

Version Changes
Updated. Changes from Version 1
We have attempted to address and incorporate most of the concerns that were raised by the reviewers about the previous version of our manuscript. The reviewers generally felt that the method of selecting the respondents for the ethno-botanical survey was not clearly explained and might be construed to be biased. In our update we explain that we interviewed a total of 9 respondents with 3 focal/key ones with whom we went out on field excursions to identify and collect medicinal plant specimens, and another 6 (2 from each forest block, chosen randomly and did not join the excursions). Two of the respondents were female but all were elderly, chosen with advice and guidance from local leaders and field assistance. We also clarify that we mainly collected information about indigenous medicinal plants rather than comparing or analyzing local opinion about these plants. We also provided more background information and citations regarding medicinal plant research in Kenya and East Africa, which was scanty in the previous version, and put our own results into the perspective of these studies. We elaborated on our choice of classification criterion for diseases treated by the medicinal plants, including justification for the group "vector-borne" for the purpose of highlighting the very common diseases in east Africa such as malaria. We provided further postulations, based on other studies and background information, on why digestive-related diseases appeared predominant in local treatments using medicinal plants. Further, we incorporated the various changes and other comments suggested by the reviewers, including removing some repeated illustrations; writing the conclusions and recommendations more substantively to tie closely with the results; declaring how ethical issues about intellectual property rights were addressed and revising some taxonomic information that we had earlier got wrong or was missing.
Abstract
Kakamega forest is Kenya’s only rainforest and is distinguishably rich in biodiversity but threatened by agricultural encroachment and other forms of human activity. It is also one of Kenya’s Important Bird Areas and a significant source of natural products to neighboring rural communities, such as medicinal plants, food, wood and other fibers. By using structured questionnaires for direct interviews, local indigenous knowledge was tapped through involvement of a focal group of elderly key informants in three blocks of the forest. Forty key species of medicinal plants used by local people were identified and recorded. Fifty-five percent of these were shrubs, thirty-two percent trees, seven-and-a-half percent lower plants such as herbs or forbs while five percent were climbers. About seventy percent of the medicinal plants occurred inside the forest itself and thirty percent around the edge and the immediate surroundings outside the forest. Thirty-eight (95%) of the plants were indigenous to Kenya and two (5%) exotic. Such extensive indigenous knowledge of the medicinal uses of the plants, including their distribution trends in the forest, may be tapped for decision support in rural health service planning, policy formulation for conserving the forest, tracking and mitigation of climate change impacts.
Introduction
Although community development goals are not always consistent with biodiversity conservation objectives 1 there are often many opportunities for mitigating negative effects by tapping into local indigenous knowledge with reference to certain aspects of environmental use and conservation 2. Indeed, application of knowledge and values of communities that are resident within or around key biodiversity areas has been gaining increasing global popularity as significant elements in enriching and improving strategies for conserving biodiversity 2. This is because integration of such indigenous knowledge into conservation programs facilitates cross-borrowing of ideas, promotes constructive engagement, and instills a sense of common ownership and responsibility towards achievement of a synergy of goals 3. This echoes the concept of social capital 3 that, apart from amassing local support and goodwill, adoption of local indigenous knowledge in conservation may also promote and provide sustainable insurance against conflicts of purposes. This results in increased chances of achieving the dual goal of biodiversity conservation stewardship as well as community development. For instance, studies have shown that rainforest ethno-botanical checklists prepared by communities living in or near them tend to be more exhaustive because they are based on practical day-to-day uses that are firmly ingrained in local cultural norms and values 3– 5.
Like in many parts of the developing world, there is a growing upsurge in demand for herbal and other traditional remedies for various ailments among communities in Kenya. This is due either to the increasing cost of conventional modern medicine or, inadequacies in public health service delivery 6. For a long time, the bulk of “technical” information on traditional plant uses in the treatment of disease has been disparate and privately held, with limited accessibility to the public or peer-review domain 7, 8. Fortunately, over the past five years there has been an upsurge in research and publication on indigenous knowledge and use of medicinal plants in Kenya. This includes research on medicinal plants of the Nandi forest 9, indigenous knowledge on medicinal plants of Mt. Elgon forest 10 and the uses of medicinal plants by the Ogiek people of the East Mau forest 11. As a result, a firmer foundation is being laid gradually but steadily for further research into the effectiveness of these treatments and the various options for preparation and administration for managing diseases.
