

Abstract
This exploratory, descriptive study examined the views and opinions of parents of individuals with Down syndrome (DS) related to prenatal testing for DS and the use of age-based criteria to determine eligibility for this testing. This survey-based study was designed in collaboration with parents of individuals with DS and the British Columbia-based Lower Mainland Down Syndrome Society (LMDSS). The survey was a 26-item, self-report questionnaire, which was distributed by the LMDSS. Out of the 246 potentially eligible individuals that were mailed surveys, 101 participants returned their completed surveys. The availability of prenatal screening and diagnostic testing for DS was perceived positively by 55.1% and 64.7% of parents, respectively. More than half (60.2%) of participants felt that prenatal diagnostic testing for DS should be available to all pregnant women, regardless of age. In this study, views of Canadian parents of individuals with DS aligned with the prenatal testing policy recently adopted in the USA (whereby any woman, regardless of age or risk factors, can opt for prenatal diagnostic testing) rather than with new Canadian policy (whereby the age for automatic eligibility for diagnostic testing had increased from 35 to 40 years old and more recently is no longer offered on the basis of age-related risks, but on the basis of other risk factors).
Keywords: Down syndrome, prenatal testing, prenatal screening, parent’s attitudes, prenatal diagnosis, policy recommendations, guidelines
INTRODUCTION
It has been well established that a woman’s risk for having a child with Down syndrome (DS) increases with age. For women who are 35 years old at the time of delivery, the chance of having a child with DS is ~1 in 250, but for women who are 40 years old at the time of delivery, the chance is ~1 in 69 [Hook et al., 1983].
Diagnostic prenatal testing for DS has been available since the mid-1960s [Summers et al., 2007; Delisle and Wilson, 1999], while maternal serum screening was introduced in 1984 [ACOG Practice Bulletin, 2007]. The nature of available diagnostic tests (chorionic villus sampling or amniocentesis, which are associated with a risk of miscarriage that is often quoted as ~1/175–1/100) [Wilson et al., 2007] and screening tests, (non-invasive procedures like maternal serum screening/ultrasound), and the populations to whom they are offered, have evolved over time. Until recently, clinical practice guidelines for prenatal testing for DS were similar between the USA and Canada: prenatal screening was available to all pregnant women; diagnostic testing was available to those over the age of 35 and any women who received “positive” results1 on their screening tests [Driscoll and Gross, 2009]. However, in 2007, the practice guidelines of medical organizations in the USA and Canada diverged, such that in the USA diagnostic testing became available to all women, regardless of age and without the requirement of a positive screening test [ACOG Practice Bulletin, 2007, Driscoll and Gross, 2009]; while in Canada, for women without a positive screening test result, only those over the age of 40 were eligible [Summers et al., 2007]. Since 2007, the Canadian guidelines have been amended again: they now recommend that diagnostic testing no longer be offered to women on the basis of age [Chitayat et al., 2011]; rather, it should be available only when other risk factors are present (e.g. an increased risk on a prenatal screening test, ultrasound findings, or having a previous child with a chromosomal abnormality [Chitayat et al., 2011]).
The national Down syndrome societies in both Canada and the USA (the Canadian Down Syndrome Society (CDSS), The National Down Syndrome Congress (NDSC) and The National Down Syndrome Society (NDSS)) have their own recommendations for prenatal screening and testing. Broadly, these recommendations are similar between organizations: they emphasize the importance of informed consent, autonomy, and the right to continue a pregnancy where DS is diagnosed (CDSS, The NDSC, The NDSS). The NDSS states that all women should have access to prenatal testing (both screening and diagnostic tests), regardless of their age, while the other two organizations do not specifically make a recommendation on this issue (info@cdss.ca, The NDSC, The NDSS). The CDSS responded to the SOGC change in prenatal testing guidelines (2007) with the following statement: “…the SOGC and federal and provincial governments have a responsibility to ensure that all screens, tests, information and related counseling are readily available, funded and supported within provincial health systems and regional health authorities as part of a comprehensive prenatal strategy.” [http://www.cdss.ca/positioning/positioning/prenatal-genetic-screening-and-testing.html accessed Nov 2, 2011] The NDSS also issued a position statement in response to the ACOG change in prenatal testing guidelines (2007) emphasizing the importance of providing accurate and up-to-date information about DS to expectant parents as well as the importance of avoiding coercion in the prenatal testing process (whereby expectant parents might feel pressure to have prenatal testing or to terminate a pregnancy diagnosed with DS). To this end, the NDSS issued a “call-to-action”: “(we) challenge and strongly encourage health care professionals and organizations like ACOG to partner with NDSS and other Down syndrome organizations.” [http://www.ndss.org/index.php?option=com_content&view=article&id=153%3Aposition&limitstart=3, accessed Nov. 21, 2011] These sentiments are echoed in the position statements on prenatal screening and diagnosis from the NDSC and the CDSS.
