

Abstract
Background
Chronic spontaneous urticaria is a debilitating disease for the patients and often considered by the doctors a very difficult disease to treat. In 2009 the European Academy of Allergy and Clinical Immunology/Global Allergy and Asthma European network/European Dermatology Forum/World Allergy Organization (EAACI/GA2LEN/EDF/WAO) published a revised version of the guidelines for the treatment of urticaria which included an algorithm for the treatment.
Objective
The objective of this study was to examine the clinical effect and the practical use of the algorithm.
Methods
The study was performed as a case-series study of all newly referred patients to our urticaria clinic over a period of 18 months.
Results
Our results show that the single most important and efficient treatment of urticaria patients is up dosing non-sedating antihistamines as recommended by the EAACI/GA2LEN/EDF/WAO guidelines. We did not find any predicting factors for responders to the antihistamine treatment, but about one third of the patients did not respond to the up-dosing of the antihistamines.
Conclusion
Antihistamines seems to be the most efficient treatment for urticaria; other treatments such as montelukast, azathioprine, and mycophenolate mofetil may also be used, but only in combination with antihistamines and only in the case of an independent antihistamines treatment failure. The EAACI/GA2LEN/EDF/WAO guideline for the treatment of urticaria offers an efficient and simple guidelines for the treatment of urticaria.
Keywords: Guideline, Treatment, Urticaria
INTRODUCTION
Chronic urticaria is a challenge both for the patient and the doctor. It may seem as a trivial disease, but in reality it is severe and often debilitating. Apart from a constant or constantly relapsing tormenting itch, it also leads to the loss of both social life and jobs for the patient1-3. A systematic work-up and approach to treatment is highly needed for these patients4. A Joint initiative by The European Academy of Allergy and Clinical Immunology (EAACI), the European Union-funded network of excellence, the Global Allergy and Asthma European network (GA2LEN), the European dermatology forum (EDF) and the World Allergy Organization (WAO), has provided a thorough and systematic guidelines for classification and treatment of urticaria in 2006, updated in 20095,6.
Urticaria is characterized by a rapid appearance of wheals and/or angioedema. Wheals are characterized by a central swelling, itching or sometimes burning, with a short yet variable duration (1 to 24 hours). Angioedema, on the other hand, is a swelling of the lower dermis and the subcutis and might have a longer duration than the wheals (up to 72 hours)5,7,8.
Urticaria may be categorized into spontaneous urticaria, physical urticaria and other urticaria disorders. Spontaneous urticaria is divided into acute spontaneous urticaria with spontaneous wheals and/or angioedema for less than 6 weeks and chronic spontaneous urticaria (CSU) with a duration of 6 or more weeks. Physical urticaria includes various types of urticaria depending on the physical stimuli to be induced. Thus, there are acquired cold urticaria, delayed pressure urticaria, heat urticaria, solar urticaria, urticaria factitia and vibratory urticaria. The group of other urticaria disorders include aquagenic urticaria, cholinergic urticaria, contact urticaria and exercise induced anaphylaxis/urticaria5,7,8.
The diagnosis and the classification of urticaria is highly based on a thorough medical and personal history of the patient in which the eliciting factors of the urticaria is identified9. However, some paraclinical testing may aid the classification of the disease, including differential count and C-reactive protein (CRP)/erythrocyte sedimentation rate, a test for infections (Helicobacter Pylori, streptococci, staphylococci, Mycoplasma pneumonia, hepatitis virus and others), thyroid hormones and antibodies, a histamine release test (HR-test) or an autologous skin serums test. In the case of physical urticaria, cold provocation, heat provocation, light testing (ultra violet A and ultra violet B) may be used. For the other types of urticaria exercise, such as contact urticaria, a wet cloth or prick test, may be applied5.
The 2009 version of the EAACI/GA2LEN/EDF/WAO treatment guidelines include a stringent and easy to use flowchart for the treatment of urticaria (Fig. 1)6. What is clear from the treatment guidelines is the fact that there are very few treatments with a high level of evidence. Only those treatments with non-sedating second generation H1-antihistamines (ns sg AH1) have a strong evidence and recommendation for the means of intervention, whereas the use of ns sg AH1, in combination with cyclosporine, has a high quality of evidence but a low recommendation. The other treatment modalities are a result of the Consensus Meeting on Urticaria in 2008 and are based on the best available evidence, which, nonetheless, ranges from low to very low only.
