

Abstract
Background and Objectives
High dose rosuvastatin loading before percutaneous coronary interventions (PCI) reduces the myocardial damage and the incidence of adverse cardiac events in patients with stable angina and acute coronary syndrome. However, no studies are present yet about rosuvastatin loading in patients with ST-segment elevation myocardial infarction (STEMI) in a primary PCI setting.
Subjects and Methods
A total of 475 patients who underwent primary PCI for STEMI were studied. The study population was divided into two groups with 208 patients in the statin group=40 mg rosuvastatin loading before primary PCI and 267 patients in the control group=no statin pretreatment. At median 3 days after PCI a single-photon emission computed tomography (SPECT) was performed with technetium 99m tetrofosmin For this study were compared infarct size, corrected Thrombolysis in Myocardial Infarction (TIMI) frame count and the myocardial blush grade (MBG) between the both groups.
Results
Baseline clinical and procedural characteristics were similar between the groups. Infarct size, as assessed by SPECT, was significantly smaller (19.0±15.9% vs. 22.9±16.5%, p=0.009) in the statin group than in the control group. Patients of the statin group showed a lower corrected TIMI frame count (28.2±19.3 vs. 32.6±21.4, p=0.020), and higher MBG (2.49±0.76 vs. 2.23±0.96, p=0.001) than the patients of the control group. The multivariate analysis revealed that rosuvastatin loading {odds ratio (OR) 0.61}, pain to balloon time (OR 2.05), anterior myocardial infarction (OR 3.89) and final the MBG (OR 2.93) were independent predictors of a large infarct size.
Conclusion
A high dose rosuvastatin loading before the primary PCI reduced the infarct size by microvascular myocardial perfusion improvement.
Keywords: Angioplasty, Myocardial infarction, Stents, Hydroxymethylglutaryl-CoA Reductase inhibitors
Introduction
The benefits of statin in the primary and secondary prevention for coronary artery diseases are well established.1),2),3),4),5) Clinical studies showed in the era of percutaneous coronary intervention (PCI) a high dose statin loading before a PCI may improve the clinical outcomes in patients with stable angina and acute coronary syndrome (ACS) with a reduction of periprocedural myocardial damage.6),7),8) The positive effects of statin pretreatment on clinical outcomes may be dependent on the periprocedural inflammatory status.8),9) According to the Novel Approaches for Preventing or Limiting Events (Naples) II and Atorvastatin for Reduction of Myocardial Damage During Angioplasty (ARMYDA)-RECAPTURE trials, a high dose statin loading is more effective in patients with a high C-reactive protein level at baseline.8),10) Therefore, a high dose statin loading therapy may be more efficacious in patients with ST-segment elevation myocardial infarction (STEMI) than in other clinical situations because STEMI is characterized by extremely high inflammation.
However, few data only are available to support the statin loading therapy before a primary PCI in patients with STEMI. The Efficacy of High-Dose AtorvaSTATIN Loading Before Primary PCI in ST-Elevation Myocardial Infarction (STATIN STEMI) trial demonstrated a 80 mg atorvastatin loading improved the coronary flow and perfusion after primary PCI.11) However, the number of STATIN STEMI participants was too small to draw a definite conclusion and further large trials are required to confirm the effect of statin loading in a primary PCI setting. Therefore, a retrospective study was designed to investigate the effects of high dose rosuvastatin loading before primary PCI on infarct size in patients with STEMI.
Subjects and Methods
Study population
For this study a single center STEMI and a primary PCI cohort were analyzed from January 2008 to December 2012. During the study period, 516 consecutive patients underwent primary PCI for STEMI. A total of 24 patients were excluded because of current treatment with statins, 8 patients were excluded because they died before they underwent the technetium 99m tetrafosmin single-photon emission computed tomography (SPECT) study, 8 patients were excluded because of SPECT refusal and 1 patient was excluded because of an inadequate image. Therefore 475 patients were eligible patients; of these, 208 patients received 40 mg rosuvastatin loading before primary PCI (statin group) and 267 patients didn't receive any statin pretreatment (control group). Rosuvastatin loading was performed in the emergency room at the on-call physician's discretion. All patients provided informed consent for processing their anonymous data according to a protocol approved by the Institutional Review Board of Wonkwang University Hospital (WKUHIRB-201310-HRE-021).
