

Abstract
Purpose
To discriminate the visual symptoms and signs of Meares-Irlen syndrome (MIS) and nonspecific dyslexia from other ophthalmologic diseases (NODs).
Methods
Forty-five patients were enrolled. Thirty four of the patients with MIS whose symptoms improved with tinted lenses comprised MIS group. The other 11 patients whose reading difficulty improved with other ocular therapy and did not require tinted lenses comprised NODs group. The main symptoms causing dyslexia and associated ocular diseases were evaluated.
Results
The mean age was 17.9 ± 9.5 years in MIS group, and 19.3 ± 11.0 years in NODs group. In MIS group, the most common symptoms while reading were difficulty to move lines (85%), doubling (53%), and difficulty in bright condition (27%). On the other hand, blurring was the most common symptom in NODs group (45%). The associated ocular diseases in the two groups were refractive error (79% and 73%), dry eye (29% and 18%), and exophoria (6% and 27%), respectively.
Conclusions
Doubling, difficulty to move lines, and difficulty in bright condition while reading are main specific symptoms in MIS compared to nonspecific dyslexia from other ophthalmologic disorders.
Keywords: Diagnosis, Meares-Irlen syndrome, Tinted lenses
Dyslexia is a specific learning difficulty that affects reading and comprehension. Generally speaking, primary dyslexia (developmental dyslexia) refers to children who have difficulty mastering the relationships between the spelling patterns of words and their pronunciations. There is good evidence that dyslexia can be ameliorated by systematic phonic teaching combined with phonological awareness training. The high rates of association of seemingly disparate neuropsychiatric disorders (including attention deficit hyperactivity disorder [ADHD] and motor disorders) raises important challenges for understanding these disorders [1,2].
In contrast, Meares-Irlen syndrome (MIS, previously known as scotopic sensitivity syndrome) is a condition characterized by reading difficulties that are mitigated by wearing colored filters of a specific tint. Meares [3] and later Irlen and Lass [4] described a syndrome involving visual distortion that can be alleviated with colored filters. This syndrome has been referred to as "scotopic sensitivity syndrome" and the Irlen syndrome colored overlays and tinted lenses are purported to improve reading ability and visual perception, increase sustained reading time, and eliminate symptoms associated with reading, such as light sensitivity, eyestrain, headaches, blurring of print, loss of place, and watery eyes [5].
However, the symptoms of MIS should be differentially diagnosed from other ophthalmologic disorders such as refractive errors, exophoria and posterior subcapsular cataracts, which have similar non-specific visual symptoms to MIS [6].
We investigated the visual symptoms and signs in patients who had visited our department for reading difficulties to characterize the specific clinical features of MIS and the variable spectrum of dyslexia for ophthalmologists.
Materials and Methods
The medical records of 45 patients from December 2009 were retrospectively reviewed. Main symptoms causing reading difficulties and associated ophthalmologic disorders were evaluated. The study followed the tenets of the Declaration of Helsinki and was approved by the institutional review board at Korea University Medical Center. All patients were selected through a brief questionnaire including assessment for any symptoms of eyestrain or visual perceptual distortion and other symptoms to determine which symptoms caused reading difficulty. An ophthalmic examination that included an assessment of visual acuity, refractive errors, the slit lamp examination, the tear break-up time, strabismus and retinal findings was also performed. We excluded patients who were younger than nine years old and those who were linguistically, intellectually or mentally challenged.
Examination for dyslexia
We conducted a thorough examination for dyslexia using the reading writing speed meter, which was developed to evaluate reading/writing abilities in Korea [7]. Patients were asked to read aloud paragraphs differing in font size, spacing between letters and the level words depending on their age group (see below). The number of words read in 1.5 minutes was determined and recorded. Different paragraphs were provided for those in grades 1 to 3, 4 to 6, middle school, and high school. Additionally, the wording presented was random to eliminate the guessing of words based on context. The statistical analysis of the pace of reading before and after wearing tinted lenses was done using the SPSS ver. 13.0 (SPSS Inc., Chicago, IL, USA).
