

Abstract
Introduction
The purpose of our study was to evaluate clinical and pathological characteristics as well as treatment outcomes in HIV-infected patients with disseminated tuberculosis from the Regional HIV/AIDS Center Constanţa, Romania, and to determine associated risk factors.
Methods
We analyzed HIV-infected adults diagnosed with disseminated tuberculosis (TB) over the past two years, monitored in the Regional HIV/AIDS Center Constanţa.
Results
Out of a total number of 956 HIV-infected patients, 42 had been diagnosed with tuberculosis over the past two years (2011-2013) (4.39%) and 16 of them developed disseminated TB (38%). At the time of diagnosis, we recorded abnormal chest X-rays in 8 (50%), and positive sputum cultures in 4 (25%) of them. The median CD4 count was 40 cells/μL with a range of 5-85 cells/μL; HIV-RNA was detectable in all cases. Multidrug-resistant tuberculosis (MDR-TB) was identified in 6 cases. The outcome was unfavorable in 15 patients.
Conclusion
In our study, disseminated tuberculosis appeared to be a common pattern of evolution of HIV-TB co-infection (38%). Sputum smear positivity was low and chest X-ray images did not follow a typical pattern. HIV-TB co-infected patients with CD4 lymphocyte cell count <50 cells/μL were more likely to have disseminated TB. The severity of cases, proved by a high mortality rate, requires consideration of this diagnosis early in patients with advanced AIDS, even if laboratory investigations are not suggestive.
Keywords: HIV, disseminated tuberculosis, MDR-TB
Introduction
Disseminated tuberculosis (TB) is a contagious bacterial infection characterized by hematogenous or lymphatic spread of Mycobacterium tuberculosis from the lungs to other parts of the body.1 It is also known as miliary tuberculosis or extrapulmonary tuberculosis respecting multiplicity of the body sites involved. Because the clinical manifestations are nonspecific and polymorphic, it can mimic several other disorders, and diagnosis is often difficult.
The World Health Organization (WHO) reported that one third of the world's population is infected with Mycobacterium tuberculosis, with roughly 9 million new cases of active TB in 2010.2 Furthermore, 14.8% of TB patients have HIV coinfection.2 Conversely, the risk of coinfection with TB is about 20-37 times higher among those infected with HIV, and one in four deaths in the HIV-positive population is attributed to tuberculosis.3
According to several studies, among the opportunistic infections occurring in HIV seropositive persons, TB is the most common, with high risk for mortality.4 HIV infection increases the probability of acquiring TB, possibly leading to an unfavorable outcome for these patients.5,6
Another serious problem that has emerged in the past years is the appearance of Mycobacterium tuberculosis strains exhibiting multidrug-resistance (MDR) – resistance to at least isoniazid and rifampicin. This may be due to inadequate control, poor surveillance, delayed diagnosis, or inappropriate drug intake by patients. However, the clinical manifestations are similar to those classically described in infections with non-resistant strains, although the chest roentgenographic appearance is more often atypical, with an alveolar infiltrate, while cavitation is more frequent than with nonresistant TB.7
We performed a retrospective case record study to describe clinical and pathological characteristics, as well as treatment outcomes of HIV-infected patients with disseminated tuberculosis from the Regional HIV/AIDS Center Constanţa, Romania, and to determine associated risk factors.
Methods
We analyzed HIV-infected adults diagnosed with disseminated TB during the past two years (2011-2013) in our Regional Center. Due to the retrospective nature of the study, the TB diagnosis was established based on symptoms and history (prolonged fever, weight loss), clinical examination, chest X-ray (16 patients), CT scan/MRI (16 patients) of the affected area, sputum or pleural effusion cultures (16 patients), pleural biopsy (5 cases), bronchoscopy for biopsy or culture (5 patients), pathological examination (lymph node biopsy for the patients that survived and autopsy exam for the patients that did not survive). Naïve patients were defined as those who had never received antiretroviral therapy, whereas experienced patients had already received antiretroviral therapy at the time of disseminated TB diagnosis.
Statistical Analysis
A descriptive analysis was conducted, identifying the main characteristics of patients recruited into the study. Multivariable logistic regression analyses were performed to determine independent associations between patient characteristics and site of disease. For statistical analysis we used Microsoft Excel and Epi Info.
Results
Out of the 956 HIV-infected patients monitored in the Regional HIV/AIDS Center Constanţa, 42 had been diagnosed with tuberculosis in the past two years (4.39%). Out of this total number of 42 cases, 16 of them developed disseminated TB (38.09%) while 26 patients only had pulmonary tuberculosis.
Most of the patients diagnosed with disseminated TB were men (M/F =13/3), aged 22-66 years (median age 35.57 years). Nine out of the 16 patients had ages ranging from 22 to 25 years, as they are part of the “Romanian cohort” of children born in 1987-1989.