Percutaneous coronary intervention
Before the procedure aspirin (300 mg/day) and clopidogrel (300 mg/day) were loaded in all patients. An intravenous bolus of 5000 U of unfractionated heparin was given heparin boluses were given to maintain activated clotting time >300 seconds during the procedure additionally. The coronary angiography and the stent implantation were performed using standard interventional techniques. Platelet glycoprotein IIb/IIIa inhibitors were administered according to the operator's preference. After the procedure aspirin (100 mg/day), clopidogrel (75 mg/day) and statins were prescribed to all patients.
Data collection and analyses
Pre- and post-PCI angiograms were reviewed. The Thrombolysis in Myocardial Infarction (TIMI) flow grade before and after PCI, the corrected TIMI frame count (cTFC) and the myocardial blush grade (MBG) were analyzed by 2 experienced blinded observers as described previously.12),13) Creatine kinease myocardial band isoenzyme (CK-MB) isoenzyme and troponin T were measured before primary PCI and 8, 24 and 48 hours after. Peak concentrations were identified and the area under time-concentration curve was estimated from cardiac biomarker levels measured at individual time-points. Troponin T was measured quantitatively (Elecsys Troponin T assay, Roche Diagnostics, Indianapolis, IN, USA) with a detection threshold of 0.003 ng/mL.
To evaluate major adverse cardiac events (MACE) such as death, new myocardial infarction and target vessel revascularization a clinical follow-up was performed on day 30 with all patients.
Single-photon emission computed tomography and left ventricular function assessment
Single-photon emission computed tomography imaging with technetium 99m tetrofosmin was performed by a standardized technique. After injection of adenosine, 370 MBq of technetium 99m tetrofosmin was injected intravenously and stress myocardial images were obtained. After 4 hours, another 1110 MBq of technetium 99m tetrofosmin was administered intravenously and the resting myocardial images were obtained. The SPECT images were acquired on a dual-headed gamma camera (Vertex 60, Philips ADAC, Milpitas, CA, USA) equipped with high-resolution collimators. Myocardial perfusion defects (infarct size) were quantified and expressed as a percentage involvement of the left ventricle. The patients underwent SPECT imaging in a median of 3 days (interquartile range, 2-4 days) after PCI.
Study end points
The primary end point was the myocardial infarct size as assessed by SPECT. The secondary end points included 1) TIMI flow grade, cTFC, MBG after PCI, 2) infarct size assessed by serial cardiac biomarker measurement, and 3) 30-day MACE.
Statistical analysis
Based upon preliminary data of the Wonkwang Medical Center, the infarct size of the control group was expected to be 20% (standard deviation 15%). The sample size was selected to demonstrate a reduction in the infarct size from 20% in the control group to 15% in the statin group. A minimal sample size of 178 patients in each group would provide 80% power with two-sided alpha of 0.05.
All measurements were represented as mean±standard deviation or absolute number (percentage). Inter-group analysis was performed using independent t-test and χ2 test, which were conducted using Statistical Package for the Social Sciences (SPSS) 19.0 for Windows (SPSS Inc., Chicago, IL, USA). To compare the change of cardiac biomarkers before and after PCI, the paired t-test was used. A multivariable logistic regression model was constructed to predict large infarct size (greater than median value, >18%). According to the significant univariate analysis following variables were selected and inserted into the logistic regression analysis: rosuvastatin loading, pain to balloon time, anterior infarction, angiographic slow flow and final MBG. Statistical significance was set at p<0.05.