Fig. 1.
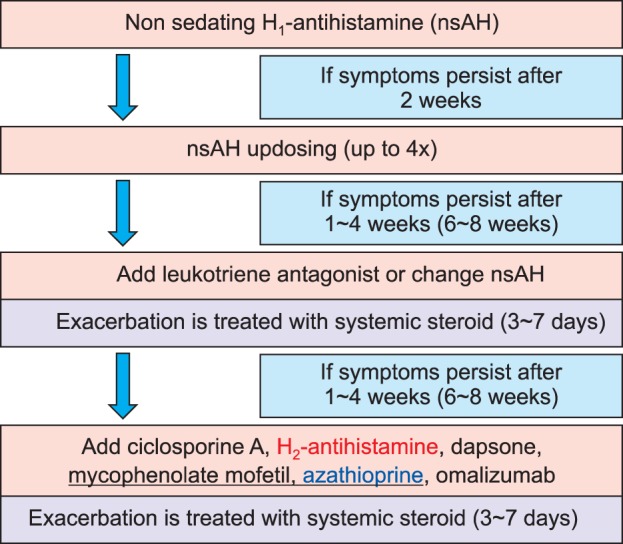
The treatment algorithm for urticaria adapted from the European Academy of Allergy and Clinical Immunology/Global Allergy and Asthma European network/European Dermatology Forum/World Allergy Organization (EAACI/GA2LEN/EDF/WAO) guidelines. The algorithm used in this study did not contain H2 blockers, and azathioprine was added.
Recently, it has been shown that patients with urticaria are often perceived as a time consuming and difficult to satisfy group of patients; every third patient is referred to a tertiary center for a treatment for their condition10. In the case of CSU, this is most viable option for the patients as these centers often have implemented the newest guidelines and have experience with alternative treatment options11.
In the autumn of 2009, we started a specialized clinic for patients with urticaria in order to standardize the treatment and diagnostic work-up in our department for these patients based on the recommendations of the EAACI/GA2LEN/EDF/WAO, although not in a protocolized manner. Over the course of the next 18 months, we registered the demographic data, previous treatment methods and paraclinical values for all new patients referred from either dermatologists or general practioners in the primary health care, as well as the result of our diagnostic work up and the treatment.
MATERIALS AND METHODS
Over a period of 18 months all newly referred patients, under the diagnosis of chronic spontaneous/idiopathic urticaria, from either primary care, e.g. general practitioners and dermatologists, or secondary care e.g. other hospital departments, were registered in a database, programed in Filemaker pro (Santa Clara, CA, USA). All available information including the age, sex, the number of visit, the total treatment time in our outpatient clinc, and the effect of a given treatment, were recorded along with paraclinical measurements such as thyroid stimulating hormone (TSH), antinuclear antibodies, HR-test, CRP, and hepatitis serology. The effect of the treatment was divided into: no effect, a partial effect, or good effect; it was based purely on the subjective classification of the patient. A partial effect means that the patient felt some improvement for the symptoms but not sufficient enough get back to their everyday routines. Good effect means that the patient felt enough improvement for the symptoms to be able to continue everyday life without the interference from urticaria symptoms. The timeframe between the visits/change of the treatment suggested by the EAACI/GA2LEN/EDF/WAO guidelines is shown in Fig. 1. As the patients were often seen at a little longer interval, as shown in parenthesis in Fig. 1, they were asked to evaluate the effect of the given treatment over the last 4 weeks.
The treatment algorithm for the CSU patients in this clinic was based on the one published by the EAACI/GA2LEN/EDF/WAO, with a few alterations (Fig. 1). Furthermore, the recommended time frame could not be followed for practical reasons. As the treatment was not protocolized, not all paraclinical values were measured in all the patients, and a deviation from the described treatment algorithm depended, to some measure, on the clinical situation and the discretion of the doctor.
The data was analysed using descriptive statistics (statistical program used was STATA; ATATACORP, College Station, TX, USA), t-test and chi square testing. This study was approved by the Danish National Data Protection Agency.
