 2 shows that there was no statistically significant difference between the educational status and the correct cause of menopause known by the subject (Chi-square value (χ2 = 0.073, df = 1, P = 0.787). There was no significant difference between employment status and correct cause of menopause as stated by the women (χ2 = 3.66, df = 1, P = 0.057). There is a statistically significant association between the religion and the cause of menopause correctly known. (χ2 = 48.817, df = 2, P < 0.01). More number of Hindu subjects knew the correct cause as compared to Muslims and others. Study with a higher sample size could be useful in providing any further comment on the effect of religion in the current situation.
Table 2.
Relationship between the variables and cause of menopause correctly known
Common symptoms that the study subjects suffered were emotional problems (crying spells, depression, irritability) 90.7%, headache 72.9%, lethargy 65.4%, burning micturition 58.9%, forgetfulness 57%, musculoskeletal problems (joint pain muscle pain) 53.3%. The three most common symptoms in age < 50 years were emotional symptoms, headache, and sexual problems. The 50-60 years old complained of emotional problems, lethargy, and dysuria. The subjects > 60 years complained of emotional problems, forgetfulness, and headache. None of the ladies had ever heard of any HRT but 70% had heard of calcium supplements which could be used in old age. One of the reasons for these complaints could be co-morbidities like hypertension, diabetes, etc., but we did not investigate for them in the current study.
Table 3 shows that there is a statistically significant association between the mean number of menopausal symptoms and number of years of stoppage of menses. The number of symptoms increases as the number of years of stoppage of menses increases.
Table 3.
Years of stoppage of menses and symptoms
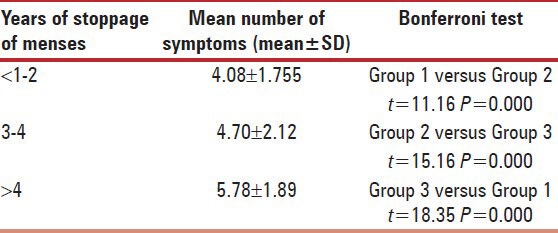
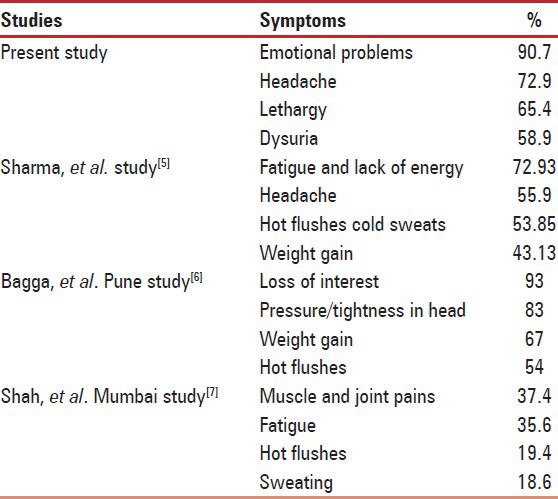
Table 4 Prevalence of four most common menopausal symptoms of the present study and compares it with that reported in the other studies done in India.
Table 4.
Prevalence of four most common menopausal symptoms of various studies done in India
22.4% of ladies thought that the main reason for menopause was due to God. The subjects were interrogated again since these are explanations given by lay people and cannot be considered entirely incorrect. 9.3% did not know any specific reason for menopause. The others (69%) knew that the reason was due to physiological hormonal changes that occur in the female which leads to menopause. 11.2% did not feel any need to clean the external genitalia since they thought that menses had stopped by now. 52.3% used to clean it with plain water. Only 36.5% knew the exact way to clean the external genitalia. 22.4% did not feel any need to visit a doctor for the complaints since they thought it was not possible to treat these symptoms.
Hot flushes and night sweats are common menopausal symptoms but were not reported by the study subjects in our current study setting.