Results
Baseline characteristics
The baseline clinical characteristics of the patients in the control and statin groups are shown in Table 1. The risk factors, door-to-balloon time and the baseline cardiac biomarker levels were similar between the groups. Most of all patients received drug-eluting stents and over 70% of the patients received second generation drug-eluting stents (Table 2). Angiographic and procedural characteristics were similar between the groups, but in the control group a greater number of stents was used than in the statin group (1.4±0.7 vs. 1.3±0.5, p=0.028).
Table 1.
Baseline clinical characteristics
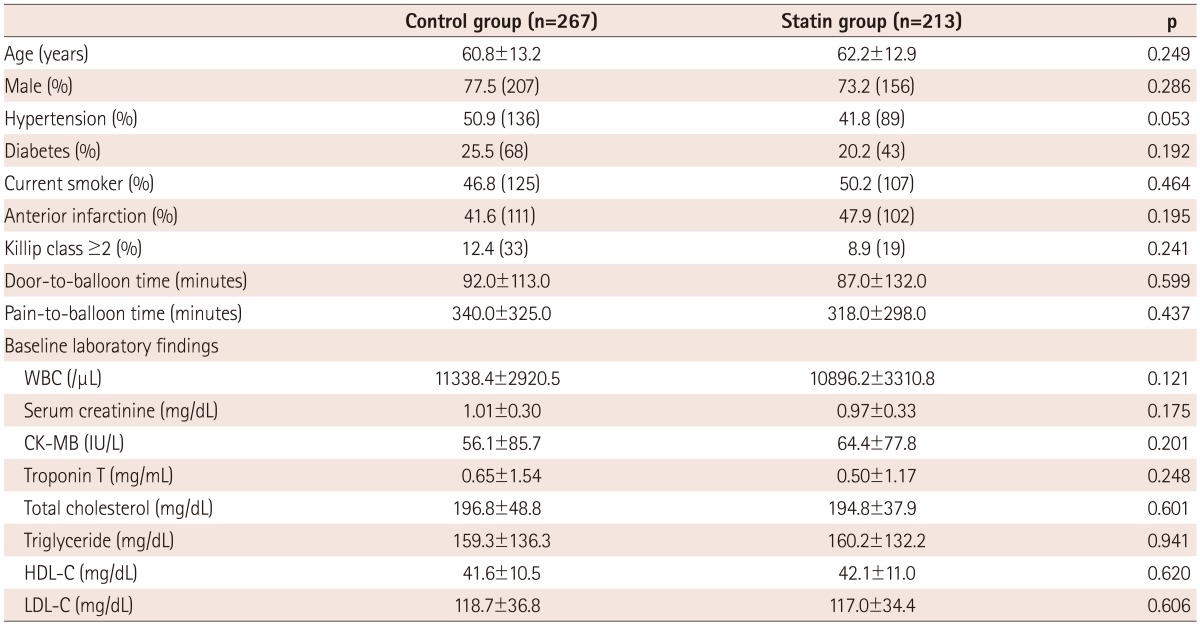
WBC: white blood cell, CK-MB: creatine kinease myocardial band isoenzyme, HDL-C: high density lipoprotein-cholesterol, LDL-C: low density lipoproteincholesterol
Table 2.