Choosing tinted lenses
MISVIS (Incheon, Korea) filters consist of diverse colors of lenses. Each color provides four to five lenses with differences in the degree of darkness (Fig. 1). All examinations were performed with the use of the patient's own spectacle correction. Patients first wore the lightest lens of each color group to ascertain the color group that he/she was most comfortable with. Within the selected color group, each patient then wore each lens and was instructed to choose the dark-tinted lens that was most satisfactory, subjectively and objectively. Subjects whose reading speed improved more than 20% while wearing the selected lenses and who were very satisfied with the lenses were considered to have MIS [5]. Patients whose reading speed did not improve at all while wearing the selected tinted lenses were categorized as dyslexic from nonspecific ocular disease and the nature of the associated nonspecific ophthalmologic diseases (NODs) were investigated.
Fig. 1.

MISVIS filter used in this study.
Results
Forty-five patients with dyslexia were included in this study. We divided these patients into two groups. The MIS group (average age, 17.9 ± 9.5 years; range, 8 to 34 years) comprised of 34 patients who were diagnosed with MIS. The remaining 11 patients (average age, 19.3 ± 11.0 years; range, 8 to 16 years) with dyslexia from NODs comprised the NODs group. Males predominated both the MISs (72%) and NODs group (60%). The most common symptoms observed in the MIS group were difficulty in moving lines (85%), doubling (53%), and difficulty in bright conditions (27%), followed by letter reversal (26%), blurring (18%), repetition (12%), headache (9%), and floating (3%) (Table 1). Blurring was the most common symptom in the NODs group (45%), followed by difficulty to move lines (36%) and repetition (18%) (Table 1).
Table 1.
Comparison of visual symptoms and signs between MIS and dyslexia from NODs
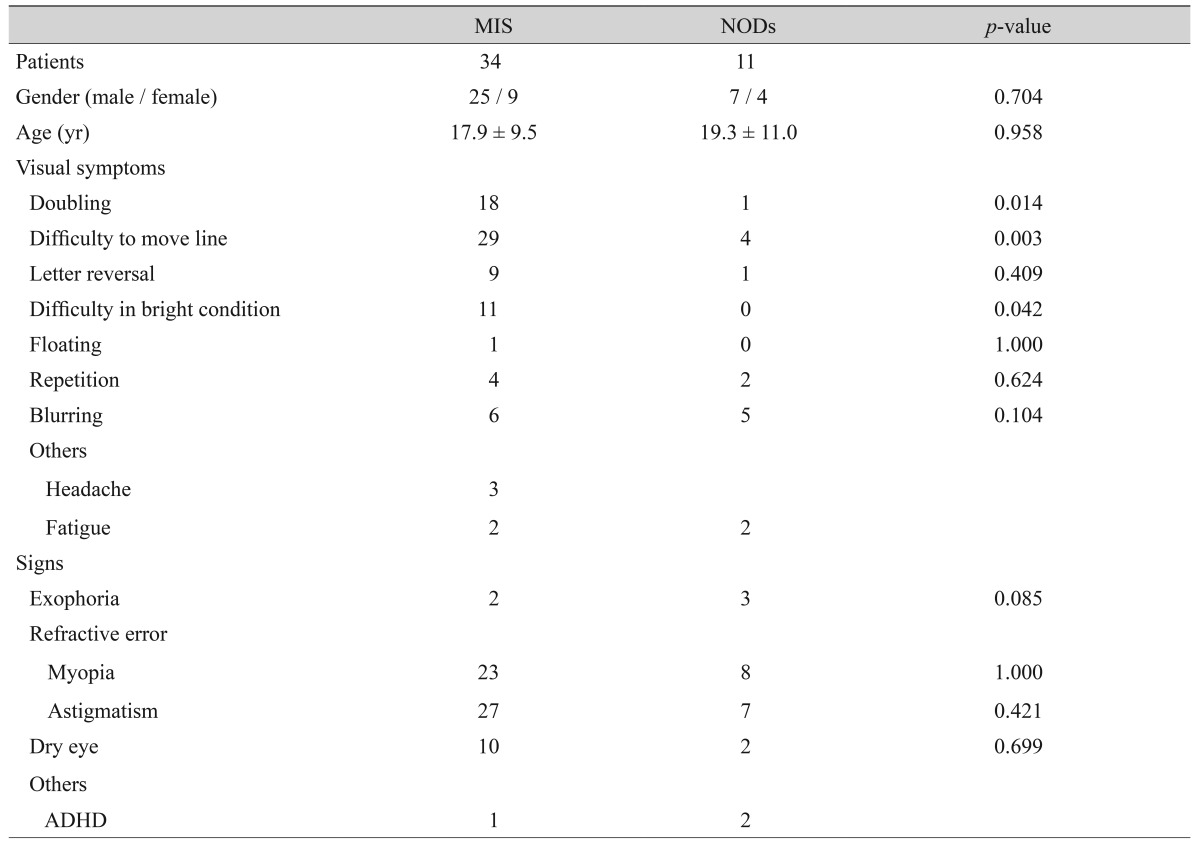
Values are presented as number or mean ± SD.
