

Abstract
We report the case of a 50-year old man diagnosed with intracardiac migration of a Kirschner wire (K-wire). The patient had undergone surgical fixation of rib fracture 32 months previously. Chest roentgenograms, chest computed tomographic scans and echocardiography revealed that one of the K-wires had migrated to the right ventricle. The K-wire was removed immediately. To the best of our knowledge, this is the first reported instance of asymptomatic intracardiac migration of a K-wire from the right rib.
Keywords: Foreign body, Right ventricle, Kirschner wire, Intracardiac migration
INTRODUCTION
Orthopaedic metallic wires and pins are frequently used for the fixation of fractures and dislocations. Migration of orthopaedic wires to solid organs or body cavities has been reported in the literature. We report here the first case of silent migration of a Kirschner wire (K-wire) used in the right rib fixation to the right ventricle.
CASE REPORT
A 50-year old man underwent surgical fixation of rib fracture with four K-wires 32 months ago. Three weeks after fixation, chest roentgenograms confirmed satisfactory stabilization and the K-wires were in a good position (Fig. 1A). Notably, one of the four K-wires was not bent over at the distal end (Fig. 1A). The patient was then discharged from hospital. He was then lost to the follow-up. Thirty-two months later, he presented to a local hospital for check-ups. A comparison of the postoperative (Fig. 1A) and current (Fig. 1B) routine upright anterior–posterior chest roentgenogram revealed that one of the K-wires had migrated from the right third rib into the left thorax, over the cardiac silhouette (Fig. 1B). The chest computed tomographic scan localized the object to within the right ventricle (Fig. 1C). Transthoracic echocardiography showed a highly echogenic, linear object in the right ventricle, as well as tricuspid regurgitation, but no pericardial effusion. He denied any recent cough, chest pain, haemoptysis, hemosputum, irregular heartbeat, fever or chills since the insertion of the K-wires.
Figure 1:

(A) Postoperative chest roentgenogram after surgical stabilization of rib fractures with four K-wires (see arrow). (B) Chest roentgenogram revealed a metallic foreign body (arrow) located over the cardiac silhouette and demonstrated the absence of the top K-wire of the right chest. (C) The chest computed tomographic scan showed a migrated wire (arrow) located in the right ventricle.
The patient was transferred to our hospital and surgical removal of the K-wire was immediately planned. A median sternotomy was performed and the ascending aorta and both vena cavae were cannulated in the standard way for cardiopulmonary bypass. Fibrillation was induced and a nearly 8-cm-long K-wire was removed through a small right ventricular incision (Fig. 2). During the same operation, the remaining K-wires were removed from the right ribs. The patient made an uneventful recovery and was discharged from hospital 7 days postoperatively.
Figure 2:
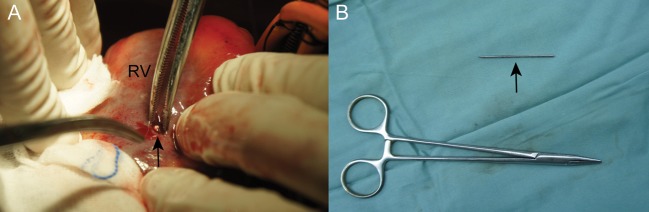
Intraoperative photograph: (A) The K-wire was located in the right ventricle. It was removed through a small right ventricular incision (arrow). (B) The extirpated K-wire was unbent with a sharp point and was nearly 8 cm long. RV: right ventricle.
DISCUSSION
Migration of a K-wire into the heart has been rarely reported. The most common primary site of fixation where migration often occurred was the sternoclavicular joint, followed by the clavicle, the acromioclavicular joint and the proximal humerus [1]. The intracardiac migration of a K-wire from the pelvic bone [2], the femur [3] and the finger [4] has also been reported. In the present case, the wire had been used for the fixation of the right third rib and its migration had caused embolization of the right ventricle. To the best of our knowledge, this is the first report in the literature so far.
To date, almost all patients with intracardiac migration of wires or pins presented with acute symptoms [1–5]. In this case, the wire did not cause particular symptoms and the diagnosis was made after a routine examination. There occurred no cough, chest pain, haemoptysis, hemosputum, irregular heartbeat, fever or chills. The mechanism of this silent migration into the right heart is not entirely clear. Although mechanisms that include respiratory excursion or gravitational forces may be proposed, we assume that the wire embolized the heart from a peripheral vein, most likely the right subclavian vein, and ultimately lodged in the right ventricle [1–5]. The migration of the wire through the bone was probably slow, and the timing of the wire embolization to the heart is uncertain.
It has been recommended that the pin should be removed immediately if the follow-up roentgenograms show any signs of migration of wires and pins. Although this patient did not have cardiac symptoms and showed no evidence of thrombus or bacterial endocarditis, he needed removal of the foreign body because of potential injury to the cardiac structures. We began the removal operation immediately to prevent sudden death due to heart perforation and pericardial tamponade.
It is worth emphasizing again that the distal end of each K-wire must be bent sufficiently when this device is used for fixation of fractures, and a restraining device should be used in conjunction with it. In our case, one of the four K-wires that was not bent over, migrated and embolized in the heart (Fig. 1A and B). Close clinical and radiographic postoperative follow-up examinations are also important after insertion of orthopaedic wires, which should be withdrawn once treatment has been concluded. If intracardiac wire migration is identified, it should be removed as a matter of urgency regardless of symptoms.
Funding
This study was supported by National Natural Science Foundation of China, grant number 81200087.
Conflict of interest: none declared.
REFERENCES
- 1.Freund E, Nachman R, Gips H, Hiss J. Migration of a Kirschner wire used in the fixation of a subcapital humeral fracture, causing cardiac tamponade: case report and review of literature. Am J Forensic Med Pathol. 2007;28:155–6. doi: 10.1097/PAF.0b013e31806195a1. [DOI] [PubMed] [Google Scholar]
- 2.Park SY, Kang JW, Yang DH, Lim TH. Intracardiac migration of a Kirschner wire: case report and literature review. Int J Cardiovasc Imaging. 2011;27:85–8. doi: 10.1007/s10554-011-9977-0. [DOI] [PubMed] [Google Scholar]
- 3.Ono M, Goerler H, Boethig D, Breymann T. Surgical removal of Kirschner wire from the right ventricle, migrated from the femur. Eur J Cardiothorac Surg. 2010;37:486. doi: 10.1016/j.ejcts.2009.08.022. [DOI] [PubMed] [Google Scholar]
- 4.Haapaniemi TA, Hermansson US. Cardiac arrhythmia caused by a Kirschner wire inside the heart: an unusual complication of finger osteosynthesis. J Hand Surg Br. 1997;22:402–4. doi: 10.1016/s0266-7681(97)80412-3. [DOI] [PubMed] [Google Scholar]
- 5.Actis Dato GM, Arslanian A, Di Marzio P, Filosso PL, Ruffini E. Posttraumatic and iatrogenic foreign bodies in the heart: report of fourteen cases and review of the literature. J Thorac Cardiovasc Surg. 2003;126:408–14. doi: 10.1016/s0022-5223(03)00399-4. [DOI] [PubMed] [Google Scholar]