

Dear Editor:
A 60-year-old female presented with a pruritic and stinging, 1.8 cm-sized, indurated plaque with a central crust on the back (Fig. 1A) and she brought a firm, light-brown, round object on June 2012. She had been mountain climbing in Incheon, Korea 11 days earlier, and had felt a nodule on her back, which eventually dropped by itself while she undressed. Her past history and family history were nonspecific. On close examination, the nodule was a light-brown arthropod, 7×8 mm in size (Fig. 1B). A punch biopsy was performed on the skin lesion, including the central crust. Histopathologic examination revealed a cavity with surrounding dense inflammatory infiltrates composed of lymphocytes, neutrophils, and eosinophils in the dermis, and amorphous eosinophilic material deposits around an intradermal cavity (Fig. 2A). The fat tissue was pulled up to the mid dermis (Fig. 2B). The tick was oval in shape, 7×8 mm in size, and light brown in color (Fig. 1B). An ovoid spicular plate was located on the ventrolateral surface posterior to the coxa IV. The genital opening was straight and located on the level of the coxa IV. A round anus was located on the posterior portion, and a horseshoe-shaped anal groove was extended to the posterior margin of the body, surrounding the anus. The internal spur of the coxa I was long, and it did not overlap with the coxa II. The findings were consistent with the morphological features of Ixodes nipponensis. On follow-up examination after punch removal, the cutaneous finding dramatically improved.
Fig. 1.

(A) Pruritic and stinging, solitary, brownish nodule on the left back. (B) Photographs showing Ixodesis nipponensis (right: ventral surface; left: dorsal surface; scale: 1 mm; ⓐ: spicular plate; ⓑ: genital aperture; ⓒ: anus and anal groove; ⓓ: coxa IV).
Fig. 2.
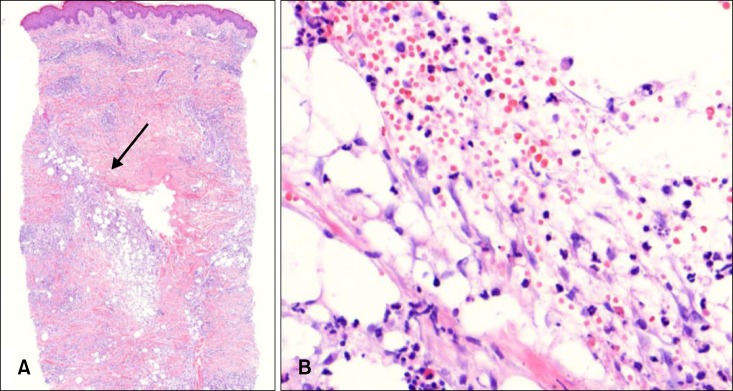
(A) A cavity with surrounding dense inflammatory cells infiltration and amorphous eosinophilic material (arrow) in the dermis (H&E, ×20). (B) Inflammatory cell infiltration composed of lymphocytes, neutrophil, and eosinophils in the dermis (H&E, ×400).
Ticks are blood-sucking ectoparasites that rely on hosts, such as reptiles, birds, mammals, and even humans1. Dermatoses by the tick's bite includes a pruritic papule, papular urticaria, subcutaneous hemorrhage, erythema chronicum migrans, lymphocytoma cutis, and others1. Tick bite and the related dermatoses have rarely been reported in Korea; however, reports are increasing because of the increasing popularity of outdoor activities2. Thirty-six cases of tick bite have been reported in Korea up to the present2-5. Histologically, most of the reported cases of tick bites showed a dense cellular infiltration composed of neutrophils, lymphocytes, and eosinphils in the dermis. In only two of the reported cases, apparent localized fat herniation was observed, with subcutaneous fat tissue and dermal collagen fibers pulled toward the upper dermis3. This finding is assumed to be caused by the blood-sucking motion of the tick3, and no similar finding had been mentioned in the Korean literature. In only one of the reported cases in the Korean literature, a typical intradermal cavity with eosinophilic necrotic tissue was reported4. Saliva of the ticks, secreted during the blood-sucking motion makes the cavity by a chemical reaction4. To the best of our knowledge, this is the first case of tick bite showing localized fat herniation with a typical intradermal cavity. We report a case of tick bite with characteristic and interesting histopathologic findings.
References
- 1.Cho BK, Kang H, Bang D, Kim SN, Hwang S, Song ES. Tick bites in Korea. Int J Dermatol. 1994;33:552–555. doi: 10.1111/j.1365-4362.1994.tb02894.x. [DOI] [PubMed] [Google Scholar]
- 2.Yun SK, Ko GB, Chon TH. Tick bite: report of a case and review of Korean cases. Korean J Dermatol. 2001;39:891–895. [Google Scholar]
- 3.Jeong E, Park HJ, Lee JY, Cho BK. Two cases of tick bite showing localized fat herniation response. Ann Dermatol. 2006;18:70–72. [Google Scholar]
- 4.Lee JY, Cho BK, Hyun JS, Lee SW, Choi MJ, Kim TY. A case of tick bite with formation of intradermal cavity. Korean J Dermatol. 2002;40:311–313. [Google Scholar]
- 5.Ko JH, Cho DY, Chung BS, Kim SI. Two human cases of tick bite caused by Ixodes nipponensis. Korean J Parasitol. 2002;40:199–203. doi: 10.3347/kjp.2002.40.4.199. [DOI] [PMC free article] [PubMed] [Google Scholar]