

Stakeholder engagement is critical in the development of a new program intervention.1–3 Focus groups2 or interviews4 are traditional data collection strategies typically used for this process. The persona-scenario exercise, an alternative to traditional strategies, originated from the field of human computer interface design.4–6 This article describes how persona-scenario exercises were applied in the codesign of the complex primary care intervention TAPESTRY (Teams Advancing Patient Experiences: Strengthening Quality). (For more information on TAPESTRY, visit www.healthtapestry.ca). The goal of the TAPESTRY program is to determine how health care teams can be more responsive to the needs of our aging population. The program involves trained community volunteers reaching out to older adults in their homes to assess their health needs. Volunteers will be linked to patients’ health care teams using technology, which will improve communication with providers and will also maximize engagement with community service providers.
The persona-scenario exercise is a structured approach that asks participants to create a fictitious, authentic “persona” based on guiding questions (eg, What is your name, age, and sex? What is your experience with intervention components?). Personas should characterize the stakeholder group that participants represent (eg, primary care provider, patient). Participants use their personas to create the potential intervention (the scenario) using another set of guiding questions (eg, How does the person get involved in the program? What are the volunteers, patients, and providers doing in the scenario? How are they interacting?).
Scenarios allow for “multiple views of an interaction” and “diverse kinds and amounts of detailing.”5 This does not happen by using focus groups, in which participants take turns responding to guided questions based on past experiences and their context.
The persona-scenario exercise has several potential advantages. It allows participants to use their own experiences and perceptions to help guide the development of complex interventions through the personas and scenarios that they create. In program development, in which some intervention elements are not known and incorporation of stakeholder opinion is vital, this method helps introduce the program components and identify potential interactions between them.
Methods
We used the persona-scenario exercise to engage stakeholders in codesigning the health service intervention TAPESTRY. The following is a discussion on the group facilitation and analysis for the 13 persona-scenario sessions that took place to design the program.
Group facilitation
The persona-scenario exercise was conducted with patients, health care providers, volunteers, and community service agency staff. Sessions were conducted with participants of a single stakeholder group. Each group received a tailored discussion guide and an introduction to the program components (volunteers, electronic health records, community services, interdisciplinary teams). Participants were told that the goal of the exercise was to create a detailed and realistic character that represented their stakeholder group (ie, the persona) and to have that persona experience all aspects of TAPESTRY (ie, the scenario), stressing that they had the freedom to be creative beyond the health care system as they knew it.
Participants were divided into pairs. Each pair of participants typically created one persona and one scenario; however, if time allowed, they could create another scenario with their personas. Pairs described their personas and scenarios to the group, and this summary was audiorecorded—unlike in focus groups, in which the entire discussion is recorded. After using various combinations of working group sizes, we found that paired participants worked best. Ideally, having no more than 4 pairs allowed for enough time for each pair to present their personas and scenarios to the group, and also resulted in a manageable participant-to-facilitator ratio. We recommend that pairs share similar backgrounds, such as age or experience level, so that personas represent more authentic characters. For example, less experienced volunteers should not be paired with more experienced volunteers because they are unable to create personas as realistic as those of the more experienced volunteers. Having tested several configurations, we found that, ideally, each pair should have a note-taker who is not participating in the discussion to write down key points using a laptop or pen and paper. This helped participants to speak freely and work through ideas without losing time to write their answers, and allowed note-takers to facilitate conversation. Using research staff as note-takers to clearly write out participants’ answers to each question enhanced the sharing of information with the larger group and improved the quality of audiorecordings. Note-takers must feel comfortable in clarifying questions and giving directions regarding pacing, staying on topic, and fully completing the exercise. Ideally, the exercise should last no more than 2 hours (10 minutes for instruction and consent; 10 minutes per persona; 25 to 30 minutes per scenario; and 8 to 10 minutes for each pair to report back to the group).
Analysis
Summaries of the persona-scenario exercises that were presented by participants or note-takers were transcribed verbatim and coded in NVivo, version 10.7 Three researchers (R.V., K.N., and J.L.) coded a transcript together to create the coding structure. Two authors (K.N., J.L.) independently completed the open coding8 process; few new ideas emerged after 13 sessions, indicating data saturation. A list of highly descriptive and self-explanatory nodes was generated. These were organized by program components under broad headings, exported to Excel, and formatted into a table with columns for nodes, actions, and items. Each node was assigned specifications (ie, actions that were required to actualize the ideas and items that were required to execute the actions) to be implemented (Table 1). Two research team members (K.N., J.L.) independently reviewed each node (investigator triangulation) to ensure that multiple perspectives were incorporated during analysis, increasing rigour.9 Once the table with actions and items was generated, it was reviewed to determine what already existed in the program, what was unfeasible, and what needed to be developed. Finally, a program to-do list was created (Figure 1). The action and item specifications that were generated from the nodes formed the basis of program development.