This study sought to set in motion a process for systematic documentation of plants of medicinal value in the Kakamega forest, with a view to consolidate indigenous knowledge about them and making this information available to the wider community. It is hoped that in the process of this, ecosystem and other socio-economic services offered by the Kakamega forest will be highlighted. The study also sought to highlight any plant species in the forest that may have medicinal value that are also of conservation concern, either as endangered or as invasive species.
Materials and methods
Study area: The Kakamega forest lies in western Kenya between 00°08′30.5′′ – 00°23′12.5′′ N and 34°18′ 08′′ – 34°57′26.5′′ E from 1520–1680 m above sea level 12– 14 ( Figure 1). The mean annual rainfall is 2000 mm, with long rains in April/May and short rains in September/October 12, 13, while the mean annual temperature is 20°C. The forest covers 183 km 2 and 100 km 2 of this consists of closed canopy forest of which one-third, in the north, is gazetted as a national reserve under protection. The rest is comprised of grassy and bushed glades, tea, cultivation and plantations of softwoods and commercially valuable hardwoods 14, 15.
Figure 1. Map of Kakamega forest (this figure has been reproduced with kind permission from Otieno and co-authors 13).
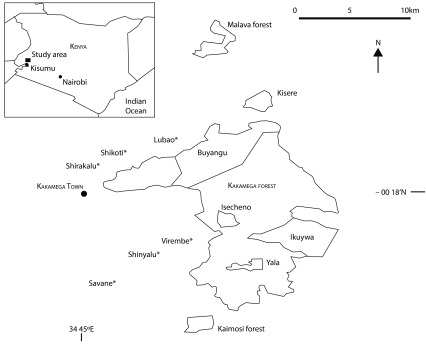
The forest is Kenya’s only true tropical rainforest 14 and constitutes one of Kenya’s 61 Important Bird Areas (IBAs) due to the presence of about 350 bird species, many of which are range-restricted or endemic species reminiscent of the wider Guineo-Congolean forest system that extended from the eastern Democratic Republic of Congo, of which Kakamega is the easternmost outlying relict 15. There are at least 380 plant species, though there is no significant endemism. As a result of massive exploitation through massive legal and illegal logging between the 1960s and 1990s, the forest flora is dominated by a mixture of large secondary-growth trees and hardly any primary-growth trees. Even for this secondary forest, much of the closed canopy and contiguity exists only in the northern part of the forest, consisting of the Buyangu blocks, which are now protected as a national wildlife reserve. The southern end, comprising of the Isecheno, Yala and Ikuywa as well as the detached units of the Kisere, Kaimosi and Malava blocks ( Figure 1), are managed as forest reserves but are still accessible to the local public community despite some level of official restriction.
Apart from birds and plants, the forest also has a remarkable richness in other biodiversity including several species of mammals, reptiles, amphibians and invertebrates 16.
The forest is under an increasing threat of loss to agriculture and settlement by the increasing local human population. The neighbourhood of the forest, where the western Kenya Bantu ethnic community called the Luhya reside, is densely populated with an average density of 433 persons per square kilometer 17, 18.
The study was carried out within the three main blocks of the southern Isecheno-Yala-Ikuywa blocks, Buyangu, and the detached Kisere and Kaimosi blocks in the north (see Figure 1). The blocks were covered in two field seasons of 11 days each, the first between April and May 2009 while the effects of the wet season were still evident and many plants bore fruit and then in late July during the dry season when full fruiting is reduced and some leaves are shed off. This was to control for any rainy-season effects.
Sampling strategy: A key informant was identified from each study block during each sampling week, to be interviewed about the medicinal plants as outlined by Kothari 19. The choice of blocks was primarily to achieve sampling with as much coverage of the forest as possible (including protected areas, reserves and detached fragments) though not necessarily to sample in every spatial part of the forest. Key informants were selected on the following criteria: (1) seniority of age in the community (not less that 50 years old); (2) local residency for a period of not less than 20 years; (3) knowledge of forest plants in the local dialect and well versed with their use(s). Current or previous experience as herbalist was preferable but not essential.
The selection was based on prior consultation with the local community leaders and additional guidance by field assistants according to Okello et al. 10 and prior consent was obtained before interviews. One of the key informants engaged in the interviews was a practicing traditional healer. Further information was obtained from random opportunistic interviews with 6 other non-core informants who were also at least 50 years old, 2 from each block. The choice of elderly informants was made on the basis that most indigenous knowledge about traditional medicine in developing countries tends to be possessed by elderly members of the society 20.