At the time of diagnosis, prolonged fever was reported in all patients, more than 5 kg weight loss was reported in 14 (87.5%) patients, abnormal chest X-rays in 8 (50%), and identification of Mycobacterium tuberculosis strains in the sputum cultures was reported in 4 (25%) patients (Table 1).
Table 1. Characteristics of patients with disseminated TB (N=16).
| Patient characteristics | |
| Gender M/F | 13/3 |
| Age (median) | 35.57 years |
| Naïve/Experienced patients | 5/11 |
| Pulmonary TB or TB infection in the medical history (no. of patients/total) | 6/16 |
| MDR-TB (no. of patients/total) | 6/16 |
| Relevant findings | N (%) |
| Prolonged fever | 16 (100%) |
| Weight loss | 14 (87.5%) |
| Abnormal chest X-rays (upper-lobe infiltrates and cavities with mediastinal lymphadenopathy) | 8 (50%) |
| Positive sputum cultures | 4 (25%) |
| Negative sputum cultures | 12 (75%) |
| Laboratory data | |
| Median CD4 cell count | 40 cells/μL |
| Median HIV-RNA | 266,965 copies/mL |
The median CD4 cell count was 40 cells/μL with a range of 5-85 cells/μL; HIV-RNA was detectable in all cases (median viral load – 266,965 copies/mL, range 707-758,086 copies/mL), and 12 patients (75%) had HIV-RNA greater than 100,000 copies/mL.
In order to identify the risk factors, we compared two groups of HIV patients with TB infection, namely pulmonary TB patients versus disseminated TB patients. The median CD4 cell count level in the pulmonary TB group was 148 cells/μL, versus 40 cells/μL in the disseminated TB group. Multivariate analysis demonstrated that HIV-TB co-infected patients with CD4 lymphocyte cell counts <50 cells/μL were more likely to have disseminated TB (p=0.0046). The statistical analysis was done with the 2-tailed Fisher's exact and chi-square test.
Similar results were reported by Leeds et al;8 they concluded that patients with CD4 cell counts <100 were more likely to have severe forms of extrapulmonary TB (central nervous system, meningeal, and/or disseminated).
Five patients had been recently diagnosed with HIV (less than one month back) and were not receiving antiretroviral treatment, while 11 patients were already on antiretroviral therapy but were noncompliant.
Medical history revealed a previous episode of pulmonary TB in 6 of the patients, treated with rifampicin, isoniazid, ethambutol and pyrazinamide; all of them presented MDR-TB at the time their data was collected for the study.
The outcome was unfavorable, with death, in 15 cases; 6 patients were noncompliant to tuberculosis therapy and died 2-3 months after starting specific treatment; in 4 cases the diagnosis was delayed because the symptoms were nonspecific and unfortunately the negative results of the bacteriologic analyses (sputum smears and cultures) had been interpreted as proof against TB in the differential diagnosis.
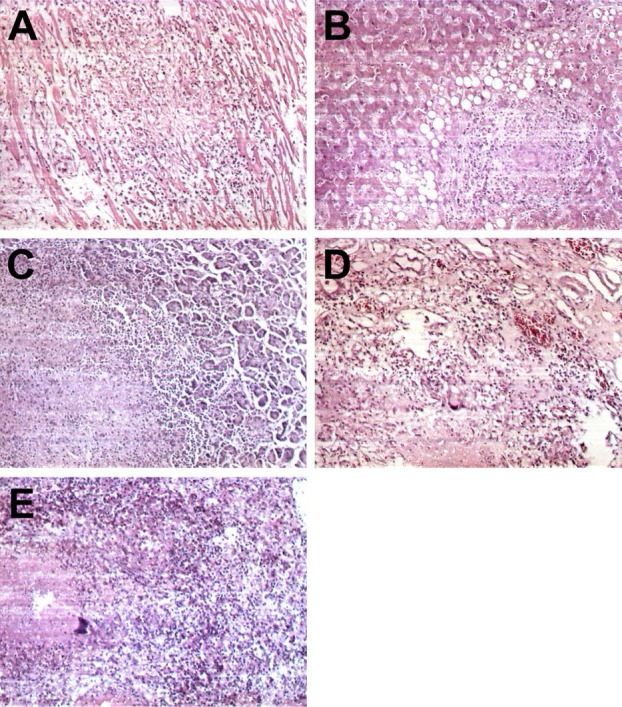
Pathological examination (performed in 15 cases) revealed lung involvement in 12 cases (75%), mediastinal lymphadenopathy in 11 cases, liver (2 cases), spleen (4 cases), kidney (4 cases), pancreas (1 case), meninges (3 cases), pleura (5 cases), heart (3 cases), pericardium (3 cases) and peritoneum involvement (5 cases) (Table 2, Figure, A-E).
