

Abstract
Cystic lymphangiomas are rare tumours that can mimic various causes of acute abdomen including appendicitis. They exhibit variations in two characteristics on presentation: they can arise from a wide range of organs including various intra-abdominal structures and they can have a wide variation in size on presentation. We report a case of a gigantic cystic lymphangioma presenting as an acute abdomen closely mimicking acute appendicitis and we conduct a review of the relevant literature.
Keywords: Cystic lymphangioma, Acute abdomen, Acute appendicitis
Cystic lymphangiomas are rare benign tumours that can develop from a wide range of body organs and structures. Godart postulated that they result from failure of development and communication of premature lymphatics that normally coalesce and communicate with the venous system.1 In adults, however, sequestration of lymphatic tissue is most likely secondary to inflammatory processes or surgical or radiation therapy. Goh et al demonstrated that abdominal lymphangiomas have a male preponderance and present more acutely in paediatric patients, whereas in adults, female patients predominate and the history is more chronic.2 We report the case of a gigantic retroperitoneal cystic lymphangioma in a patient presenting with an acute abdomen closely mimicking acute appendicitis.
Case history
A 21-year-old overweight woman presented to the emergency department with acute abdominal pain that had worsened over 24 hours prior to admission. She described the pain as a constant central abdominal pain radiating subsequently to the right iliac fossa although it was still felt in the paraumbilical region. The pain was associated with nausea and vomiting of food particles that were not bile or blood stained. Her bowel habits remained unaltered. She felt feverish the night before and had nocturnal sweating. There were no specific chronic symptoms but the patient noted a recent gain in her weight.
On physical examination, performed by a senior registrar in the surgical department, she had a temperature of 38.7ºC and there was marked tenderness in the right iliac fossa with guarding and rebound tenderness. There was mild to moderate tenderness in the epigastric and paraumbilical regions with voluntary guarding. No abdominal masses were palpated. Blood results were unremarkable.
As a diagnosis of acute appendicitis was strongly suspected, the patient was promptly considered for surgery. After induction of anaesthesia, a prominent swelling was palpated in the epigastric region. Accordingly, laparoscopic exploration was undertaken to evaluate this new finding. After a laparoscope was introduced through an infraumbilical incision, inadvertent rupture of the lower part of a giant, tense, fluid filled, multiloculated cyst occurred. A midline laparotomy incision was promptly done and the gigantic cyst was found to be arising from the lesser sac and extending into the pelvis (Fig 1). It was completely excised (Fig 2). No other cysts were noted in the abdominal or pelvic viscera.
Figure 1.

Intra-operative dissection of the wall of the cystic lymphangioma. Arrows indicate the origin of the cystic lymphangioma in the lesser sac.
Figure 2.

Cystic lymphangioma after excision
Histological examination of the pathological specimen (Fig 3) revealed a tissue diagnosis of a multilocular cystic lymphangioma with evidence of uniform inflammation. The patient remained asymptomatic and free of disease recurrence five years after the original procedure.
Figure 3.
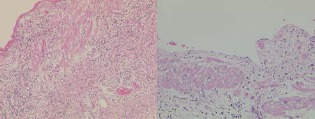
Histological images of the cystic lymphangioma
Discussion
The vast majority of cystic lymphangiomas (90%) originate from the head and neck, trunk and extremities. The remaining 10% occur sporadically in the mesentery and various thoracic and abdominal organs. Intra-abdominal cystic lymphangiomas are rare and can occur anywhere in the abdomen including perirenal, pararenal or pelvic extraperitoneal spaces. They are often solitary but may be multiple2,3 and can vary greatly in size on presentation.4 They also have a tendency to recur if they are incompletely removed by surgical excision.5
Cystic lymphangiomas may be diagnosed incidentally or alternatively present as bowel obstruction or signs of peritonitis as well as many acute presentations. A non-enhancing extramucosal mass with homogeneous attenuation is the typical finding on computed tomography and magnetic resonance imaging.
The localised nature of the clinical signs directed us towards an erroneous diagnosis of acute appendicitis with peritonitic signs mainly appreciated in the right iliac fossa. Involuntary guarding and the overweight habitus of the patient obscured the potential to appreciate an abdominal swelling that would otherwise have suggested an alternative diagnosis. Exploratory laparoscopy was an appropriate diagnostic option in what was essentially an unsuspected diagnostic entity. Though there is a potential for laparoscopic excision in experienced hands, the size and complexity of this rare condition influenced the decision to convert to an open procedure to accomplish complete excision of the cystic lymphangioma.
References
- 1.Godart S. Embryological significance of lymphangiomas. Arch Dis Child. 1966;41:204–206. doi: 10.1136/adc.41.216.204. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Goh BK, Tan YM, Ong HS, et al. Intra-abdominal and retroperitoneal lymphangiomas in pediatric and adult patients. World J Surg. 2005;29:837–840. doi: 10.1007/s00268-005-7794-0. [DOI] [PubMed] [Google Scholar]
- 3.Yang CS, Wu MS, Wang HP, et al. Disseminated cystic lymphangiomatosis presenting with acute abdomen: report of a case and review of the literature. Hepatogastroenterology. 1999;46:196–198. [PubMed] [Google Scholar]
- 4.Tsukada H, Takaori K, Ishiguro S, et al. Giant cystic lymphangioma of the small bowel mesentery: report of a case. Surg Today. 2002;32:734–737. doi: 10.1007/s005950200138. [DOI] [PubMed] [Google Scholar]
- 5.Alqahtani A, Nguyen LT, Flageole H, et al. 25 years’ experience with lymphangiomas in children. J Pediatr Surg. 1999;34:1,164–1,168. doi: 10.1016/s0022-3468(99)90590-0. [DOI] [PubMed] [Google Scholar]