Data was collected from key informants through field excursions using direct personal interviews that employed the use of a structured questionnaire guided by a mix of closed and open-ended questions (see survey questionnaire). This was combined with free-style discussions and field excursions with the informants. For data consistency, the same informants were involved in each sampling season in each area. In addition, there was a final joint focused group discussion with all the key informants to synergize the information gathered. Information captured and recorded included:
1) Local name of plant in question; 2) Disease/condition treated by plant; 3) Plant part(s) used for the treatment; 4) Preparation method; 5) Indidgenous, common (English) and scientific name of the plants. These were determined by consulting illustrated standard botanical field guides 7.
The questionnaire provided to local informants to identify local medicinal plants
Data analysis
A checklist of all recorded species of medicinal value was compiled, including their indigenous, common and scientific names, plant origination (i.e. indigenous or exotic), plant form (e.g. tree, shrub, herb etc.) and conditions treated ( Table 1 and data set). Data was also presented in terms of the methods of preparation and administration to patients; as well as the age group and gender of target patients (data file below). All the lists generated by the different key informants were scrutinized and synchronized into a final list at the joint focused group discussion 20. With help from the informants/respondents, each plant was observed in its natural habitat and a image taken using a digital camera, collected and pressed. For each medicinal plant, a small part (preferably one with flowers) was collected while fresh and digitally photographed for identification and pressed for herbarium. Species whose common (English) and scientific names were not immediately established in the field were taken for specialized identification at the EA Herbarium at the National Museums of Kenya in Nairobi.
Table 1. Checklist of the medicinal plants identified in and around Kakamega forest species accounts.
| Scientific name | Local name | Common name | Family | Plant origin | Plant form | Diseases or conditions
targeted |
|---|---|---|---|---|---|---|
| Albizia grandi bracteata | Mukhunzuli | Large-leaved Albizia | Fabaceae | Indigenous | Tree | Gonorrhea |
| Albizia gummifera | Musenzeli | Peacock flower | Fabaceae | Indigenous | Shrub | Sexually transmitted infections
Stomach-ache |
| Azadirachta indica | Muarubaini | Neem tree | Meliaceae | Exotic | Tree | Fever, aches, pains
Malaria attack Insect bites Pest control Skin infections |
| Aspilia pluriseta | Shralambila | Dwarf Aspilia | Asteraceae | Indigenous | Herb/forbe | Stopping bleeding in wounds
Drippy nose in poultry |
| Bequartiodendron oblanceolata | Musamia | Not established | Not established | Indigenous | Tree | Ulcers in digestive track
Boils around belly |
| Chrysocephalum sp | Mwikalo | Yellow Buttons | Asteraceae | Indigenous | Shrub | Stomach problems related to STIs |
| Clematopsis scabiosifolia | Lunyili | Not established | Ranunculaceae | Indigenous | Climber | Stuffy nose and associated respiratory problems |
| Clerodendron pygmaeum | Luseshe | Cashmere Bouquet | Verbenaceae | Indigenous | Shrub | Common flu and associated |
| Coffea eugenioides | Itikwa | Mufindi coffee | Rubiaceae | Indigenous | Shrub | Eye problems in livestock |
| Conyza floribunda | Liposhe | Asthma weed | Asteraceae | Indigenous | Shrub | Tooth-ache |
| Desmodium adscendens | Matite | Not established | Fabaceae | Indigenous | Herb/forbe | Stomach-ache |
| Desmodium repandum | Not established | Not established | Fabaceae | Indigenous | Shrub | Stomach upset |
| Diospyros abyssinica | Lusui | Giant Ebony | Ebenaceae | Indigenous | Tree | Recurrent nightmares