Coronary angiographic and procedural characteristics
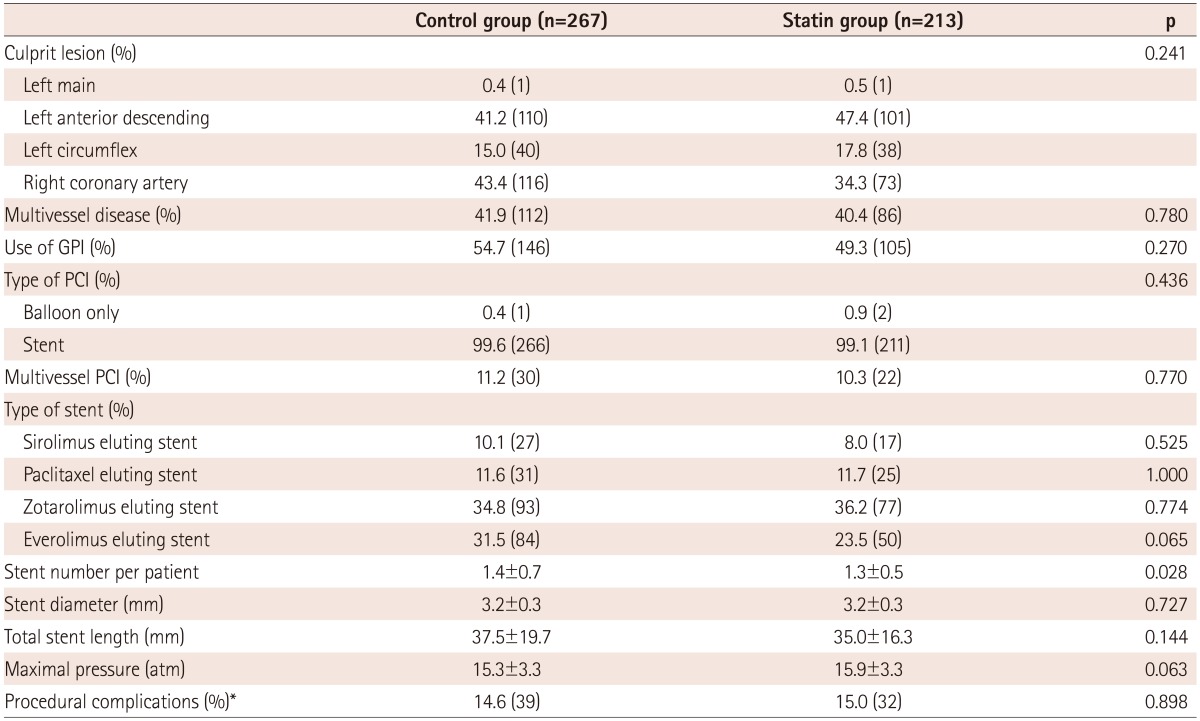
*Procedural complications included abrupt vessel closure, slow/no reflow, distal embolization, side branch occlusion, and major dissection during primary percutaneous coronary intervention. GPI: glycoprotein IIb/IIIa inhibitor, PCI: percutaneous coronary intervention
Angiographic and biochemical outcomes
Angiographic no reflow and final TIMI flow grade <3 occurred at a similar rate in both groups (Table 3). The final cTFC was lower (28.2±19.3 vs. 32.6±21.4, p=0.020) and the final MBG was higher in the statin group (2.49±0.76 vs. 2.23±0.96, p=0.001).
Table 3.
Radionuclide imaging, angiographic, and clinical outcomes
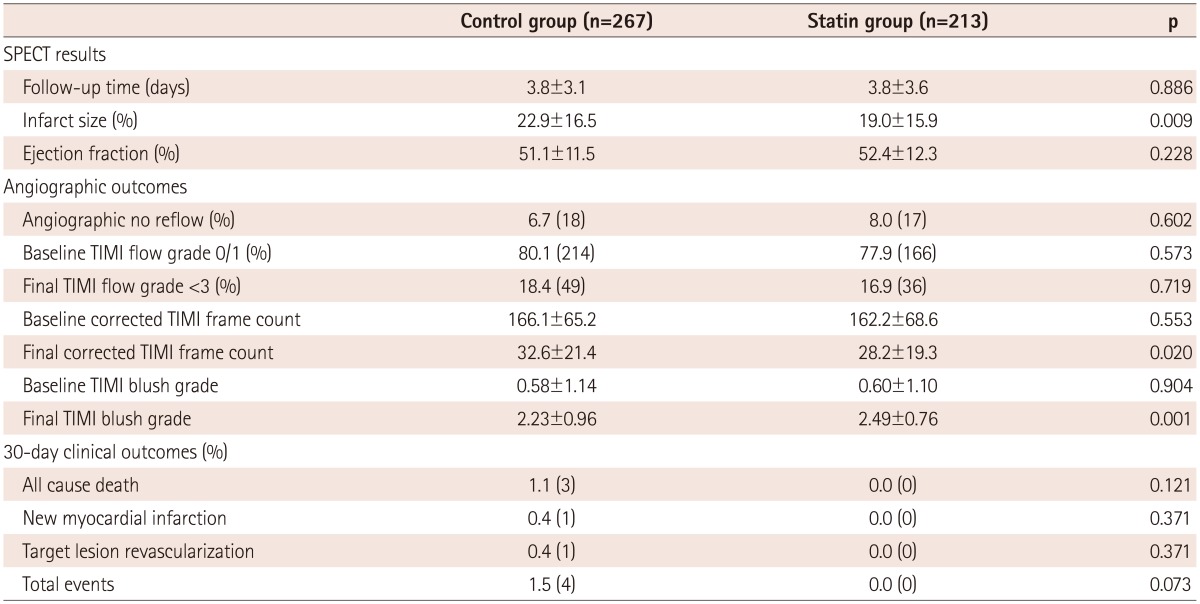
SPECT: single-photon emission computed tomography, TIMI: Thrombolysis in Myocardial Infarction
All single time-points after PCI (8, 24, and 48 hours) and peak level of CK-MB and troponin T were lower in the statin group (Fig. 1). The statin group showed significantly lower cumulative CK-MB levels (367.9±297.3 IU/L vs. 483.5±340.4 IU/L, p<0.001) and cumulative troponin T levels (13.03±11.29 ng/mL vs. 16.53±13.04 ng/mL, p=0.005) than the control group.
Fig. 1.

Time-concentration curve of creatine kinease myocardial band isoenzyme (CK-MB).
