

Abstract
INTRODUCTION
Appendiceal mucinous neoplasms represent an exceptionally rare form of pathology with an incidence rate ranging between 0.2 and 0.3% of all appendectomies.1,2 The most common presentation is right lower quadrant pain with a palpable abdominal mass present in 50% of cases.8–12 Patients may also present with nausea, vomiting, change in bowel habits, weight loss, appendicitis, intestinal obstruction, ureteral compression, or lower gastrointestinal bleeding. Early diagnosis and proper surgical precautions must be implemented to prevent iatrogenic rupture of the appendix and the widespread seeding of potentially malignant mucin-producing cells throughout the peritoneal cavity.
PRESENTATION OF CASE
A 50-year-old African-American female presented with complaints of left-sided pelvic pain. Pelvic examination revealed adnexal fullness with thickening behind the cervix. An adnexal mass was revealed on ultrasound and MRI. The patient was subsequently taken to the operating room for a planned robotic salpingectomy. During the procedure, she was unexpectedly found to have an abnormally large appendix displaced to the left lower quadrant. General surgery was consulted intra-operatively to perform an appendectomy. The final pathology report revealed a low-grade mucinous adenocarcinoma with mucin dissecting into the wall of the appendix.
DISCUSSION
Appendiceal mucinous cystadenomas are characterized by hyperplasia of glandular epithelium along with hypersecretion of mucous resulting in a grossly dilated appendix. The clinical manifestation of appendiceal mucoceles is often non-specific. The prevalence is higher in women than men (4:1) with the average age at the time of diagnosis being 54 years-old.14–17 Appendiceal mucinous cystadenomas can be particularly problematic for women as these tumors are commonly misdiagnosed pre-operatively as right-sided adnexal masses due to commonalities in clinical presentation and diagnostic findings.8–12 It is estimated that based on imaging studies only 15–29% of appendiceal mucinous cystadenomas are correctly diagnosed prior to surgical intervention.13
CONCLUSION
To the best of our knowledge, only one other case of appendiceal adenocarcinoma with left-sided presentation has been reported. Appendiceal carcinomas can create a diagnostic dilemma due to non-specific clinical findings and inadequate imaging studies. Early recognition and careful intra-operative precautions must be taken to maintain the integrity of the appendix to prevent iatrogenic rupture and the spread of potentially malignant mucin-producing cells throughout the peritoneal cavity.
Keywords: Appendiceal mucinous adenocarcinoma, Appendiceal neoplasm, Appendectomy, Left-lower quadrant pain, Left-sided mass, Adnexal mass
1. Introduction
Appendiceal mucinous neoplasms represent an exceptionally rare form of pathology with an incidence rate ranging between 0.2 and 0.3% of all appendectomies.1,2 They are classified as either low-grade mucinous neoplasms or mucinous adenocarcinomas based on architectural and cytologic features. Tumors that are confined to the appendix with a low-grade histology are usually benign. Right hemicolectomy is indicated for: (1) invasive adenocarcinoma; (2) tumors near the cecum; (3) lesions larger than 2 cm; (4) mucin production; (5) invasion of the lymphatics, serosa, or mesoappendix; or (6) cellular pleomorphism with a high mitotic rate.3 It is important for gynecologists and general surgeons to consider appendiceal mucinous cystadenomas in their differential diagnosis for a pelvic mass because early recognition and extra intra-operative precautions must be implemented to prevent iatrogenic rupture and subsequent spilling of potentially malignant mucin-producing cells throughout the peritoneal cavity. We report a case of a low-grade mucinous tumor of the appendix diagnosed at time of surgery.
2. Presentation of case
A 50-year-old African-American female presented with complaints of left-sided pelvic pain. She was being treated at a tertiary care university-based teaching hospital. Pelvic examination revealed adnexal fullness with thickening behind the cervix. An adnexal mass was revealed on ultrasound and MRI (see Figs. 1 and 2). The patient was subsequently taken to the operating room for a planned robotic salpingectomy. During the procedure, she was unexpectedly found to have an abnormally large appendix displaced to the left lower quadrant. Operative findings included a 9 cm × 3 cm dilated appendix adhesed to the peritoneum along with extensive adhesions between pericolic adipose tissue of the cecum and the left pelvic sidewall (see Fig. 3). The patient was found to have a normal appearing right atrophic ovary and right fallopian tube. The left ovary and fallopian tube were found to be previously removed from a prior operation. General surgery was consulted intra-operatively to perform an appendectomy. The final pathology report revealed a low-grade mucinous adenocarcinoma with mucin dissecting into the wall of the appendix (see Fig. 4). The patient was subsequently brought back to the operating room for a hemi-colectomy. Final pathology revealed no evidence of malignancy at the resection margin.