Sores |
| Dissotis speciosa | Lunyili | Not established | Melastomataceae | Indigenous | Shrub | Diarrhea |
| Dovyalis macrocalyx | Shinavatevia | Shaggy-fruited dovyalis | Flacourtiaceae | Indigenous | Shrub | Constipation
Peptic ulcers |
| Entada abyssinica | Shivayamboga | Abyssinia Entada | Leguminoceae | Indigenous | Tree | Stomach-ache |
| Erythrococca atrovirens | Shirietso | Not established | Euphorbiaceae | Indigenous | Shrub | Wounds, especially septic |
| Hibiscus sp | Lubulwa | Not established | Malvoideae | Indigenous | Shrub | Stomach-ache
General fever |
| Justica flava | Lihululwa | Yellow Justicea | Acanthaceae | Indigenous | Herb/forbe | Reducing post-natal pains |
| Lantana trifolia | Imbulimutacha | Three-leaf Shrub | Verbenaceae | Indigenous | Shrub | Malaria and general fever (humans)
Diarrhea in livestock |
| Leucas calostachys | Lumetsani | Not established | Lamiaceae | Indigenous | Shrub | Severe diarrhea especially accompanied with blood |
| Leucas deflexa | Shitsunzune | Not established | Lamiaceae | Indigenous | Shrub | Eye infection/effects in livestock |
| Markhamia lutea | Lusiola | Nile Tulip tree | Bignoniaceae | Indigenous | Tree | Ear pain in humans
Eye problems in cattle |
| Mondia whytei | Mukomer | White’s ginger | Apocynaceae | Indigenous | Climber | Loss of appetite
Low libido Fatigue Mineral deficiency |
| Ocimum kilimandscharicum | Not established | Kilimanjaro basil | Lamiaceae | Indigenous | Shrub | Nasal congestion, colds, flu,
Insect bites General aches and pains |
| Olea capensis | Mutukhuyu | Elgon Olive | Oleaceae | Indigenous | Tree | Stomach-ache
Peptic ulcers |
| Paullinia pinnata | Not established | Bread and cheese plant | Sapindaceae | Indigenous | Shrub | Hiccup |
| Paulownia tomemtosa | Musembe | Foxglove tree | Paulowniaceae | Exotic | Tree | Stomach problems
Boils |
| Piper capense | Not established | Staart Pepper | Piperaceae | Indigenous | Shrub | Cough |
| Piper umbellatum | Indava | Cow-foot leaf | Piperaceae | Indigenous | Shrub | Head-ache and fever |
| Plectrantus forsteri | Shikhokho | Spur flower | Lamiaceae | Indigenous | Shrub | Worm infection in livestock |
| Prunus africana | Mwiritsa | Red Stinkwood | Rosaceae | Indigenous | Tree | Prostate cancer
Stomach-ache |
| Rhus natalensis | Busanguli | Desert date | Anacardiaceae | Indigenous | Shrub | Worm infections in humans and livestock |
| Sapium ellypticum | Musasa | Jumping seed tree | Euphorbiaceae | Indigenous | Tree | Eye problems in livestock such as by injury or infection |
| Senecio moorei | Not established | Not established | Asteraceae | Indigenous | Shrub | Cough |
| Solanum incanum | Indalandalwa | Sodom Apple | Solanaceae | Indigenous | Shrub | Stomach-ache |
| Thunbergia alata | Indereresia | Black-eyed Susan vine | Acanthaceae | Indigenous | Shrub | Joint dislocation in both humans and livestock |
| Toddalia asiatica | Not established | Orange climber | Rutaceae | Indigenous | Shrub | Worms in cattle |
| Trichilia emetica | Munyama | Banket mahogany | Meliaceae | Indigenous | Tree | Fever
Stomach-ache Sexually transmitted infections Malaria |
| Zanthoxyllum gilleti | Shikhoma | Not established | Rutaceae | Indigenous | Tree | Cough and chest complications associated with bacterial infection |
Results and discussion
A total of 40 species of medicinal plants used by the people around the Kakamega forest were identified and recorded ( Table 1 and data set). The species fall into 25 families ( Table 2) and the list represents 11% of all plant species recorded in Kakamega forest 21. It certainly not presumed here that the list of species from this study is a complete one for the Kakamega forest as, due to the constraints of time and resources, the study did not cover every part the forest. The most dominant families were Asteraceae, Fabaceae and Lamiaceae, each representing 10.3% of all species collected.