Infarct size measured by single-photon emission computed tomography
The median infarct size was 18.0% (interquartile range, 7.0-32.8%). There was no difference in the time from PCI to SPECT between the groups (Table 3). The statin group revealed a significant smaller infarct size than the control group (19.0±15.9% vs. 22.9±16.5%, p=0.009). However, the left ventricular ejection fraction was similar between both groups.
Multivariate analysis revealed that rosuvastatin loading {odds ratio (OR)=0.61; 95% confidence interval (CI)=0.41-0.91; p=0.015}, pain to balloon time >210 minutes (OR=2.05; 95% CI=1.38-3.05; p<0.001), anterior infarction (OR=3.89; 95% CI=2.56-5.91; p<0.001) and MBG <3 (OR=2.93; 95% CI=1.92-4.48; p<0.001) were independent predictors of the large (>18%) infarct size (Table 4).
Table 4.
Univariate and multivariate analysis for the prediction of >18% (median) infarct size
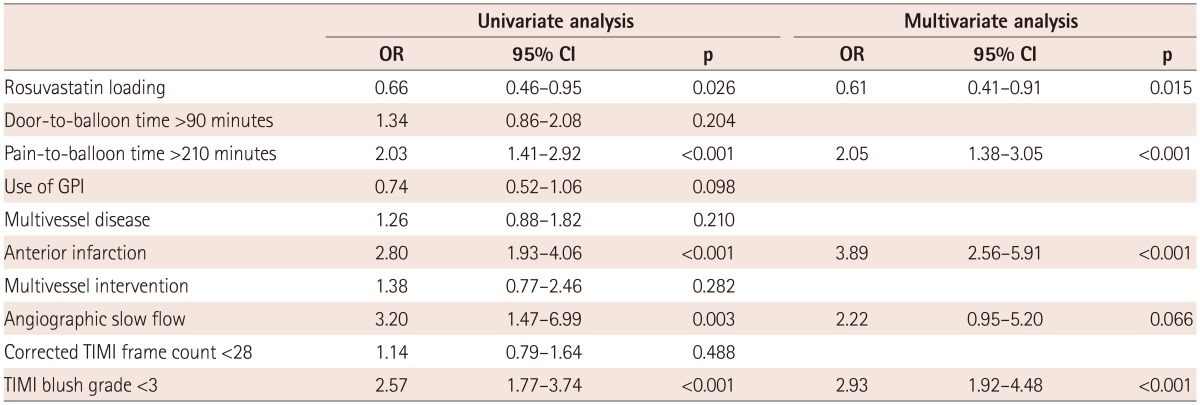
OR: odds ratio, CI: confidence interval, GPI: glycoprotein IIb/IIIa inhibitor, TIMI: Thrombolysis in Myocardial Infarction
30-day clinical outcomes
The incidences of MACE at day 30 were not significantly different between the groups (1.5% vs. 0%, p=0.073) (Table 3). No serious side effects were detected associated with rosuvastatin loading.