RESULTS
Age and sex distribution
In our observation period, the total number of newly referred patients from either primary care or other departments in the secondary care, was 85; 31 males and 54 females (p<0.05). The average age of the total population was 41.9 years (range ±6.79) (males: 42.5 [6 to 69], females 42.2 [10 to 79]). Fifty-six patients achieved a good effect after one visit, whereas 29 needed more than one visit to achieve a good or a partial effect (Fig. 2).
Fig. 2.
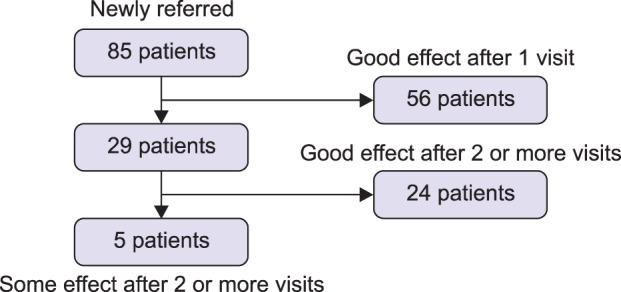
A flow chart of the patients registered in this study. The patients are subgrouped depending on the number of visits needed to obtain 'good effect'.
Treatment at referral
The distribution and the effect of the different treatment modalities at the time of the referral can be seen in Table 1. The most common treatment among the patients referred to the urticaria clinic was antihistamines. The other treatments included antihistamines combined with steroids (11) or azathioprine (1), systemic steroids alone (2), tranexamic acid (4) or no treatment at all (19). A certain number of the patients in each treatment group, except for the no treatment group, had a partial effect of their treatment (Table 1). There was no significant gender difference with regard to the treatment although in the group of no-treatment the men to women ratio was 3:16 (p=0.06).
Table 1.
Treatment at the time of referral

The treatment at the time of the referral is shown in the first row, and the total number of the patients receiving the treatment is shown in the second row. Below the effect of the treatment, at the time of the referral, is shown. AH: antihistamines, SS: systemic steroids, aza: azathioprine, Tranex: tranexamic acid.
Patients achieving 'good' effect after one visit
The number of patients achieving 'good' effect after one visit in the urticaria clinic (patients who, on their second visit, rated the effect of the treatment instigated on their first visit as 'good') was 56 (Table 2). The treatment these patients received, when they were referred, was not significantly different from the entire population of the referred patients; however, their treatment was changed significantly in order to obtain a good effect (Fig. 2) (p <0.01). Most notably the number of the patients receiving antihistamine increased (33 to 48) as well as the number of the patients receiving antihistamines and montelukast (0 to 6); on the other hand, the number of the patients receiving antihistamines and systemic corticosteroids was reduced from 6 to 1 (Table 2). The average time until 'good' effect obtained in this group was 87.3 days (13 to 274) which is significantly lower than the total time in the follow up for the patients in the group not achieving good effect at their first visit (p<0.05).
Table 2.
Treatment after one visit in the 'good' effect group

The treatment of the patients with 'good effect' after one visit. The top row shows the treatment, the second row the number of the patients receiving the treatment at the referral, and the third row shows the treatment after one visit. AH: antihistamines, SS: systemic steroids, aza: azathioprine, Tranex: tranexamic acid, mont: montelukast.
The role of antihistamines in obtaining good effect after one visit
Among the patients treated with anti histamines already at referral, 28 of the 33 (85%) achieved a 'good' effect simply by increasing the dose of the antihistamines (Table 3). Among the patients who did not receive the antihistamine treatment, or the antihistamine treatment in combination with either systemic steroids or azathioprine, 20 of the 23 patients achieved a good effect after their treatment was changed to antihistamines. Antihistamines combined with montelukast were a good treatment for 6 patients (4 treated with antihistamines, 1 with systemic steroids and 1 with tranexamic acid at the time of referral) (Table 3, 4).
Table 3.