Table 2. Families and corresponding number of species of medicinal plants identified.
| Family | No of species | % proportion (N = 40) |
|---|---|---|
| Acanthaceae | 2 | 5 |
| Anacardiaceae | 1 | 2.5 |
| Apocynaceae | 1 | 2.5 |
| Asteraceae | 4 | 10.3 |
| Bignoniaceae | 1 | 2.5 |
| Ebenaceae | 1 | 2.5 |
| Euphorbiaceae | 2 | 5 |
| Fabaceae | 4 | 10.3 |
| Flacourtiaceae | 1 | 2.5 |
| Lamiaceae | 4 | 10.3 |
| Leguminoceae | 1 | 2.5 |
| Malvaceae | 1 | 2.5 |
| Melastomataceae | 1 | 2.5 |
| Meliaceae | 2 | 5 |
| Oleaceae | 1 | 2.5 |
| Paulowniaceae | 1 | 2.5 |
| Piperaceae | 2 | 5 |
| Ranunculaceae | 1 | 2.5 |
| Rosaceae | 1 | 2.5 |
| Rubiaceae | 1 | 2.5 |
| Rutaceae | 2 | 5 |
| Sapindaceae | 1 | 2.5 |
| Sapotaceae | 1 | 2.5 |
| Solanaceae | 1 | 2.5 |
| Verbenaceae | 2 | 5 |
Profiles of 40 putative medicinal plant species identified in and around Kakamega forest
Of the 40 species, 22 were shrubs, 13 trees, 3 lower plants such as herbs or forbs, and 2 were climbers. This dominance of the shrubs also supports the prominence of the three families of Asteraceae, Fabaceae and Lamiaceae ( Table 2). Twenty-six of the medicinal species occurred inside the forest itself and 14 occurred outside. One of the species (Prunus africana) is also listed in the IUCN Red List as vulnerable to extinction 22. This species was encountered inside the forest while no other such threatened species was encountered outside the forest and this might underscore the forest reserve’s role in aiding the conservation of medicinal species.
The majority of the species identified (95%) were indigenous and only 5% were exotic ( Table 1) a fact that also reflects the localized nature of the indigenous knowledge about these medicinal plant species. For instances, despite the presence of Eucalyptus sp (family Myrtaceae) and Grevillea sp (family Proteaceae) in and around certain parts of the forest such as the Isecheno and Buyangu blocks, no informant mentioned any medicinal uses associated with them. Some Eucalyptus species are known to be used in treatment of certain bacterial or fungal infections in humans 23 while Greville sp is used in treatment of skin sores and as an antiseptic 24.
The total number of species recorded in this study compares closely to that recorded by Jeruto 9 in a study of medicinal plants used around the Nandi forest but is much smaller than the 107 species recorded in a study by Okello et al. for medicinal plants used by the Sabaot people around Mt. Elgon 10 and the 119 species recorded by Ndegwa of medicinal plants used by the Ogiek people in the East Mau forest 11.
The diseases reported to be treated using the plant species varied widely but were grouped into 14 categories including use in the treatment of a number of livestock diseases ( Figure 2). Ninety percent of the diseases treated are those that affect humans and about ten percent for livestock diseases. Most of the human diseases treated using these species, fell into the categories of digestive or peptic; respiratory, vector-borne; and reproductive ailments ( Figure 2). Furthermore, these treatments are applicable for both genders and almost all age groups except in 17% of the cases where the treatments are applicable to adults only and 7% of the cases where treatments were applicable for old people only. 37% of the species are used by the local people to treat more than one condition. One particular species Azadirachta indica ( Table 1) is used by the local people to treat up to 6 different conditions, using all of its parts. This makes it the most valuable medicinal species even though it is of exotic origin 7. In 17% of the species, more than one plant part is used in the treatment of various conditons, not necessarily in combination.
Figure 2. Overall distribution of categories of disease treated using medicinal plants recorded.

In preparing the treatments from the plants, the local people mainly use leaves, roots and barks, but in a few species, the treatment is derived from flowers, fruits and young shoots ( Figure 3). Additionally, since many of the species are used in treating digestive or peptic, respiratory or vector-borne ailments, the majority of them are administered orally as an infusion, concoction, decoction or a lick of its powdered form 10. The rest are applied either on the surface of the affected part of the body, through steam treatment, as fluid drops or through inhalation of either its fresh form or powder prepared from its crushed form.
Figure 3. Percentage of use of the various parts of the medicinal plant species identified.

A number of diseases are treated by many medicinal species, reflecting the prevalence of those specific conditions in the community. These included diseases related to stomach upsets (12 species), boils (2 species), fevers and aches (5 species), diarrhea (3 species), colds and flu (2 species), worm infestation (3 species) and malaria (4 species).