Discussion
In the present study it was shown the loading of 40 mg rosuvastatin before primary PCI is associated with a smaller infarct size which is measured by SPECT and lower levels of cardiac biomarkers. An improved coronary microcirculation was assessed by cTFC and MBG and may be attributable to the beneficial outcomes in the statin group.
High dose statin loading therapy before PCI can reduce the incidence of periprocedural MI and improve the outcomes in patients with ACS also. The ARMYDA-ACS trial was the first randomized study to assess the efficacy of high dose statin loading therapy before PCI in patients with ACS.6) As results of this trial an 80 mg atorvastatin loading 12 hours before PCI was indicated to reduce the postprocedural biomarker elevation and the 30-day MACE. Previously the authors performed a similar randomized study with 40 mg rosuvastatin. In this study the statin loading administered approximately 16 hours before PCI reduced the risk of periprocedural MI and 30-day MACE by 53% and 63%, respectively compared to the pretreatment without statin.7) However, the data of high dose statin loading in patients with STEMI were limited and not promising.
A chronic statin pretreatment before PCI reduced the length of hospital stay and the 30-day mortality and was an independent predictor of mortality in patients with MI in several non-randomized registries.14),15) However, prospective, randomized studies didn't show a benefit of statin loading therapy in patients with STEMI. The 30-day and 9-month MACE were not reduced in the STATIN STEMI trial if 80 mg atorvastatin where loaded before the primary PCI.11) Nevertheless, the efficacy of statin loading therapy should not be based on the results of this study only because the incidence of clinical events was lower than originally hypothesized and the sample size was insufficient. In this study rather was identified a significant lower cTFC and higher MBG. Thus, possibly via beneficial effects on microvascular function the statin loading therapy might improve coronary blood flow after PCI. A similar finding was also observed in the present study. Hahn et al.16) demonstrated that 80 mg atorvastatin loading before primary PCI didn't reduce the infarct size which was measured by SPECT or 6-month MACE. They also reported no improvement of MBG and cTFC after atorvastatin loading before the primary PCI compared with the control group. Liu et al.17) recently reported that 80 mg atorvastatin loading followed by 40 mg atorvastatin therapy could reduce the inflammatory response and improve the ejection fraction in patients with STEMI. The present observational study revealed a reduced infarct size, cardiac biomarker elevation and improved cTFC and MBG after 40 mg rosuvastatin loading, but the ejection fraction was not improved. This might be attributable to the heterogenity of the study population and the small sample size in each study group.
Both atorvastatin and rosuvastatin are potent synthetic statins and commonly prescribed in patients with coronary artery diseases. They also have pleiotropic effects which encompass the non-lipid mechanisms which are responsible for the modification of endothelial function, inflammatory responses, plaque stability and thrombus formation.18) Acute effects of statin loading on MI may contribute to the plaque stability. Lee et al.19) reported the presence of functionally active 3-hydroxy-3-methylglutaryl-coenzyme A reductase in coronary atherosclerotic plaque. Statins may penetrate atherosclerotic lesions and suppress active plaque inflammation by binding of lesion 3-hydroxy-3-methylglutaryl-coenzyme A reductase. It has been shown that rosuvastatin forms the largest number of bonds with 3-hydroxy-3-methylglutaryl-coenzyme A reductase which leads subsequently to a superior efficacy.20) However, this hypothesis requires further confirmation. Therefore a large prospective study is needed to confirm the effect of statin loading in patients with STEMI.
