

Abstract
Objective:
To analyze the epidemiology of pterygium in a hospital-based population in Alkhobar, which is located in the eastern province of Saudi Arabia.
Materials and Methods:
This was a retrospective, non-randomized, and consecutive case study. Out of 88,666 patients who were seen in the ophthalmology clinic between January 1995 through the end of December 2010, 116 patients were diagnosed with advanced pterygium. The medical records of these patients were evaluated.
Results:
The overall prevalence of pterygium was found to be 0.074%. There was no significant difference by either gender, side, or by laterality (P > 0.05). A significant increase was noticed in the prevalence of pterygium with increasing age and nasal location (P < 0.05).
Conclusion:
The overall prevalence rate of pterygium in Alkhobar is low when compared with results reported from other areas of the world.
Keywords: Alkhobar, hospital-based, prevalence, pterygium, Saudi Arabia
INTRODUCTION
Pterygium is a wing-shaped, fleshy growth, and invasive extraocular lesion located most commonly in the nasal part of the limbus extending onto the cornea. This disease occurs throughout the world, and the prevalence rates vary widely from 1.2% to 23.4%.[1,2,3,4] The exact etiology and pathogenesis of pterygium remains unclear, but it is more common in people with excessive outdoor exposure to sunlight and wind, such as those who work outdoors. Pterygium is of great concern to both surgeons and patients, as it has been shown to recur in up to 97% of patients within one year after surgical removal.[5] Over the past years, several population-based studies have shown higher rates of pterygium in countries near the Equator.[6,7,8,9,10,11] These rates have been linked to excessive UV exposure that induces oxidative stress and expression of cytokines and growth factors in pterygial epithelial cells, which initiates cellular proliferation, blood vessel formation, tissue invasion, and inflammation.[11,12,13,14]
Recent reports have also indicated an association of pterygium with dry, warm, and dusty climates, and high winds and genetic predisposition.[9,15]
In this study, we aim to assess the prevalence and risk factors of advanced pterygium in Alkhobar in the eastern province of Saudi Arabia, where such data has not been previously available.
MATERIALS AND METHODS
This investigation is a hospital-based study, which took place at King Fahd Hospital at the university in Alkhobar, which serves as referral hospital for a population of 3,360,031 occupying the eastern province region. Alkhobar (26° 18’N, 50° 12’E) is located in the eastern region of Saudi Arabia. It has a desert climate with very hot, humid summers and cold, dry winters. The average altitude of Alkhobar is 6 m above sea level, and its average annual temperature is 33°C.
We retrospectively investigated cases attended the ophthalmology clinics at King Fahd Hospital of the University in Alkhobar during a 15-year period from January 1995. A total of 116 (131 eyes) patients were diagnosed with advanced pterygium (i.e., pterygium that has crossed half way toward the visual axis an imaginary line between the periphery of the cornea and the pupillary border) during that period, with the permissions of the research committees of both the College of Medicine, Dammam University, and KFHU, Al Khobar, Saudi Arabia. The necessary statistical analyses (parametric or non-parametric) to examine the relationship between variables were implemented, and a P value of <0.05 was considered significant.
RESULTS
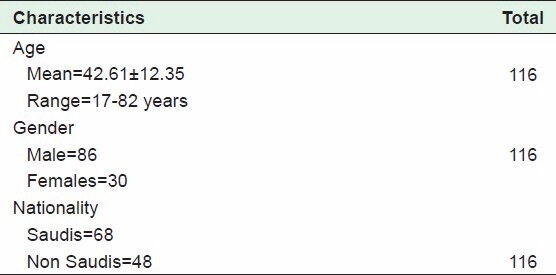
A total of 88,666 patients were seen in the ophthalmology clinic during a 15-year period from January 1995 through December 2010. A total of 116 patients had an advanced pterygium with a mean age of 42.61 ± 12.35 (age range: 17-82 years). The number of Saudis were 68 (58.6%) versus non-Saudis 48 (41.3%) [Table 1]. The total number of eyes with primary advanced pterygium were 110 (84%) versus 21 (16%) recurrent pterygium. The prevalence rate of advanced pterygium was 0.074%.
Table 1.