Table 1.
A sample of coding and analysis from the persona-scenario exercise to determine program specifications
| QUOTE FROM PARTICIPANT WHILE DISCUSSING THE PROGRAM COMPONENT OF VOLUNTEER | NODES |
SPECIFICATIONS
|
|
|---|---|---|---|
| ACTIONS | ITEMS | ||
| “We see the role for the volunteers being the information gatherer. But the volunteer really does need to communicate with the physician too. And this could be through electronic means, giving feedback to the physician and the physician will ultimately make the decision about whether an appointment is needed and inform either the patient or the volunteer” (Scenario 1, Patient Group 1) | Volunteer acts as an information gatherer and communicates patient information to the physician who makes the decisions | Integrate a functional application that gathers information directly into the electronic medical record Train volunteers on how to gather information |
|
| Volunteer provides information to the physician electronically | Volunteer sends electronic updates using the application to the clinical team weekly, monthly, or after each visit |
|
|
| Physician receives volunteer information electronically and decides whether an appointment is needed | Physician uses volunteer assessment information |
|
|
Figure 1.
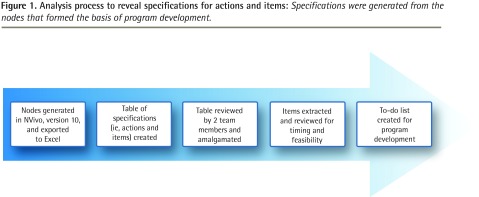
Analysis process to reveal specifications for actions and items: Specifications were generated from the nodes that formed the basis of program development.
Benefits
Based on our reflection and the feedback we received from participants, there were many benefits to using the persona-scenario exercise. Early engagement with key stakeholders helped foster support and uptake of the pilot program. One participant said, “This scenario actually gets me excited about the potential of [the TAPESTRY program].” Participants (potential future users of the program) also introduced many novel ideas that were not identified by the research team.
Challenges
Conducting the persona-scenario exercise was resource-intensive. It required a facilitator and multiple note-takers for each group (up to 5 people) and laptops for note-takers. Another challenge was the number of participants in each group. Because it was best to have participants work in pairs and each pair reported back to the group, time constraints limited group size per session. Groups with fewer than 4 participants led to different challenges, such as 3 people with different backgrounds having to collaborate, potentially resulting in less authentic personas. Finally, while persona-scenario exercises are best suited for a range of people commenting on various components of a program, some participants might be less informed about certain components and might develop scenarios that are not feasible.
Conclusion
The persona-scenario exercise is an innovative alternative to traditional focus groups, and it is a useful strategy to use for the development of a primary care program intervention by engaging stakeholders in its codesign.
Acknowledgments
The research team, as part of the TAPESTRY project, received funding from Health Canada.
Hypothesis is a quarterly series in Canadian Family Physician, coordinated by the Section of Researchers of the College of Family Physicians of Canada. The goal is to explore clinically relevant research concepts for all CFP readers. Submissions are invited from researchers and nonresearchers. Ideas or submissions can be submitted online at http://mc.manuscriptcentral.com/cfp or through the CFP website www.cfp.ca under “Authors and Reviewers.”
Footnotes
Competing interests
None declared
References
- 1.Edwards N, Roelofs S. Participatory approaches in the co-design of a comprehensive referral system. Can Nurse. 2005;101(8):20–4. [PubMed] [Google Scholar]
- 2.Bate P, Robert G. Experience-based design: from redesigning the system around the patient to co-designing services with the patient. Qual Saf Health Care. 2006;15(5):307–10. doi: 10.1136/qshc.2005.016527. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Ellis DR, Kurniawan SH. Increasing the usability of online information for older users: a case study in participatory design. Int J Hum Comput Interact. 2000;12(2):263–76. [Google Scholar]
- 4.Reeder B, Turner AM. Scenario-based design: a method for connecting information system design with public health operations and emergency management. J Biomed Inform. 2011;44(6):978–88. doi: 10.1016/j.jbi.2011.07.004. Epub 2011 Jul 23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Carroll JM. Five reasons for scenario-based design. Interact Comput. 2000;13(1):43–60. [Google Scholar]
- 6.Idoughi D, Seffah A, Kolski C. Adding user experience into the interactive service design loop: a persona-based approach. Behav Inf Technol. 2012;31(3):287–303. [Google Scholar]
- 7.NVivo, version 10 [computer software: qualitative data analysis program] Cambridge, MA: QSR International; 2013. [Google Scholar]
- 8.Miles MB, Huberman MA. Qualitative data analysis. An expanded sourcebook. 2nd ed. Thousand Oaks, CA: Sage Publications; 1994. [Google Scholar]
- 9.Golafshani N. Understanding reliability and validity in qualitative research. Qual Rep. 2003;8(4):597–607. [Google Scholar]