The presented study has several limitations. Presumably due to a biochemical stunning of the myocardium which limits an isotope uptake the infarct size is often overestimated in the early SPECT imaging between 18 and 48 hours.21) Therefore, the size of perfusion defect in this study did not reflect the true infarct size. However, the timing of SPECT imaging was similar in both groups (3.8±3.1 days vs. 3.8±3.6 days, p=0.886) and the assessment of statin loading effects were carried out under similar conditions. The study was not randomized and the sample size was small. The effects of statin loading on clinical outcomes could not be accurately determined, however, conclusions could be drawn on the benefits on surrogate markers. Furthermore, the outcomes according to the kind of statins or dose of statins and the exact duration of the therapy were not identified.
In conclusion, a high dose rosuvastatin loading before primary PCI was associated with a reduced infarct size by an improved microvascular myocardial perfusion.
Footnotes
The authors have no financial conflicts of interest.
References
- 1.Randomised trial of cholesterol lowering in 4444 patients with coronary heart disease: the Scandinavian Simvastatin Survival Study (4S) Lancet. 1994;344:1383–1389. [PubMed] [Google Scholar]
- 2.Shepherd J, Cobbe SM, Ford I, et al. Prevention of coronary heart disease with pravastatin in men with hypercholesterolemia. West of Scotland Coronary Prevention Study Group. N Engl J Med. 1995;333:1301–1307. doi: 10.1056/NEJM199511163332001. [DOI] [PubMed] [Google Scholar]
- 3.Sacks FM, Pfeffer MA, Moye LA, et al. The effect of pravastatin on coronary events after myocardial infarction in patients with average cholesterol levels. Cholesterol and Recurrent Events Trial investigators. N Engl J Med. 1996;335:1001–1009. doi: 10.1056/NEJM199610033351401. [DOI] [PubMed] [Google Scholar]
- 4.Hong YJ, Jeong MH, Lim JH, et al. The prognostic significance of statin therapy according to the level of C-reactive protein in acute myocardial infarction patients who underwent percutaneous coronary intervention. Korean Circ J. 2003;33:891–900. [Google Scholar]
- 5.Ridker PM, Danielson E, Fonseca FA, et al. Reduction in C-reactive protein and LDL cholesterol and cardiovascular event rates after initiation of rosuvastatin: a prospective study of the JUPITER trial. Lancet. 2009;373:1175–1182. doi: 10.1016/S0140-6736(09)60447-5. [DOI] [PubMed] [Google Scholar]
- 6.Patti G, Pasceri V, Colonna G, et al. Atorvastatin pretreatment improves outcomes in patients with acute coronary syndromes undergoing early percutaneous coronary intervention: results of the ARMYDA-ACS randomized trial. J Am Coll Cardiol. 2007;49:1272–1278. doi: 10.1016/j.jacc.2007.02.025. [DOI] [PubMed] [Google Scholar]
- 7.Yun KH, Jeong MH, Oh SK, et al. The beneficial effect of high loading dose of rosuvastatin before percutaneous coronary intervention in patients with acute coronary syndrome. Int J Cardiol. 2009;137:246–251. doi: 10.1016/j.ijcard.2008.06.055. [DOI] [PubMed] [Google Scholar]
- 8.Briguori C, Visconti G, Focaccio A, et al. Novel approaches for preventing or limiting events (Naples) II trial: impact of a single high loading dose of atorvastatin on periprocedural myocardial infarction. J Am Coll Cardiol. 2009;54:2157–2163. doi: 10.1016/j.jacc.2009.07.005. [DOI] [PubMed] [Google Scholar]