Demographic data of patients with advanced pterygium
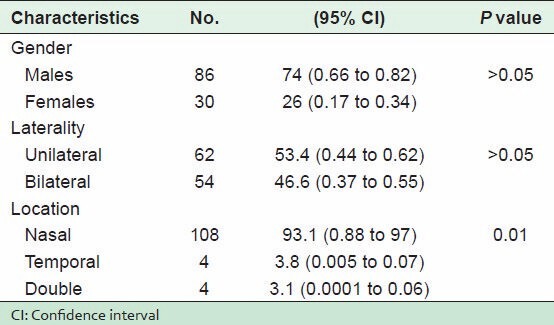
There was no significant difference in the rates of pterygium by side: Right, 52% (95% CI: 0.43 to 0.61); left, 48% (95% CI: 0.4 to 0.57); P > 0.05. The rates for men and women were 74% (95% CI: 0.66 to 0.82) and 26% (95% CI: 0.17 to 0.34), respectively, also demonstrating no statistically significant difference; P > 0.05. There was no significant difference in the rate of pterygium by laterality: Unilateral, 53.4% (95% CI: 0.44 to 0.62); bilateral 46.6% (95% CI: 0.37 to 0.55); P > 0.05. The prevalence rate increased obviously with age: Middle and older group (≥30-82 y), 81% (95% CI: 0.64 to 0.98); younger group (<30 y), 19% (95% CI: 0.11 to 0.26); P = 0.006 [Table 2]. The rate of nasal pterygium 93.1% (0.88 to 97) was more significant than both temporal pterygium 3.8% (0.005 to 0.07) and double pterygium 3.0% (0.0001 to 0.06); P = 0.01 [Table 3].
Table 2.
Prevalence rate of pterygium according to age

Table 3.
Characteristics of advanced pterygium
DISCUSSION
The prevalence rates of pterygium from various studies show considerable variation, ranging from 0.3% to 33.1%, depending on factors such as age, sex, race, and geography.[2,15,16,17,18,19] There are a few comparable studies showing low prevalence rates of pterygium. In such studies, the prevalence rates were 1.3% in Tehran,[17] 1% in Kyoto,[20] 2.83% in Victoria,[21] and 2.88% in Beijing.[19] This study showed the prevalence rate of pterygium in Alkhobar to be lower than in the previous studies; the overall prevalence of pterygium was 0.074%. This low rate is due to the inclusion of only the advanced pterygia (pterygium amenable to surgical treatment) in the study.
Recent reports demonstrated a relationship between UVB light and pterygium.[6,7,14,22] It was seen that the populations living at high altitudes (above 3000 m) were exposed to high UVB sunlight and had high prevalence rates of pterygium. In an aged Mongolian population living in Henan County, where the average altitude was 3450 m, the prevalence of pterygium was 17.0%.[23] In Zeku County, China, with an average altitude of 3700 m, the prevalence of pterygium was 14.49%.[16] The altitude of the location of this study was 6 m, which is low. This could be one of the factors that might explain the low prevalence of pterygium in Alkhobar.
Several studies reported a positive association between increasing age and the presence of pterygium. A study of a tropical islands in the Riau Archipelago, Indonesia, demonstrated a significantly higher average age of subjects with pterygium (42.8 years) compared to those without (18.6 years).[2] In Victoria, Australia, the prevalence of pterygium increased from 2.83% in persons aged 40 years to 6.45% among those aged 80-89 years.[21] A similar trend was reported in the Central Sahara in Africa with prevalence increasing from 1.1% in subjects aged 2-19 years to 13.0% in subjects aged 40-87 years.[24] In this study, we also demonstrated an increase in the prevalence of pterygium with increasing age [Table 2]. We found that the prevalence of pterygium was 19% in those ≥30 y, but 81% for those ≥30-82 years.
The prevalence between genders in this study was not significant and also the prevalence for laterality was not significant, whereas regarding location, nasal pterygium was more significant than both temporal and double pterygium [Table 3]. Similar results were found by Lu et al. in China,[23] Viso et al. in Spain,[25] Gazzard et al. in Indonesia,[26] Forsius et al. in Rwanda,[27] Sarac et al. in Turkey.[28]
To the best of our knowledge, this was the first study to examine the prevalence of pterygium in Alkhobar city in the eastern province of Saudi Arabia.