Fig. 1.

Ultrasound – midline tubular structure measuring 9.6 cm × 4 cm transverse and AP 2.3–3.3 cm suspicious of hydrosalpinx.
Fig. 2.
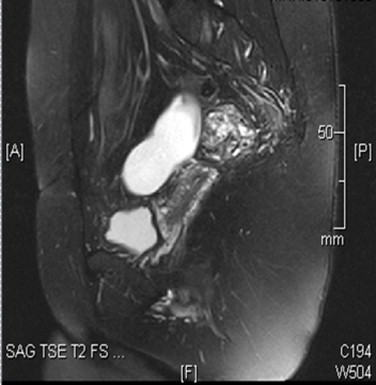
MRI – there is a tubular fluid containing structure present within the pelvis that appears to originate from the left adnexa and extends superiorly to cross the midline to the right hemipelvis.
Fig. 3.

Intra-operative imaging showing dilated appendix adhesed to left pelvic sidewall. Laparoscopic exploration revealed a normal right fallopian tube and ovary. Left fallopian tube and ovary were previously surgically removed.
Fig. 4.
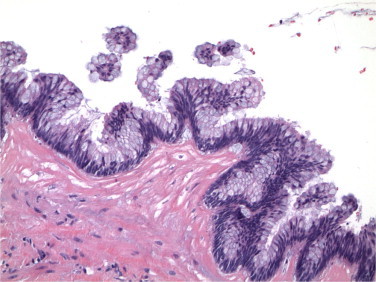
20× – the epithelial cell lining is seen to be composed of mucinous type columnar cells with occasional papillary tufting. There is minimal to mild cytologic nuclear atypia and no mitoses are seen.
3. Discussion
Appendiceal mucinous cystadenomas are characterized by hyperplasia of glandular epithelium along with hypersecretion of mucous resulting in a grossly dilated appendix. In a study of 2660 appendectomy specimens, mucinous cystadenomas were reported in only 0.6% of the cases.4 The clinical manifestation of appendiceal mucoceles is often non-specific. Retrospective studies have shown that up to 25% of patients harboring large lesions remain entirely asymptomatic until the lesions are discovered incidentally during surgery or imaging studies for alternative purposes.5–7 The most common presentation, however, is severe right lower quadrant pain with a palpable abdominal mass present in 50% of cases. 8–12 Patients may also present with nausea, vomiting, change in bowel habits, weight loss, appendicitis, intestinal obstruction, ureteral compression, or lower gastrointestinal bleeding.6,8–12 The prevalence is higher in women than men (4:1) with the average age at the time of diagnosis being 54 years-old.14–17Appendiceal mucinous cystadenomas can be particularly problematic for women as these tumors are commonly misdiagnosed pre-operatively as right-sided adnexal masses due to commonalities in clinical presentation and diagnostic findings.8–12 It is estimated that based on imaging studies only 15–29% of appendiceal mucinous cystadenomas are correctly diagnosed prior to surgical intervention.13 Consequently, surgeons are often forced to abruptly change surgical tactics intra-operatively to perform an appendectomy while taking extra precaution to maintain the organ's integrity. Iatrogenic rupture of the appendix can be disastrous as it greatly increases the risk of widespread seeding of potentially malignant mucin-producing cells throughout the peritoneal cavity, a condition known as pseudomyxoma peritonei.17
4. Conclusion
To the best of our knowledge, only one other case of appendiceal adenocarcinoma with left-sided presentation has been reported. Appendiceal carcinomas can create a diagnostic dilemma due to non-specific clinical findings and inadequate imaging studies. They are usually asymptomatic and are diagnosed incidentally during surgery. Mucinous neoplasms with acellular mucin in the appendiceal wall or surrounding the appendix are associated with an excellent prognosis and these cases should be managed similarly to appendiceal adenomas. Early recognition and careful intra-operative precautions must be taken to maintain the integrity of the appendix to prevent iatrogenic rupture and the spread of potentially malignant mucin-producing cells throughout the peritoneal cavity.
Conflict of interest statement
None.
Funding
None.
Ethical approval
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Author contributions
Data collection and writing were performed by all the authors.
Footnotes
This is an open-access article distributed under the terms of the Creative Commons Attribution-NonCommercial-No Derivative Works License, which permits non-commercial use, distribution, and reproduction in any medium, provided the original author and source are credited.