The results of this study demonstrate that apart from the Kakamega forest’s reputation as a significant Kenyan rainforest in terms of its rich biodiversity, eco-system service provision and as a remarkable tourist site 7, 12– 14, it is also important to the local community as a repository for ethno-pharmacological resources that play a crucial role in supplementing the government’s effort in human and veterinary healthcare at the grass-root level, like the neighboring Nandi forest 9. Much of the indigenous knowledge about these plant-based remedies is still held mainly by elderly members of the community. Furthermore, most knowledge holders tend to descend from families with long histories of the practice of traditional herbal healing.
In-depth discussions with the informants and a cross-section of some respondents among the local residents further revealed that even when the healers prescribe treatment to their patients, only the ready-made preparations are provided by the traditional healers meaning the patients would not be informed of the plant species from which the treatment is derived nor the method of preparation of the treatment. Nevertheless, this system is slowly changing and in recent years, some flexibility appears to be emerging, with the traditional healers, including the ones interviewed in this study, quite willing to provide information about the traditional treatments in exchange for financial inducement or compensation. For example, it is not uncommon to see young people hawking such easily used medicinal plants as Mondia whytei (see Table 1) along the streets of local urban areas. Such financial inducement was reported by the informants as a motivation for a growing crop of up-coming but semi-skilled traditional healers in the community.
Although this study was concerned with the wide variety of diseases treated using the medicinal plant species found in the Kakamega forest, the percentage proportions of medicinal plant types (shrubs, trees, herbs, climbers and lianas) is similar to that found by Jeruto et al. 25 who carried out a similar but narrower study in the Nandi forest for species used in treatment of malaria only. This latter study identified 40 medicinal plant species just like in our study, perhaps because of the larger spatial coverage of their study area.
In terms of plant parts used in treatment, leaves were predominantly used ( Figure 3). This concurs with findings of a study in south-western Ethiopia 26 and in Morogoro, Tanzania 27, although these comparative studies were not carried out in forest habitats. However, it differs from findings of a similar survey conducted in the Mau forest, Kenya 11 and in Mt. Elgon 10, in both cases the use of roots was found to be predominant. One presumption for prominent use of leaves for treatments in Kakamega is that the destructive methods associated with root or bark harvesting, is restricted or not permissible or compatible with the conservation policies for the Kakamega 17 forest where most of the species are derived. Thus, extracting leaves provides a more sustainable use strategy through rapid replacement by re-growth and is a practice acquired down the generations 28. Leaves are also easier to harvest and prepare into various concoctions, decoctions or infusions such as an express juice for administration in treatment, than roots and bark. In addition, the preparation of various extracts from leaves ensures better preservation of the active ingredients of the medication, that in the case of other parts of the plant 10.
According to the respondents, most of the treatments are administered orally either as infusions, decoctions or concoctions. Similar results were obtained in another earlier study by Jeruto et al. in South Nandi forest specifically 9. This appears to be consistent with the fact that most of them are used to treat diseases related to the digestive, oral tract or respiratory system ( Figure 2). The high prevalence of digestive and respiratory-related diseases, compared to other afflictions, also appears to reflect relatively poor sanitation due to the high density of human population in the district (433 persons per kilometre 17), an area that relies on only one main public healthcare facility, the Kakamega Municipal Hospital 29. The mean distance is 10 km from patient-to-hospital and the doctor to patient ratio is 1:14,200. This is compounded by a poverty level of 52% and increasing levels of school drop-outs 29, implying correspondingly diminished knowledge about basic health and sanitation which are essential in managing such communicable digestive or respiratory diseases.
Conclusion
In conclusion, there is sufficient indigenous knowledge among the community around the Kakamega forest about medicinal plant species, to contribute not only to a sustainable provision of grass-root health care but also a potential to share this knowledge beyond western Kenya. Much of this knowledge is still held mainly by a few elderly people though financial inducements are said to be motivating a growing interest in the acquisition of knowledge among the wider community about these medicinal plants. This is encouraging because as the cost of conventional modern healthcare continues to increase, pushing such services out of reach to most rural dwellers in developing countries 30, there is a corresponding increased need to identify more affordable alternatives for the treatment of many ailments that affect rural populations. Unlocking such knowledge from the monopoly of a few to the wider population through an “accelerated” social construction 31 process such as through sustained public awareness campaigns, story telling or role plays, should thus be encouraged because such indigenous knowledge also has a potential for boosting economic empowerment of the local people through the sale of intellectual property rights or social capital. This may be leveraged further to boost conservation of such habitats from which medicinal plants are sourced, such as forests.