- 9.Yun KH, Oh SK, Rhee SJ, Yoo NJ, Kim NH, Jeong JW. 12-month follow-up results of high dose rosuvastatin loading before percutaneous coronary intervention in patients with acute coronary syndrome. Int J Cardiol. 2011;146:68–72. doi: 10.1016/j.ijcard.2010.04.052. [DOI] [PubMed] [Google Scholar]
- 10.Di Sciascio G, Patti G, Pasceri V, Gaspardone A, Colonna G, Montinaro A. Efficacy of atorvastatin reload in patients on chronic statin therapy undergoing percutaneous coronary intervention: results of the ARMYDA-RECAPTURE (Atorvastatin for Reduction of Myocardial Damage During Angioplasty) Randomized Trial. J Am Coll Cardiol. 2009;54:558–565. doi: 10.1016/j.jacc.2009.05.028. [DOI] [PubMed] [Google Scholar]
- 11.Kim JS, Kim J, Choi D, et al. Efficacy of high-dose atorvastatin loading before primary percutaneous coronary intervention in ST-segment elevation myocardial infarction: the STATIN STEMI trial. JACC Cardiovasc Interv. 2010;3:332–339. doi: 10.1016/j.jcin.2009.11.021. [DOI] [PubMed] [Google Scholar]
- 12.van 't Hof AW, Liem A, Suryapranata H, Hoorntje JC, de Boer MJ, Zijlstra F Zwolle Myocardial Infarction Study Group. Angiographic assessment of myocardial reperfusion in patients treated with primary angioplasty for acute myocardial infarction: myocardial blush grade. Circulation. 1998;97:2302–2306. doi: 10.1161/01.cir.97.23.2302. [DOI] [PubMed] [Google Scholar]
- 13.Gibson CM, Cannon CP, Daley WL, et al. TIMI frame count: a quantitative method of assessing coronary artery flow. Circulation. 1996;93:879–888. doi: 10.1161/01.cir.93.5.879. [DOI] [PubMed] [Google Scholar]
- 14.Lev EI, Kornowski R, Vaknin-Assa H, et al. Effect of previous treatment with statins on outcome of patients with ST-segment elevation myocardial infarction treated with primary percutaneous coronary intervention. Am J Cardiol. 2009;103:165–169. doi: 10.1016/j.amjcard.2008.08.052. [DOI] [PubMed] [Google Scholar]
- 15.Yun KH, Shin IS, Shin SN, et al. Effect of previous statin therapy in patients with acute coronary syndrome and percutaneous coronary intervention. Korean Circ J. 2011;41:458–463. doi: 10.4070/kcj.2011.41.8.458. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Hahn JY, Kim HJ, Choi YJ, et al. Effects of atorvastatin pretreatment on infarct size in patients with ST-segment elevation myocardial infarction undergoing primary percutaneous coronary intervention. Am Heart J. 2011;162:1026–1033. doi: 10.1016/j.ahj.2011.08.011. [DOI] [PubMed] [Google Scholar]
- 17.Liu HL, Yang Y, Yang SL, et al. Administration of a loading dose of atorvastatin before percutaneous coronary intervention prevents inflammation and reduces myocardial injury in STEMI patients: a randomized clinical study. Clin Ther. 2013;35:261–272. doi: 10.1016/j.clinthera.2013.01.009. [DOI] [PubMed] [Google Scholar]
- 18.Sposito AC, Chapman MJ. Statin therapy in acute coronary syndromes: mechanistic insight into clinical benefit. Arterioscler Thromb Vasc Biol. 2002;22:1524–1534. doi: 10.1161/01.atv.0000032033.39301.6a. [DOI] [PubMed] [Google Scholar]
- 19.Lee CW, Park CS, Hwang I, et al. Expression of HMG-CoA reductase in human coronary atherosclerotic plaques and relationship to plaque destabilisation. Heart. 2011;97:715–720. doi: 10.1136/hrt.2009.190934. [DOI] [PubMed] [Google Scholar]
- 20.McTaggart F. Comparative pharmacology of rosuvastatin. Atheroscler Suppl. 2003;4:9–14. doi: 10.1016/s1567-5688(03)00004-7. [DOI] [PubMed] [Google Scholar]