References
- 1.Bartlett C., Manoharan M., Jackson A. Mucocele of the appendix—a diagnostic dilemma: a case report. J Med Case Rep. 2007;1:183. doi: 10.1186/1752-1947-1-183. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Stang A., Braumann D., Teichmann W. Mucocele of the appendix. Incidental sonographic discovery and laparoscopic resection. Dtsch Med Wochenschr. 2004;129:2295–2298. doi: 10.1055/s-2004-835258. [DOI] [PubMed] [Google Scholar]
- 3.Gouzi J., Laigneau P., Delaalande J., Flamant Y., Bloom E., Oberlin P. Indications for right hemicolectomy in carcinoid tumors of the appendix. Surg Gynecol Obstet. 1993;176(June (6)):543–547. [PubMed] [Google Scholar]
- 4.Marudanayagam R., Williams G.T., Rees B.I. Review of the pathological results of 2660 appendectomy specimens. J Gastroenterol. 2006;41:745–749. doi: 10.1007/s00535-006-1855-5. [DOI] [PubMed] [Google Scholar]
- 5.Misdraji J., Yantiss R.K., Graeme-Cook F.M., Balis U.J., Young R.H. Appendiceal mucinous neoplasms: a clinicopathologic analysis of 107 cases. Am J Surg Pathol. 2003;27(August (8)):1089–1103. doi: 10.1097/00000478-200308000-00006. [DOI] [PubMed] [Google Scholar]
- 6.Korkolis D.P., Apostolaki K., Plataniotis G.D., Tzorbatzoglou J., Karaitianos I.G., Vassilopoulos P.P. Mucocele of the appendiceal stump due to benign mucinous cystadenoma. Anticancer Res. 2006;26:635–638. [PubMed] [Google Scholar]
- 7.Connor S.J., Hanna G.B., Frizelle F.A. Appendiceal tumors: retrospective clinicopathologic analysis of appendiceal tumors from 7,970 appendectomies. Dis Colon Rectum. 1998;41:75–80. doi: 10.1007/BF02236899. [DOI] [PubMed] [Google Scholar]
- 8.Scaffa C., Di Bella O., Tartaglia E., Rotondi M., Lup F., Messalli E.M. Surgical approach to appendiceal mucocele mimicking an adnexal complex mass: case report. Eur J Gynaecol Oncol. 2007;28(6):503–505. [PubMed] [Google Scholar]
- 9.Gortchev G., Tomov S., Dimitrov D., Nanev V., Betova T. Appendiceal mucocele presenting as a right adnexal mass: a case report. Obstet Gynecol Int. 2010 doi: 10.1155/2010/281053. pii:281053. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Dragoumis K., Mikos T., Zafrakas M., Assimakopoulos E., Venizelos I., Demertzidis H. Mucocele of the vermiform appendix with sonographic appearance of an adnexal mass. Gynecol Obstet Invest. 2005;59(3):162–164. doi: 10.1159/000083680. [DOI] [PubMed] [Google Scholar]
- 11.Jaluvka V., Becker R. Preoperatively as adnexa tumor diagnosed mucocele of the appendix. Zentralbl Gynakol. 1991;113(15–16):879–882. [PubMed] [Google Scholar]
- 12.Caracappa D., Gullà N., Gentile D., Listorti C., Boselli C., Cirocchi R. Appendiceal mucocele. A case report and literature review. Ann Ital Chir. 2011;82(May–June (3)):239–245. [PubMed] [Google Scholar]
- 13.Ruiz-Tovar J., Teruel D.G., Castiñeiras V.M., Dehesa A.S., Quindos P.L., Molina E.M. Mucocele of the appendix. World J Surg. 2007;31:542. doi: 10.1007/s00268-006-0454-1. [DOI] [PubMed] [Google Scholar]
- 14.Kalu E., Croucher C. Appendiceal mucocele: a rare differential diagnosis of a cystic right adnexal mass. Arch Gynecol Obstet. 2005;2771:86–88. doi: 10.1007/s00404-004-0663-5. [DOI] [PubMed] [Google Scholar]
- 15.Madwed D., Mindelzun R., Jeffrey R.B., Jr. Mucocele of the appendix: imaging findings. AJR Am J Roentgenol. 1992;159:69–72. doi: 10.2214/ajr.159.1.1609724. [DOI] [PubMed] [Google Scholar]
- 16.Dachman A.H., Lichtenstein J.E., Friedman A.C. Mucocele of the appendix and Pseudomyxoma peritonei. AJR Am J Roentgenol. 1985;144:923–929. doi: 10.2214/ajr.144.5.923. [DOI] [PubMed] [Google Scholar]
- 17.Jeshil R.S., Vipul P. Ruptured giant mucocele of the appendix with Pseudomyxoma peritonei. Appl Radiol. 2012;42(9):29–30. [Google Scholar]