Recommendations
More extensive excursions into the Kakamega forest and its immediate surroundings to reveal more medicinal plant species, particularly through the involvement of a larger number of key informants. Low numbers of informants were used because our study was constrained by time and logistical issues, thus not allowing us to cover the whole forest. As evident, the total number of medicinal plants identified is unexpectedly small in comparison, for instance, to similar areas such as the South Nandi forest 26. Also it would be interesting to see if an equal number of male and female informants in the study might yield different knowledge perspectives such as the dominance of diseases of the alimentary canal and use of leaves over other medicinal plant parts, in the treatment of various diseases.
A deliberate effort to make accessible results of earlier studies on medicinal plants of the Kakamega forest, anecdotal and otherwise, would make such knowledge more widely accessible to the wider public for use in the treatment of diseases. This could be through publishing, with technical review and support involving local and scientific stakeholders.
Promotion of the use of natural remedies derived from various locally based resources such as medicinal plant species, should form an important priority of the Kenyan governments’ strategies to make healthcare accessible to rural populations in a more affordable way.
Acknowledgements
We wish to thank our three key respondents/informants Mr. John Shunza, Joel Mbogani and Femina Futa, the additional 4 opportunistically selected respodents as well as our interpreters Laban Shiundu, Patrick and Alphonse Ligaro for assistance with the location and identification of the medicinal plants and their uses; Kenya Wildlife Service (Buyangu, Kakamega) and Kenya Forestry Service (Isecheno Kakamega) for allowing us access to the forest to carry out the study; the local farmers on whose property some of the plants were encountered; the East African Herbarium staff for further assistance with plant identification; Helida Oyieke and Samuel Muchai for kindly reviewing the initial project proposal and finally Martin Potgieter and Hugo Asselin for reviewing the the first version of the article.
Funding Statement
Funds for the project were kindly provided by The Conservation Foundation in UK under its Young Scientist for Rainforests award scheme. The grant was awarded to Nickson Otieno. The grant had no grant number.
The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
v2; ref status: indexed
References
- 1.Berkes F: Rethinking community-based conservation. Cons Biol. 2004;18(3):621–630 10.1111/j.1523-1739.2004.00077.x [DOI] [Google Scholar]
- 2.Biswas S: Indigenous traditional knowledge integration for forest biodiversity conservation: Needs and priorities.Paper submitted at the VII World Forestry Congress, 2003 Quebec Canada2003. Reference Source [Google Scholar]
- 3.Smith D, Pretty J: Social capital in biodiversity conservation and management. Cons Biol. 2003;18(3):631–638 10.1111/j.1523-1739.2004.00126.x [DOI] [Google Scholar]
- 4.The Rainforest Foundation Indigenous knowledge.The Rainforest Foundation. Accessed on 08/November/20122011. Reference Source [Google Scholar]
- 5.Kala CP: Aboriginal uses and management of ethnobotanical species in deciduous forests of Chhattisgarh state in India. J Ethnobiol Ethnomed. 2009;5(20):1–9 10.1186/1746-4269-5-20 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Ellen R: Anthropological approaches to understanding the ethno-botanical knowledge of rainforest populations.In: ‘Tropical rainforest research: current issues’, Edwards, D. S., Booth, W. B. and Choy, S. C. (eds). Kluwer: Dordrecht1996;457–465 Reference Source [Google Scholar]
- 7.Beentje HJ: Kenya Trees, Shrubs and Lianas.National Museums of Kenya. Nairobi.1994. Reference Source [Google Scholar]
- 8.Kokwaro JO: Medicinal Plants of East Africa (2nd.Ed.),Kenya Literature Bureau of Kenya, Nairobi. Pp 35, 49, 69, 128, 158, 4011993 [Google Scholar]
- 9.Jaruto P, Lukhoba C, Ouma G, et al. : An ethnobotanical study of medicinal plants used by the Nandi people in Kenya. J Ethnopharmacol. 2008;116(2):370–376 10.1016/j.jep.2007.11.041 [DOI] [PubMed] [Google Scholar]