Table 2. Pathological examination (autopsy exam).
| Pathological examination – organ involvement | N (%) |
| Lung | 12 (75%) |
| Mediastinal lymphadenopathy | 11 (68.75%) |
| Liver | 2 (12.5%) |
| Spleen | 4 (25%) |
| Kidney | 4 (25%) |
| Pancreas | 1 (6.25%) |
| Meninges | 3 (18.75%) |
| Pleura | 5 (31.25%) |
| Pericardium | 3 (18.75%) |
| Heart | 3 (18.75%) |
| Peritoneum | 5 (31.25%) |
Figure. A - Heart granuloma showing epithelioid cells and lymphocytes between cardiomyocytes (autopsy exam, HEx100); B - Liver granuloma showing giant and epithelioid cells and lymphocytes in the periphery; some of the hepatocytes display macrovesicular steatosis (autopsy exam, HEx100); C - Caseating granuloma of the pancreas showing caseous necrosis, epithelioid cells and lymphocytes in the periphery next to normal acini (autopsy exam, HEx100); D - Caseating granuloma of the kidney medulla showing caseous necrosis, giant cells and lymphocytes (autopsy exam, HEx100); E - Caseating granuloma of the spleen (autopsy exam, HEx100).
Discussion
Tuberculosis is a systemic disease that may involve any location of the body. It is divided usually in pulmonary and extrapulmonary TB; disseminated TB occurs when two or more noncontiguous sites of the body are involved at the same time. Several reports have shown that extrapulmonary TB and disseminated TB are both more frequent in HIV-infected patients (21.4% in Nigeria, 28% in India, and 38% in our study).9-11
Low CD4 cell counts are associated with an increased frequency of extrapulmonary TB. Similar to the report of Leeds et al., Jaryal et al. concluded that manifestations of tuberculosis in HIV/AIDS patients are in relationship with the CD4 count and disseminated tuberculosis was only found in patients with CD4 counts below 100 cells/μL.12 von Reyn et al. reported a low median CD4 count (30 cells/μL, range 1-122) in 20 subjects who developed disseminated TB13 and similar results were found in our study (40 cells/μL, range 5-85 cells/μL). In the same study, abnormal chest X-rays were found in 41% of patients and positive sputum cultures in 50% of patients.13
In our study we reported a smaller percentage, only 25% of patients had Mycobacterium tuberculosis strains in the sputum cultures, data similar to that of Chamie et al.14 and El-Hazmi et al.15
Patients with extrapulmonary or disseminated TB may present with signs and symptoms specific to the involved site, such as lymphadenopathy, headache, meningism, dysuria, back pain, ascites or abdominal pain. These findings in HIV-infected patients can present a diagnostic challenge.16-19 Furthermore, asymptomatic subclinical TB infection has been described, particularly in locations with a high prevalence of TB.20,21
In our study, similar to the data generally reported, the lymph nodes have been the most common extrapulmonary site of TB. In their study, Leeds et al. reported that 40% had concomitant pulmonary tuberculosis8 while in our study the percentage was much higher (75%).
Only a few clinical reports described pericardium, liver, spleen, peritoneum or pancreas involvement,17-19 with unfavorable outcome, similar to our study.
Conclusion
In our study, disseminated tuberculosis appeared to be a common pattern of evolution of HIV-TB co-infection (38%). Sputum smear positivity was low and chest X-ray images did not follow a typical pattern. HIV-TB co-infected patients with CD4 lymphocyte cell count <50 cells/μL were more likely to have disseminated TB and we consider that very low CD4 is a risk factor for the occurrence of disseminated TB. The severity of cases, proved by a high mortality rate, requires consideration of this diagnosis early in patients with advanced AIDS, even if laboratory investigations are not suggestive. Therefore, we recommend considering empiric therapy in patients with advanced AIDS and prolonged fever.
Footnotes
Conflicts of interest: The authors have declared no conflicts of interests.
References
- 1.A.D.A.M. Medical Encyclopedia. Disseminated tuberculosis. Atlanta (GA): A.D.A.M., Inc.; 2012. [Accessed on: January 03, 2014]. Available at: http://www.nlm.nih.gov/medlineplus/ency/article/000624.htm. [Google Scholar]
- 2.HIV InSite. Tuberculosis and HIV. [Accessed on: January 03, 2014]. Available at: http://hivinsite.ucsf.edu/insite?page=kb-05-01-06.
- 3.World Health Organization (WHO) TB/HIV Facts 2011/12. [Accessed on: January 03, 2014]. Available at: http://www.who.int/tb/publications/TBHIV_Facts_for_2011.pdf.
