

Dear Editor,
Homocystinuria caused by cystathionine-β-synthase deficiency is a genetic disorder with autosomal recessive inheritance resulting in elevated homocysteine levels. The main ocular feature is ectopia lentis.[1] Megalocornea, microspherophakia in association with homocystinuria are rarely reported in literature.[2] We report two siblings of Indian origin and born out of second degree consanguity with homocystinuria who had variable ocular and systemic involvement. One sibling aged 6 years presented with best corrected visual acuity (BCVA) of 4/60 in both eyes (BE) with 15 degrees of exotropia in the left eye (LE). Corneas were clear with vertical and horizontal diameters 12.5 and 13 mm, respectively, in BE qualifying for megalocornea. Anterior chamber was irregularly shallow in BE. Iridophacodonesis was present in BE and the edge of clear lens was visible temporally in LE [Fig. 1]. Intraocular pressure (IOP) was 13 mmHg (RE) and 16 mmHg (LE). Gonioscopy showed narrow angles. Dilated evaluation of each eye revealed superonasal subluxation of a small lens with increased anteroposterior thickness suggestive of microspherophakia. Axial lengths were 22.08 mm (BE). Serum homocysteine levels were elevated (16.02 μmol/l by using Chemiluminescence ADVIA Centaur CP Immunoassay System (Siemens Health care Diagnostic, Germany). Systemic evaluation revealed global developmental delay and umbilical hernia [Fig. 2]. Pilocarpine eye drops instilled prior to laser iridotomy to prevent pupillary block resulted in inverse glaucoma RE, further strengthening the diagnosis of microspherophakia.
Figure 1.
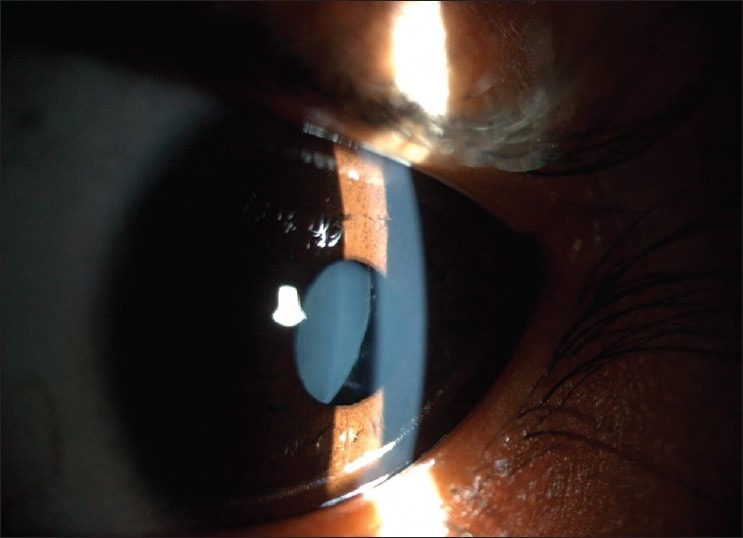
Subluxated lens seen in undilated eye with shallow anterior chamber in first child
Figure 2.