- 10.Okello SV, Nyunja RO, Netondo GW, et al. : Ethnobotanical study of medicinal plants used by Sabaots of Mt. Elgon Kenya. Afr J Trad CAM. 2009;7(1):1–10 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Ndegwa FK: Use, conservation and harvesting of medicinal plants by the Ogiek people of East Mau forest, Nakuru district, Kenya.Kenyatta University Library Online2012 [Google Scholar]
- 12.Fashing PJ, Gathua JM: Spatial variability in the vegetation structure and composition of an East African rain forest. Afr J Ecol. 2004;42(3):189–197 10.1111/j.1365-2028.2004.00512.x [DOI] [Google Scholar]
- 13.Otieno NE, Gichuki N, Farwig N, et al. : The role of farm structure on bird assemblages around a Kenyan tropical rainforest. Afr J Ecol. 2011;49(4):410–417 10.1111/j.1365-2028.2011.01273.x [DOI] [Google Scholar]
- 14.Bennun AL, Njoroge P: Important Birds Areas in Kenya.East Africa Natural History Society, Nairobi, Kenya.1999. Reference Source [Google Scholar]
- 15.Bird Life International Important Bird Areas factsheet: Kakamega forest.Accessed on 20/November/20122012. Reference Source [Google Scholar]
- 16.Kokwaro JO: Conservation status of the Kakamega Forest in Kenya: the easternmost relict of the equatorial rain forests of Africa. Mon Syst Bot Miss Bot Gard. 1988;25:471–489 Reference Source [Google Scholar]
- 17.Akotsi EFN, Situma CA, Nzioka B, et al. : Mapping land-use/land cover changes in Kakamega forest (1975–2005).International Centre of Insect Physiology and Ecology and the Department of Resource Surveys and Remote Sensing. Nairobi, Kenya2006 [Google Scholar]
- 18.Rietdorf U, Kappel R, Kaikai WO: Linking local resources to SME development. A pathway out of poverty.Project Report of BIOTA East Africa. Hamburg, Germany2006. Reference Source [Google Scholar]
- 19.Kothari CR: Research Methodology: Methods and Techniques.2 ndEdn. New Age International (P) Ltd. New Delhi, India2000. Reference Source [Google Scholar]
- 20.Badshah L, Hussian F: People preferences and use of local medicinal flora in District Tank, Pakistan. J Med Plnt Res. 2011;5(1):22–29 Reference Source [Google Scholar]
- 21.Kakamega Environmental Education Programme Plants of Kakamega forest.Accessed 14/November/2012.2012. Reference Source [Google Scholar]
- 22.IUCN IUCN Red List of threatened species.Version 2012. Accessed 09 November 20122012. Reference Source [Google Scholar]
- 23.Takahashi T, Kokubo R, Sakaino M, et al. : Antimicrobial activities of eucalyptus leaf extracts and flavonoids from Eucalyptus maculata. Lett Appl Microbiol. 2004;39:60–64 10.1111/j.1472-765X.2004.01538.x [DOI] [PubMed] [Google Scholar]
- 24.Cock I: Medicnal plant images: Grevillea spp and Petalostigma pubescens. Pharmacognosy Communications. 2012;2(2):78 10.5530/pc.2012.2.12 [DOI] [Google Scholar]
- 25.Jeruto P, Mutai C, Ouma G, et al. : An inventory of medicinal plants that the people of Nandi use to treat malaria. J Anim and Plnt Sc. 2011;9(3):1192–1200 Reference Source [Google Scholar]
- 26.Yineger H, Yewhalaw D: Traditional medicinal plant knowledge and use by local healers in Sekoru District, Jimma Zone, Southwestern Ethiopia. J Ethnobiol Ethnomed. 2007;3(24):24 10.1186/1746-4269-3-24 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Amri E, Kisangau DP: Ethnomedicinal study of plants used in villages around Kimboza forest reserve in Morogoro, Tanzania. J Ethnobiol Ethnomed. 2012;8(1):1 10.1186/1746-4269-8-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Hughes D, DuMont K: Using focus groups to facilitate culturally anchored research. Am J Community Psychol. 1993;21(6):775–806 Reference Source [DOI] [PubMed] [Google Scholar]
- 29.Kahuthu R, Muchoki T, Nyaga C, (Eds.), et al.: Kakamega District Strategic Plan.Government of Kenya (Ministry of Planning and National Development). Nairobi.2005 [Google Scholar]
- 30.Plaetse BV, Hlatiwayo G, Eygen LV, et al. : Costs and revenue of health care in a rural Zimbabwean district. J Health Pol Plann. 2005;20(4):243–251 10.1093/heapol/czi028 [DOI] [PubMed] [Google Scholar]
- 31.Lee Y: Indigenous knowledge construction and experimental learning of Taiwanese aborigines. Intern Ed Stud. 2009;2(2):155–161 Reference Source [Google Scholar]