Effect of 'up-dosing' antihistamines
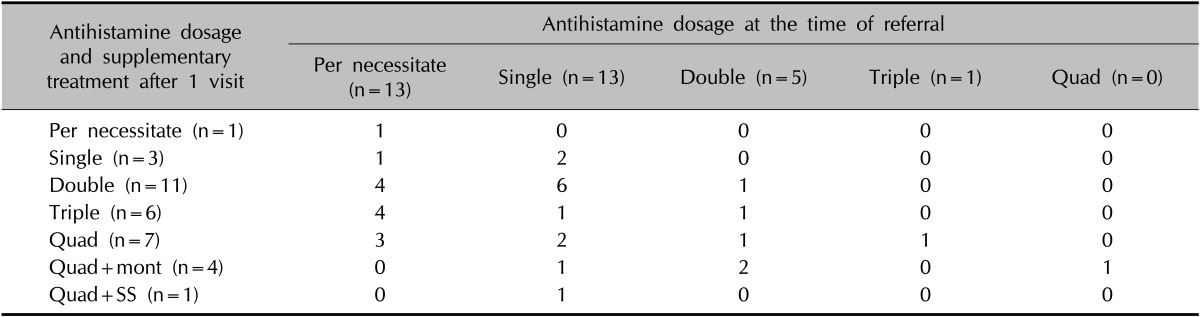
Patients in antihistamine treatment before and after the first visit with 'good effect' after one visit. The top row groups the patients according to the dosage of antihistamine at the time of the referral and shows the number of the patients. The numbers in each column below show the number of the patients receiving a specified antihistamine dosage and the supplementary treatment described in the left column, after the first visit. Quad: quadruple, mont: montelukast, SS: systemic steroids.
Table 4.
Effect of introducing antihistimines
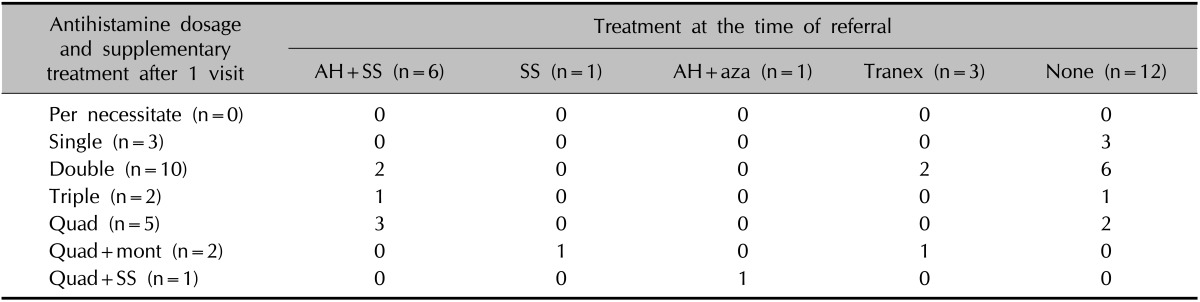
Patients successfully treated with antihistamines after one visit but not on the antihistamine treatment at the time of the referral. The top row groups the patients according to the treatment at the time of the referral and shows the number of the patients. The numbers in each column below show the number of the patients receiving a specified antihistamine dosage and the supplementary treatment described in the left column, after the first visit. AH: antihistamines, SS: systemic steroids, aza: azathioprine, Tranex: tranexamic acid, Quad: quadruple, mont: montelukast.
Patients needing more than one visit to obtain a 'good' or 'partial' effect
The 29 patients needing more than one visit to obtain a good or a partial effect needed an average of 309.3 (42 to 554) days of treatment. There was no significant difference in the treatment these patients received at the time of the referral compared to the group of the patients needing only one visit to obtain a 'good' effect. However, the number of the patients needing another treatment than antihistamines to obtain a 'good effect' differed significantly from the patients needing only one visit (p<0.05). Of the 24 patients with a good effect after 2 or more visits 9 were treated with a high dose of antihistamines 3 with antihistamines in combination with azathioprine, 3 in combination with mycophenolate mophetil, 7 with antihistamines and montelukast, 1 with an H. pylori eradication, and finally, one patient ultimately needed a treatment with omalizumab.
Paraclinical values
A basophil HR-test was performed on 70 patients, and only found positive in 11. There was no significant correlation with either treatment needed, age, or sex. TSH was measured in 77 patients and all were found normal. Antinuclear antibodies were measured in 44 patients and 4 were found positive, yet only slightly and with no clinical significance. Again, no correlation to the CSU was found. Hepatitis serology was measured in 15 patients, but only one patient had a positive hepatitis B serology, and this was due to vaccination.