MIS = Meares-Irlen syndrome; NOD = nonspecific ophthalmologic disease; ADHD = attention deficit hyperactivity disorder.
Associated ocular diseases in the MIS and NODs group, were refractive error (79.4% and 72.7%, respectively), dry eye syndrome (29.4% and 18.1%, respectively), and exophoria (5.8% and 28.2%, respectively). In the MIS group, myopia and astigmatism were found in 23 patients, hyperopia and astigmatism were found in three patients and there was one patient with pure astigmatism. In the NODs group, refractive error was more common than exophoria and dry eye syndrome. ADHD was diagnosed in one patient in the MIS group and two patients in the NODs group (Table 1).
Discussion
MIS is considered to be a magnocellular system disorder that induces visual stress and distortion and the syndrome causes reading difficulties via hypertransmission of a specific light wave [8]. The use of color-filtered lenses are useful to improve visual symptoms. This lens-related improvement in vision is not a characteristic of other types of dyslexia [9].
In our study, doubling and difficulty in moving lines were specific visual distortion symptoms observed only in MIS patients. Other symptoms of MIS, such as fatigue, eyestrain and headache, were also present in patients with refractive error, exophoria and dry eye syndrome. These observations underscore the importance of conducting a complete ophthalmic examination and directing treatment at associated ocular problems before prescribing colored filters to patients with MIS. While repetition has been considered to be a specific symptom of MIS, presently this symptom was present in both groups without any significant difference.
Dyslexia can be classified into primary (developmental) dyslexia and MIS. Primary dyslexia is a disorder of phonological processing due to abnormalities of the left hemisphere parieto-occipital lobe, which occurs in learning disabilities but can be improved with appropriate phonological training [1,2]. Even though magnocellular dysfunction may have some role in the pathogenesis of primary dyslexia [10], our study was grounded in the suggestion that these two disorders are basically different and can be differentially diagnosed. Liberman et al. [11] demonstrated that the most important sign of primary dyslexia is letter reversal and this develops in children who first learn reading. In our study, however, letter reversal was also observed in nine patients with MIS whose symptoms subsided after using color-tinted lens. Helveston [9] reported that colored filters are ineffective for primary dyslexia, making it difficult to discriminate between these two disorders only with letter reversal. Moreover, primary dyslexia is common, accounting for 10% of the population in cultural areas using English or French in which one phoneme is pronounced two different ways [12]. Primary dyslexia might be rare in native Korean-speaking people, in which one phoneme is pronounced only a single way. Consistent with this speculation, no primary dyslexia was observed in our study.
Dyslexia may appear in neuropsychiatric disorders; in particular, an association between ADHD and dyslexia has been reported [13,14]. In our study, there were three patients with ADHD; one had MIS and the other two had NODs. The ADHD patient with MIS displayed improvement after psychiatric treatment and reading ability showed definite improvement after the use of color-tinted lenses. However, while psychiatric treatment before ophthalmic treatment was recommended for the other two patients, they did not visit the clinic again and so were included in the NODs group.
In our study, doubling, difficulty in moving lines and bright conditions were specific visual symptoms observed in MIS. However, NODs also includes refractive error, dry eye syndrome and exophoria, which also cause dyslexia. Therefore, to diagnose MIS, an ophthalmologist should pay attention to these eye problems and try to correct them.