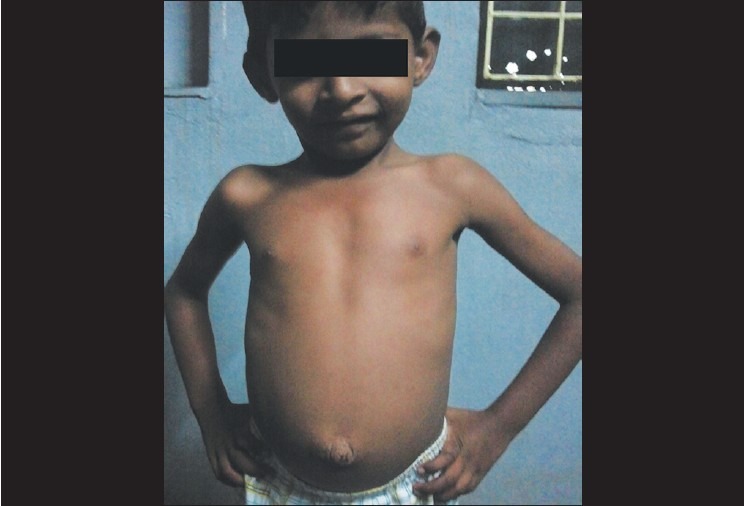
The first child with poor built and umbilical hernia
The other sibling was 9-years-old with BCVA 20/200 (BE). Corneas were clear and the corneal diameters were 12 mm horizontally and 11.5 mm vertically in BE. Anterior chamber was shallow, more nasally in BE. IOP was 12 mmHg (RE) and 14 mmHg (LE). Only dilated examination revealed nasal subluxation of the lens of about 6 clock hours in BE [Fig. 3]. The child had increased serum homocysteine (18 μmol/l levels) and systemic evaluation revealed scar of inguinal hernia repair. Fundus examination was normal in both the siblings.
Figure 3.

Second child showing nasal subluxation of the lens only after dilatation
Of the phenotypic variants recognized in homocystinuria, our siblings were probably B6 responsive type because they had mild systemic involvement with normal intelligent quotient (IQ). The major findings in classic homocystinuria are developmental delay, intellectual disability, and skeletal abnormalities such as excessive height and length of the limbs, vascular abnormalities in the form of thromboembolism. The first child had developmental delay and umbilical hernia, while the second child had only inguinal hernia. Ectopia lentis is reported to occur in 90% of patients. Homocysteinylation of fibrillin-1 leads to alterations of self-interaction properties due to a reduction of disulfide-bonded C-terminal fibrillin-1 multimers[3] leading to the weak zonules and progressive ectopia lentis. Mulvihill et al., in their study have shown that ectopia lentis in homocystinuria develops after 1 year and maximum by 8 years of age.[4] Both the siblings in this study developed ectopia lentis by 8 years of age. The superonasal subluxation was also atypical as the common type of subluxation seen is nasal or inferior.[5] Other ocular features include optic atrophy, iris atrophy, anterior staphylomas, and corneal opacities. Retinal detachments occur in 5-10%. The first sibling had a MESH (megalocornea, ectopia lentis, spherophakia, homocystinuria) association, but the second sibling did not have this association. The cases are presented because of the atypical ocular and systemic features with varying phenotypic presentations. Presence of abdominal hernia in children may be associated with collagen disorders and hence an ocular examination may be sought in view of development of glaucoma and ambyopia secondary to a subluxated lens.
References
- 1.Spaeth GL, Barber GW. Homocystinuria- its ocular manifestations. J Pediatr Ophthalmol. 1996;3:42–8. [Google Scholar]
- 2.Lieberman TW, Podos SM, Hartstein J. Acute glaucoma, ectopia lentis and homocystinuria. Am J Ophthalmol. 1966;61:252–5. doi: 10.1016/0002-9394(66)90278-9. [DOI] [PubMed] [Google Scholar]
- 3.Hubmacher D, Cirulis JT, Miao M, Keeley FW, Reinhardt DP. Functional consequences of homocysteinylation of the elastic fiber proteins fibrillin-1 and tropoelastin. J Biol Chem. 2010;285:1188–98. doi: 10.1074/jbc.M109.021246. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Mulvihill A, Yap S, O’Keefe M, Howard PM, Naughten ER. Ocular findings among patients with late-diagnosed or poorly controlled homocystinuria compared with a screened, well- controlled population. J AAPOS. 2001;5:311–5. doi: 10.1067/mpa.2001.118219. [DOI] [PubMed] [Google Scholar]
- 5.Ramsey MS, Daitz LD, Beaton JW. Lens fringe in homocystinuria. Arch Ophthalmol. 1975;93:318. doi: 10.1001/archopht.1975.01010020328014. [DOI] [PubMed] [Google Scholar]