In conclusion, this study demonstrates the prevalence of pterygium according to age and gender in Alkhobar in the eastern province of Saudi. When we compare the results with reported findings from other areas of the world, our study shows a lower prevalence rate of pterygium, which might be due to low altitude and a positive association with age. Further cross-sectional, prospective, population-based studies are suggested to monitor the prevalence of pterygium and other risk factors in Saudi.
ACKNOWLEDGMENT
The author would like to thank Dr. Amar Hassan Khamis, Associate Professor of Biostatistics and Genetic Epidemiology, Department of Family and Community Medicine University of Dammam for his help in statistical analysis.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
REFERENCES
- 1.West S, Muñoz B. Prevalence of pterygium in Latinos: Proyecto VER. Br J Ophthalmol. 2009;93:1287–90. doi: 10.1136/bjo.2008.152694. [DOI] [PubMed] [Google Scholar]
- 2.Tan CS, Lim TH, Koh WP, Liew GC, Hoh ST, Tan CC, et al. Epidemiology of pterygium on a tropical island in the Riau Archipelago. Eye. 2006;20:908–12. doi: 10.1038/sj.eye.6702046. [DOI] [PubMed] [Google Scholar]
- 3.Luthra R, Nemesure BB, Wu SY, Xie SH, Leske MC Barbados Eye Studies Group. Frequency and risk factors for pterygium in the Barbados Eye Study. Arch Ophthalmol. 2001;119:1827–32. doi: 10.1001/archopht.119.12.1827. [DOI] [PubMed] [Google Scholar]
- 4.Al-Bdour M, Al-Latayfeh MM. Risk factors for pterygium in an adult Jordanian population. Acta Ophthalmol Scand. 2004;82:64–7. doi: 10.1046/j.1600-0420.2003.0213.x. [DOI] [PubMed] [Google Scholar]
- 5.Hirst LW, Sebban A, Chant D. Pterygium recurrence time. Ophthalmology. 1994;101:755–8. doi: 10.1016/s0161-6420(94)31270-x. [DOI] [PubMed] [Google Scholar]
- 6.Moran DJ, Hollows FC. Pterygium and ultraviolet radiation: A positive correlation. Br J Ophthalmol. 1984;68:343–6. doi: 10.1136/bjo.68.5.343. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Taylor HR, West S, Munoz B, Rosenthal FS, Bressler SB, Bressler NM. The long- term effects of visible light on the eye. Arch Ophthalmol. 1992;110:99–104. doi: 10.1001/archopht.1992.01080130101035. [DOI] [PubMed] [Google Scholar]
- 8.Ang LP, Chua JL, Tan DT. Current concepts and techniques in pterygium treatment. Curr Opin Ophthalmol. 2007;18:308–13. doi: 10.1097/ICU.0b013e3281a7ecbb. [DOI] [PubMed] [Google Scholar]
- 9.Singh G. Pterygium in the tropics. Ophthalmology. 1990;97:542–3. [PubMed] [Google Scholar]
- 10.Sliney DH. Geometrical gradients in the distribution of temperature and absorbed ultraviolet radiation in ocular tissues. Dev Ophthalmol. 2002;35:40–59. doi: 10.1159/000060809. [DOI] [PubMed] [Google Scholar]
- 11.Balci M, Þahin Þ, Mutlu FM, Yaðci R, Karanci P, Yildiz M. Investigation of oxidative stress in pterygium tissue. Mol Vis. 2011;17:443–7. [PMC free article] [PubMed] [Google Scholar]
- 12.Kria L, Ohira A, Amemiya T. Immunohistochemical localization of basic firoblast growth factor, platelet derived factor, transforming growth factor beta and tumor necrosis factor alpha in the pterygium. Acta Histochem. 1996;98:195–201. doi: 10.1016/s0065-1281(96)80038-9. [DOI] [PubMed] [Google Scholar]