- 4.Kamath R, Sharma V, Pattanshetty S, Hegde MB, Chandrasekaran V. HIV-TB coinfection: Clinico-epidemiological determinants at an antiretroviral therapy center in Southern India. Lung India. 2013;30:302–6. doi: 10.4103/0970-2113.120605. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Gao L, Zhou F, Li X, Jin Q. HIV/TB co-infection in mainland China: a meta-analysis. PLoS One. 2010;5:e10736. doi: 10.1371/journal.pone.0010736. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Sharma SK, Mohan A, Kadhiravan T. HIV-TB co-infection: epidemiology, diagnosis & management. Indian J Med Res. 2005;121:550–67. [PubMed] [Google Scholar]
- 7.Klatt EC. Pathology of AIDS. Version 24. Savannah: Mercer University School of Medicine; 2013. [Google Scholar]
- 8.Leeds IL, Magee MJ, Kurbatova EV, et al. Site of extrapulmonary tuberculosis is associated with HIV infection. Clin Infect Dis. 2012;55:75–81. doi: 10.1093/cid/cis303. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Jones BE, Young SM, Antoniskis D, Davidson PT, Kramer F, Barnes PF. Relationship of the manifestations of tuberculosis to CD4 cell counts in patients with human immunodeficiency virus infection. Am Rev Respir Dis. 1993;148:1292–7. doi: 10.1164/ajrccm/148.5.1292. [DOI] [PubMed] [Google Scholar]
- 10.Affusim CC, Kesieme E, Abah VO. The pattern of presentation and prevalence of tuberculosis in HIV-seropositive patients seen at Benin City, Nigeria. ISRN Pulmonology. 2012;2012:6–12. [Google Scholar]
- 11.Vajpayee M, Kanswal S, Seth P, Wig N, Pandey RM. Tuberculosis infections in HIV-infected Indian patients. AIDS Patient Care STDS. 2004;18:209–13. doi: 10.1089/108729104323038883. [DOI] [PubMed] [Google Scholar]
- 12.Jaryal A, Raina R, Sarkar M, Sharma A. Manifestations of tuberculosis in HIV/AIDS patients and its relationship with CD4 count. Lung India 2011. 28:263–6. doi: 10.4103/0970-2113.85687. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.von Reyn CF, Kimambo S, Mtei L, et al. Disseminated tuberculosis in human immunodeficiency virus infection: ineffective immunity, polyclonal disease and high mortality. Int J Tuberc Lung Dis. 2011;15:1087–92. doi: 10.5588/ijtld.10.0517. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Chamie G, Luetkemeyer A, Walusimbi-Nanteza M, et al. Significant variation in presentation of pulmonary tuberculosis across a high resolution of CD4 strata. Int J Tuberc Lung Dis. 2010;14:1295–302. [PMC free article] [PubMed] [Google Scholar]
- 15.El-Hazmi MM, Al-Otaibi FE. Predictors of pulmonary involvement in patients with extra-pulmonary tuberculosis. J Family Community Med. 2012;19:88–92. doi: 10.4103/2230-8229.98287. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Iredia CH, Oguntibeju OO, Lewis HA, Mokwena K. Trends and characteristics of patients admitted with musculoskeletal tuberculosis to a referral hospital from 2003 to 2008. Afr J Microbiol Res. 2011;5:532–40. [Google Scholar]
- 17.Nancoz O, Kherad O, Perrin E, Hsu C, Lobrinus JA, Nendaz M. Disseminated tuberculosis presenting with polymorphonuclear effusion and septic shock in an HIV-seropositive patient: a case report. J Med Case Rep. 2010;4:155. doi: 10.1186/1752-1947-4-155. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Abdi-Liae Z, Moradnejad P, Alijani N, Khazraiyan H, Mansoori S, Mohammadi N. Disseminated tuberculosis in an AIDS/HIV-infected patient. Acta Med Iran. 2013;51:587–9. [PubMed] [Google Scholar]
- 19.Ntsekhe M, Mayosi BM. Tuberculous pericarditis with and without HIV. Heart Fail Rev. 2013;18:367–73. doi: 10.1007/s10741-012-9310-6. [DOI] [PubMed] [Google Scholar]
- 20.Oni T, Burke R, Tsekela R, et al. High prevalence of subclinical tuberculosis in HIV-1-infected persons without advanced immunodeficiency: implications for TB screening. Thorax. 2011;66:669–73. doi: 10.1136/thx.2011.160168. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Mtei L, Matee M, Herfort O, et al. High rates of clinical and subclinical tuberculosis among HIV-infected ambulatory subjects in Tanzania. Clin Infect Dis. 2005;40:1500–7. doi: 10.1086/429825. [DOI] [PubMed] [Google Scholar]