DISCUSSION
Ageing is a reality of human existence on mother earth which nobody can escape. The quest to understand the secrets of ageing dates back to the dawn of civilization and reflects strongly the human desire to increase life expectancy and perpetuate an everlasting youthful look. The current study undertaken to know the symptomatology of menopause and perception of reasons for menopause, states that there was no statistically significant difference between correct cause of menopause as stated by the women and the educational or employment status. Religion was significantly associated with the knowledge of the correct cause. More number of Hindu subjects knew the correct cause as compared to Muslims and others. The possible reason for this finding could be educational status of Hindu ladies which was found to be higher than the Muslim ladies. Such findings should be definitely proved with a stronger research study. In developing countries the mean age of menopause is 44-45 years as compared to developed countries where the figures are slightly on a higher side.[5] The present study found the mean age at menopause to be 48.26. This might be due to regional differences, environmental factors, and genetic factors. Kerala is a developed state of India so the age of onset may be slightly on the higher side compared to the Indian setting. The Menopause-specific quality of life (MEN-QOL) is self-administered and consists of a total of 29 items in a Likert scale format. Each item assesses the impact of one of the four domains of menopausal symptoms, as experienced over the last month (vasomotor, psychosocial, physical and sexual). Items pertaining to a specific symptom are rated as present or not present and if present how bothersome on a zero to six scale. In the current study, we used a questionnaire, which could only enlist the complaints told by the lady itself. We did not use a standard validated questionnaire like the MENQOL due to feasibility reasons.
Qualitative research technique as conducted by Saka et al., (2012) Nigeria[8] using Focus group discussion is a better study design but due to resource constraints we did not go for that design in our current study.
In the study done by Mehershi, et al., (2010), 85% of Gynecologists from Jaipur in Rajasthan prescribed hormonal replacement therapy to their patients. There was a great disparity in their minds too whether to prescribe HRT or not.[9] There is a huge debate over the interpretation of the findings of the Women's health initiative study. It was stated in 2007 that age is one of the major factors in prescription of HRT. The target population was unanimously considered to be women below 55 years of age. HRT initiated at the early post-menopausal period in healthy women is safe.[10] Hormonal therapy is known to be a standard line of treatment for vasomotor symptoms of moderate to severe degree, vaginal atrophy, and osteoporosis. Recently, it is found that there is a chance of development of cardiovascular disease and Alzheimer's disease due to hormonal replacement. The current study has found that 22.4% did not feel any need to visit a doctor for these complaints. They thought that the complaints would subside on its’ own by passage of time. According to the authors, this was the greatest misunderstanding they had.
In the study done by Ominder et al., (2011) in Amol, Iran the frequency of dyspareunia was 55.6%. In the current study, the prevalence was found to 31.8%.[11] Reasons for this difference are unknown. The authors predict that this could have been due to shy and embarrassing attitude of post-menopausal ladies towards sexuality in the current study setting.
In the study done at Udipi by Bairy, et al., (2009),[12] 352 post-menopausal women attending the out-patient clinics in a tertiary care hospital in South India, were included in the study. There was a high prevalence of aching in muscles and joints (67.7%), feeling tired (64.8%), poor memory (60.5%), lower backache (58.8%), feeling bloated (55.1%), and difficulty in sleeping (51.7%) among the menopausal respondents. The MEN-QOL questionnaire was used in this study. Many elderly ladies might have approached any other health service institutions nearby for their complaints. The findings of the current community based study can be generalized to the whole village around KMC. Due to feasibility problems we gave up the idea of using a MENQOL questionnaire in community settings.
Puri (2008)[13] conducted a study to ascertain the knowledge about menopause and post-menopausal bleeding in women of urban and slum area of Chandigarh, India. The most common menopausal symptom was vaginal irritation/discharge (42.7%). Less than half of females (38.7%) ever took treatment for menopausal symptoms. Calcium supplements were taken by majority 63%. In the current study, knowledge regarding calcium supplements was observed among 70% of ladies.
Many prevalence studies have been done in the world regarding this topic. The few ones are as follows. Lu, et al., (2007),[14] conducted a cross-sectional survey in Australia among 197 Arabic women aged 45-65 years. The median age at menopause in this study was 49 years. Out of 29 symptoms, the most frequent symptom reported was “feeling tired or worn out” (86%), followed by “aching in muscles and joints” (85%). Peeyananjarassri (2006),[15] conducted a survey among 270 women aged 45-65 years who attended the gynecological and menopause clinic, Songklanagarind Hospital. The average age at menopause of the post-menopausal women was 48.7 years (range 40-57 years). The prevalence of the classical menopausal symptoms–hot flushes, night sweats, and vaginal dryness – in the women aged 45-65 years were 36.8%, 20.8%, and 55.3%, respectively. In the current study, the most common symptoms found were emotional problems 90.7%, headache 72.9%, lethargy 65.4%, and dysuria 58.9%.
Mahajan, et al.,[16] did a study in North India regarding health issues of menopausal women and found that mean number of symptoms was found to be increasing linearly with rising age of the study subjects. They have also mentioned about a report by WHO, which states that hot flushes are prevalent more in European and North American populations as compared to Asians. In the current study, no lady has reported hot flushes or night sweats as post-menopausal symptoms. This may be due to misinterpretation or inappropriate concealment of information by the ladies. It should not be misinterpreted as absence of hot flushes or night sweats among women of Kerala.