DISCUSSION
Many consider the approach to the patient suffering from a CSU very difficult. The patients have often undergone many clinical tests, especially for allergies, and have often been subjected to various diets to no visible effect. They may have been treated with antihistamines, which is also the case in our population, but often in insufficient dosages and without any sufficient effect.
The EAACI/GA2LEN/EDF/WAO treatment guidelines include a treatment algorithm, and the purpose of this study was to use these guidelines in an everyday clinical setting and evaluate its effect and efficacy. We included 85 patients referred to Aarhus University Hospital from a primary or a secondary care over a period of 18 months. The treatment followed the guidelines, not in a protocolized manner, but rather at the doctors discretion. The patients were divided into two subgroups according to the number of visits needed before a good treatment response was obtained. Thus 66% (56/85) of the patients needed only one visit before a good effect on their symptoms was obtained. A bias might be that the urticaria simply resolved spontaneously. However, given the fact that the average duration of urticaria symptoms before the referral was 2.9 years, it is hard not to attribute the resolvement of the symptoms to the treatment. The majority of these patients were treated with antihistamines before the referral, but in insufficient dosages since 28 of the 33 patients in this treatment benefitted sufficiently from an increase in the antihistamine dosage. Among the patients not in an antihistamine treatment at the time of the referral (antihistamines plus systemic steroids, tranexamic acid and systemic steroids) 20 out of the 23 had a sufficient effect from an antihistamine treatment ranging from a single to quadruple dosage. Thus, it seems that the first step on the EAACI/GA2LEN/EDF/WAO treatment guidelines with a steady and perhaps an increased dosage of antihistamines has a very good effect in a clinical setting. This is also a safe treatment12.
A minority of the patients needed more than one visit in order to obtain sufficient effect of the treatments prescribed. At the time of the referral, there was no significant difference in the distribution of the treatment modalities in this group of patients compared to the group of patients needing only one visit. However, the number of the patients needing another treatment than antihistamines significantly increased in the group of the patients needing more than one visit to obtain sufficient effect than in the group needing only one visit. This is a logical consequence of the treatment algorithm since the patients treated with antihistamines had the dosage increased or shifted to another treatment if the antihistamines did not have sufficient effect after one visit. An interesting observation, though, is that a large proportion (7/24) of the patients benefitted from adding montelukast to their antihistamine treatment (Table 5). The most recent addition in the selection of drugs for the treatment of CSU omlizumab13 was only used once in this material, but the use has increased significantly over the last years.
Table 5.
Treatments needed by more than one visit

Patients needing more than one visit before achieving 'good' effect. The first row shows the treatment, the second the number of the patients receiving the treatment at the time of the referral, and the third the treatment at the time 'good' or 'some' effect is achieved. AH: antihistamines, SS: systemic treatment, aza: azathioprine, Tranex: tanexamic acid, mont: montelukast, mycoph: mycophenolate, H. Pyl. err: Helicobactor pylori eradication therapy.
Another interesting observation is that neither the treatment at the time of the referral nor the paraclinical values nor the age or gender could predict if the CSU would be treatment resistant or treatable after only one visit. This is consistent with other observations14,15.
From our observational study we must conclude that if a stringent treatment algorithm is adhered to, the majority of urticaria patients can obtain sufficient treatment effect after only one visit to a tertiary centre. Antihistamines are the mainstay therapy, and in the majority of the CSU patients, an increased dosage of antihistamines often resolves symptoms. As of yet there is no predictive paraclinical or clinical test for the duration or the treatment of CSU.