This paper is limited by the retrospective nature of the data collection, the lack of standardization of symptom recording and the asymmetric sample size. An effective diagnosis/test for developmental dyslexia has been and remains the goal of 30 years of extensive research in this field and the general consensus is that dyslexia cannot be diagnosed with just one test. Even though this study was focused on MIS, the improvement criteria for wearing color-tinted lenses should be validated [7]. Further studies are clearly required to improve diagnostic tools for MIS such as evaluating the standardization of symptom recording and the efficacy of color-tinted lenses in patients with MIS by measuring not only improvement of symptoms but testing objective detection of the lesion as well.
In conclusion, doubling, difficulty in moving lines and bright conditions are specific visual symptoms observed in patients with MIS compared to nonspecific dyslexia from ophthalmologic disorders.
Footnotes
No potential conflict of interest relevant to this article was reported.
References
- 1.Stein J. The magnocellular theory of developmental dyslexia. Dyslexia. 2001;7:12–36. doi: 10.1002/dys.186. [DOI] [PubMed] [Google Scholar]
- 2.Nandakumar K, Leat SJ. Dyslexia: a review of two theories. Clin Exp Optom. 2008;91:333–340. doi: 10.1111/j.1444-0938.2008.00277.x. [DOI] [PubMed] [Google Scholar]
- 3.Meares O. Figure/ground, brightness contrast, and reading disabilities. Visible Lang. 1980;14:13–29. [Google Scholar]
- 4.Irlen H, Lass MJ. Improving reading problems due to symptoms of scotopic sensitivity syndrome using Irlen lenses and overlays. Education. 1989;109:413–417. [Google Scholar]
- 5.Williams GJ, Kitchener G, Press LJ, et al. The use of tinted lenses and colored overlays for the treatment of dyslexia and other related reading and learning disorders. Optometry. 2004;75:720–722. doi: 10.1016/s1529-1839(04)70226-2. [DOI] [PubMed] [Google Scholar]
- 6.Evans BJ. The need for optometric investigation in suspected Meares-Irlen syndrome or visual stress. Ophthalmic Physiol Opt. 2005;25:363–370. doi: 10.1111/j.1475-1313.2005.00289.x. [DOI] [PubMed] [Google Scholar]
- 7.Park SH, Kim SH, Cho YA, Joo CK. The effect of colored filters in patients with Meares-Irlen syndrome. J Korean Ophthalmol Soc. 2012;53:452–459. [Google Scholar]
- 8.Chase C, Ashourzadeh A, Kelly C, et al. Can the magnocellular pathway read? Evidence from studies of color. Vision Res. 2003;43:1211–1222. doi: 10.1016/s0042-6989(03)00085-3. [DOI] [PubMed] [Google Scholar]
- 9.Helveston EM. Scotopic sensitivity syndrome. Arch Ophthalmol. 1990;108:1232–1233. doi: 10.1001/archopht.1990.01070110048023. [DOI] [PubMed] [Google Scholar]
- 10.Livingstone MS, Rosen GD, Drislane FW, Galaburda AM. Physiological and anatomical evidence for a magnocellular defect in developmental dyslexia. Proc Natl Acad Sci U S A. 1991;88:7943–7947. doi: 10.1073/pnas.88.18.7943. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Liberman IY, Shankweiler D, Orlando C, et al. Letter confusions and reversals of sequence in the beginning reader: implications for Orton's theory of developmental dyslexia. Cortex. 1971;7:127–142. doi: 10.1016/s0010-9452(71)80009-6. [DOI] [PubMed] [Google Scholar]
- 12.Fluss J, Ziegler J, Ecalle J, et al. Prevalence of reading disabilities in early elementary school: impact of socioeconomic environment on reading development in 3 different educational zones. Arch Pediatr. 2008;15:1049–1057. doi: 10.1016/j.arcped.2008.02.012. [DOI] [PubMed] [Google Scholar]
- 13.Skottun BC, Skoyles J. Dyslexia: sensory deficits or inattention? Perception. 2007;36:1084–1088. doi: 10.1068/p5468. [DOI] [PubMed] [Google Scholar]
- 14.Skottun BC, Skoyles JR. Attention, reading and dyslexia. Clin Exp Optom. 2006;89:241–245. doi: 10.1111/j.1444-0938.2006.00052.x. [DOI] [PubMed] [Google Scholar]