CONCLUSIONS
The current study, thus, attempted to know the symptomatology and perception of reasons for menopause. It clearly states that the prevalence of post-menopausal symptoms is definitely high among women in the current study setting. There are many misunderstandings regarding menopausal symptoms among the rural women in Kerala (who are the most educated in India). Such studies help in creating awareness since disseminating health education for postmenopausal women is of prime importance. Women's clinic might be a good idea. Health workers may be most fruitful in this area. Further research studies to assess the severity of the symptoms using a standard field tested and simple scales should be done in the community setting.
Limitations
The prevalence of hot flushes and night sweats, which are important and debilitating symptoms have not been reported by women in the current study setting. This could be due to misinterpretation of symptoms and a shy attitude.
ACKNOWLEDGMENT
Ms. Divya - Medico social worker, Ms. Suchitra K. Rajappan - Statistician, Kannur Medical College, Anjarakandy, and for help provided.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Kulshreshtha B, Ammini A. Hormone replacement therapy. In: Sharma OP, editor. Geriatric care: A textbook of geriatrics and gerontology. 3rd ed. New Delhi: Viva Books Publishers; 2008. pp. 647–50. [Google Scholar]
- 2.Vaze N, Joshi S. Yoga and menopausal transition. J Midlife Health. 2010;1:56–8. doi: 10.4103/0976-7800.76212. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Mishra N, Mishra VN, Devanshi Exercise beyond menopause: Dos and don’ts. J Midlife Health. 2011;2:51–6. doi: 10.4103/0976-7800.92524. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Tumbull S. Yoga as a treatment for menopausal symptoms. J Yoga Ontogenet and Therap Investig. 2010;2:14–5. [Google Scholar]
- 5.Sharma S, Tandon VR, Mahajan A. Menopausal symptoms in urban women. JK Science. 2007;9(1):13–7. [Google Scholar]
- 6.Bagga A. Age and symptomatology of menopause: A case study. Obstet and Gynecol Today. 2004;10:660–6. [Google Scholar]
- 7.Shah R, Kalgutkar S, Savardekar L, Chilang S, Iddya U. Menopausal symptoms in urban Indian women. Obstet and Gynecol Today. 2004;11:667–70. [Google Scholar]
- 8.Saka M, Saidu R, Jimoh A, Akande T, Olatinwo A. Behavioral pattern of menopausal Nigeria women. Ann Trop Med and Public Health. 2012;5:74–9. [Google Scholar]
- 9.Mehersihi S, Khandelwal S, Swarankar M, Kaur P. Attitudes and practices of gynecologists in Jaipur towards management of menopause. J Midlife Health. 2010;1:74–8. doi: 10.4103/0976-7800.76216. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Pines A. Guidelines and recommendations on hormone replacement therapy in menopause. J Midlife Health. 2010;1:41–2. doi: 10.4103/0976-7800.66990. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Omidvar S, Bakouie F, Amiri FN. Sexual function among married menopausal women in Amol (Iran) J Midlife Health. 2011;2:77–80. doi: 10.4103/0976-7800.92534. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Bairy L, Shalini A, Bhat P, Bhat R. Prevalence of menopausal symptoms and quality of life after menopause in women from South India. Aust N Z J Obstet Gynaecol. 2009;49:106–9. doi: 10.1111/j.1479-828X.2009.00955.x. [DOI] [PubMed] [Google Scholar]
- 13.Puri S, Bhatia V, Mangat C. Perceptions of menopause and postmenopausal bleeding in women of Chandigarh, India. [Last accessed on 2013 Jan 01];Internet J Fam Pract. 2008 6(2):1–6. [Google Scholar]
- 14.Lu J, Liu J, Eden J. The experience of menopausal symptoms by Arabic women in Sydney. Climacteric. 2007;10:72–9. doi: 10.1080/13697130601159649. [DOI] [PubMed] [Google Scholar]
- 15.Peeyananjarassri K, Cheewadhanaraks S, Hubbard M, Zoa Manga R, Manocha R, Eden J. Menopausal symptoms in a hospital-based sample of women in southern Thailand. Climacteric. 2006;9:23–9. doi: 10.1080/13697130500487422. [DOI] [PubMed] [Google Scholar]
- 16.Mahajan N, Aggarwal M, Bagga A. Health issues of menopausal women in North India. J Midlife Health. 2012;3:84–7. doi: 10.4103/0976-7800.104467. [DOI] [PMC free article] [PubMed] [Google Scholar]