References
- 1.Grob JJ, Revuz J, Ortonne JP, Auquier P, Lorette G. Comparative study of the impact of chronic urticaria, psoriasis and atopic dermatitis on the quality of life. Br J Dermatol. 2005;152:289–295. doi: 10.1111/j.1365-2133.2005.06385.x. [DOI] [PubMed] [Google Scholar]
- 2.O'Donnell BF, Lawlor F, Simpson J, Morgan M, Greaves MW. The impact of chronic urticaria on the quality of life. Br J Dermatol. 1997;136:197–201. [PubMed] [Google Scholar]
- 3.Maurice-Tison S, Pouyanne J, Doutre MS. General practitioners, dermatologists, allergists, and the management of chronic urticaria. Results of a practice survey. Ann Dermatol Venereol. 2003;130:1S160–1S173. [PubMed] [Google Scholar]
- 4.Grattan C. The urticarias: pathophysiology and management. Clin Med. 2012;12:164–167. doi: 10.7861/clinmedicine.12-2-164. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Zuberbier T, Asero R, Bindslev-Jensen C, Walter Canonica G, Church MK, Giménez-Arnau A, et al. Dermatology Section of the European Academy of Allergology and Clinical Immunology; Global Allergy and Asthma European Network; European Dermatology Forum; World Allergy Organization. EAACI/GA(2)LEN/EDF/WAO guideline: definition, classification and diagnosis of urticaria. Allergy. 2009;64:1417–1426. doi: 10.1111/j.1398-9995.2009.02179.x. [DOI] [PubMed] [Google Scholar]
- 6.Zuberbier T, Asero R, Bindslev-Jensen C, Walter Canonica G, Church MK, Giménez-Arnau AM, et al. Dermatology Section of the European Academy of Allergology and Clinical Immunology; Global Allergy and Asthma European Network; European Dermatology Forum; World Allergy Organization. EAACI/GA(2)LEN/EDF/WAO guideline: management of urticaria. Allergy. 2009;64:1427–1443. doi: 10.1111/j.1398-9995.2009.02178.x. [DOI] [PubMed] [Google Scholar]
- 7.Grattan CE, Sabroe RA, Greaves MW. Chronic urticaria. J Am Acad Dermatol. 2002;46:645–657. doi: 10.1067/mjd.2002.122759. [DOI] [PubMed] [Google Scholar]
- 8.Zuberbier T, Maurer M. Urticaria: current opinions about etiology, diagnosis and therapy. Acta Derm Venereol. 2007;87:196–205. doi: 10.2340/00015555-0240. [DOI] [PubMed] [Google Scholar]
- 9.Wedi B, Kapp A. Evidence-based therapy of chronic urticaria. J Dtsch Dermatol Ges. 2007;5:146–157. doi: 10.1111/j.1610-0387.2007.06074.x. [DOI] [PubMed] [Google Scholar]
- 10.Weller K, Viehmann K, Bräutigam M, Krause K, Siebenhaar F, Zuberbier T, et al. Cost-intensive, time-consuming, problematical? How physicians in private practice experience the care of urticaria patients. J Dtsch Dermatol Ges. 2012;10:341–347. doi: 10.1111/j.1610-0387.2011.07822.x. [DOI] [PubMed] [Google Scholar]
- 11.Weller K, Schoepke N, Krause K, Ardelean E, Bräutigam M, Maurer M. Selected urticaria patients benefit from a referral to tertiary care centres--results of an expert survey. J Eur Acad Dermatol Venereol. 2013;27:e8–e16. doi: 10.1111/j.1468-3083.2011.04387.x. [DOI] [PubMed] [Google Scholar]
- 12.Staevska M, Popov TA, Kralimarkova T, Lazarova C, Kraeva S, Popova D, et al. The effectiveness of levocetirizine and desloratadine in up to 4 times conventional doses in difficult-to-treat urticaria. J Allergy Clin Immunol. 2010;125:676–682. doi: 10.1016/j.jaci.2009.11.047. [DOI] [PubMed] [Google Scholar]
- 13.Ivyanskiy I, Sand C, Thomsen SF. Omalizumab for chronic urticaria: a case series and overview of the literature. Case Rep Dermatol. 2012;4:19–26. doi: 10.1159/000336205. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Kulthanan K, Jiamton S, Thumpimukvatana N, Pinkaew S. Chronic idiopathic urticaria: prevalence and clinical course. J Dermatol. 2007;34:294–301. doi: 10.1111/j.1346-8138.2007.00276.x. [DOI] [PubMed] [Google Scholar]
- 15.Toubi E, Kessel A, Avshovich N, Bamberger E, Sabo E, Nusem D, et al. Clinical and laboratory parameters in predicting chronic urticaria duration: a prospective study of 139 patients. Allergy. 2004;59:869–873. doi: 10.1111/j.1398-9995.2004.00473.x. [DOI] [PubMed] [Google Scholar]