- 13.Jin J, Guan M, Sima J, Gao G, Zhang M, Liu Z, et al. Decreased pigment epithelium derived factor and increased vascular endothelial growth factor levels in pterygia. Cornea. 2003;22:473–7. doi: 10.1097/00003226-200307000-00015. [DOI] [PubMed] [Google Scholar]
- 14.Di Girolamo N, Wakefield D, Coroneo MT. UVB-mediated induction of cytokines and growth factors in pterygium epithelial cells involves cell surface receptors and intracellular signaling. Invest Ophthalmol Vis Sci. 2006;47:2430–7. doi: 10.1167/iovs.05-1130. [DOI] [PubMed] [Google Scholar]
- 15.Solomon AS. Pterygium. Br J Ophthalmol. 2006;90:665–6. doi: 10.1136/bjo.2006.091413. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Lu P, Chen X, Kang Y, Ke L, Wei X, Zhang W. Pterygium in Tibetans: A population-based study in China. Clin Experiment Ophthalmol. 2007;35:828–33. doi: 10.1111/j.1442-9071.2007.01630.x. [DOI] [PubMed] [Google Scholar]
- 17.Fotouhi A, Hashemi G, Khabazkhoob M, Mohammad K. Prevalence and risk factors of pterygium and pinguecula: The Tehran Eye Study. Eye. 2009;23:1125–9. doi: 10.1038/eye.2008.200. [DOI] [PubMed] [Google Scholar]
- 18.Paula JS, Thorn F, Cruz AA. Prevalence of pterygium and cataract in indigenous populations of the Brazilian Amazon rain forest. Eye. 2006;20:533–6. doi: 10.1038/sj.eye.6701917. [DOI] [PubMed] [Google Scholar]
- 19.Ma K, Xu L, Jie Y, Jonas JB. Prevalence of and factors associated with pterygium in adult Chinese: The Beijing Eye Study. Cornea. 2007;26:1184–6. doi: 10.1097/ICO.0b013e318151f9c6. [DOI] [PubMed] [Google Scholar]
- 20.Norn M. Spheroid degeneration, keratopathy, pinguecula, and pterygium in Japan (Kyoto) Acta Ophthalmol (Copenh) 1984;62:54–60. doi: 10.1111/j.1755-3768.1984.tb06756.x. [DOI] [PubMed] [Google Scholar]
- 21.McCarty CA, Fu CL, Taylor HR. Epidemiology of pterygium in Victoria, Australia. Br J Ophthalmol. 2000;84:289–92. doi: 10.1136/bjo.84.3.289. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Dushku N, John MK, Schultz GS, Reid TW. Pterygia pathogenesis: Corneal invasion by matrix metalloproteinase expressing altered limbal epithelial basal cells. Arch Ophthalmol. 2001;119:695–706. doi: 10.1001/archopht.119.5.695. [DOI] [PubMed] [Google Scholar]
- 23.Lu J, Wang Z, Lu P, Chen X, Zhang W, Shi K, et al. Pterygium in an aged Mongolian population: A population-based study in China. Eye. 2009;23:421–7. doi: 10.1038/sj.eye.6703005. [DOI] [PubMed] [Google Scholar]
- 24.Bueno-Gimeno I, Montes-Mico R, Espana-Gregori E, Pons AM. Epidemiologic study of pterygium in a Saharan population. Ann Ophthalmol. 2002;34:43–6. [Google Scholar]
- 25.Viso E, Gude F, Rodriguez-Ares MT. Prevalence of pinguecula and pterygium in a general population in Spain. Eye. 2011;25:350–7. doi: 10.1038/eye.2010.204. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Gazzard G, Saw SM, Farook M, Koh D, Widjaja D, Chia SE, et al. Pterygium in Indonesia: Prevalence, severity and risk factors. Br J Ophthalmol. 2002;86:1341–6. doi: 10.1136/bjo.86.12.1341. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Forsius H, Maertens K, Fellman J. Changes of the eye caused by the climate in Rwanda, Africa. Ophthalmic Epidemiol. 1995;2:107–13. doi: 10.3109/09286589509057090. [DOI] [PubMed] [Google Scholar]
- 28.Sarac O, Toklu Y, Sahin M. The prevalence of pterygium in Ankara: A hospital-based study. Turk J Med Sci. 2012;42:1006–9. [Google Scholar]