Over the last decade, the approach towards decision-making relating to tests and treatments in medicine has been increasingly moving towards a more collaborative model, involving the physician and patient working together [Charles et al., 1999]. Concurrently, a growing body of research is emerging, aimed at assessing opinions of important stakeholder groups about what sorts of tests and treatments should be available to whom in the context of medicine. For example, related to prenatal testing, Kooij et al., explored the opinions of female medical students and pregnant women in the Netherlands, regarding to whom invasive diagnostic testing should be made available, and found that 45% of pregnant women and 11% of female medical students felt that diagnostic prenatal testing should be available to all women regardless of age [Kooij et al., 2009].
In another study of 78 female siblings of individuals with DS in the UK, 64% were in favor of the availability of prenatal diagnosis for DS and 54% would consider using this themselves [Bryant et al., 2005]. The majority (76%) was in favor of the availability of the option of termination of fetuses with DS but only 33% indicated they would personally consider this option [Bryant et al., 2005].
Although research documenting the opinions of these important stakeholder groups about prenatal testing has been emerging, the opinions of parents of individuals with DS – who have a unique and important perspective on these issues - have rarely been sought. A 1980’s study found that 86.6% of 97 mothers of children with DS felt amniocentesis should be available to all women [Elkins et al., 1986]. To the best of our knowledge, there have been no published studies relating to the opinions of parents of individuals with DS about prenatal testing since the 1980s, and given the increasing emphasis on collaborative decision making models and recent changes to the prenatal testing guidelines, we sought to redress this balance. Specifically, we sought to explore the perspectives of parents of individuals with DS with respect to:
Attitudes towards prenatal screening and diagnostic testing for DS
Whether and how maternal age should be used to guide eligibility criteria for prenatal diagnostic testing for DS
METHODS
Survey Instrument
In collaboration with the British Columbia based Lower Mainland Down Syndrome Society (LMDSS - the largest Canadian provincial non-profit organization that provides support, resources and information for individuals with DS and their families), we developed a self-report survey composed of 26 questions (both open and closed ended) designed to address the study objectives reported here, as well as others reported elsewhere (Hippman, et al., in press), and to obtain demographic information, including information about whether the participant had themselves undergone any kind of prenatal testing. We also included spaces in which participants were invited to provide narrative comments (see Appendix I).
In order to ensure a common understanding of the nature of the different types of prenatal tests before assessing participants’ opinions about them, we provided a definition of each (see Table I), followed by an introductory question aimed at eliciting participants’ attitudes towards prenatal testing broadly: “What do you think about prenatal screening and diagnostic testing for Down syndrome?” We then provided a list of four options related to screening tests, and a similar list of four options for diagnostic tests, all of which were developed in collaboration with the LMDSS (see Table I). We invited participants to select as many options from each list as they liked.
Table I.
Responses and response options to the questions “What do you think of prenatal screening?” and “What do you think about prenatal diagnostic tests?”
| Type of test | Response options provided | n (%) |
|---|---|---|
| Screening testsa | I think it is a good thing that prenatal screening is available. It helps people to find out about the chance that their pregnancy is affected with Down syndrome. | 51 (57) |
| I think it is a bad thing that prenatal screening is available. It makes people very anxious without telling them for sure whether or not the child will have Down syndrome. | 17 (19) | |
| I think it is a bad thing that prenatal screening is available. I feel its’ only purpose is to allow people to terminate pregnancies that are affected with Down syndrome. | 21 (23) | |
| I am not sure what I think about prenatal screening tests for Down syndrome. | 10 (11) | |
| Diagnostic testsb | I think it is a good thing that prenatal diagnostic tests are available. They help people to find out for sure whether or not their pregnancy is affected with Down syndrome, and allow them to make decisions about whether or not to continue with the pregnancy based on that information | 46 (51) |
| I think it is a good thing that prenatal diagnostic tests are available. They help people to find out for sure whether or not their pregnancy is affected with Down syndrome, and can allow people more time to prepare themselves to care for a child with Down syndrome. | 24 (28) | |
| I think it is a bad thing that prenatal diagnostic tests are available. I feel their only purpose is to enable people to terminate pregnancies that are affected with Down syndrome. | 20 (23) | |
| I am not sure what I think about prenatal diagnostic tests for Down syndrome. | 11 (13) |
Note: The percentages in this table do not equal 100% and the numbers in this table appear different to those presented in the text as a result of the fact that some individuals chose more than one option, holding both positive and negative attitudes towards testing depending on circumstance. With respect to prenatal screening, 2 participants felt this was both a good thing and a bad thing when the reason is to terminate. Similarly with respect to diagnostic testing, 5 participants felt that it was both a good thing if it helps parents prepare or make decisions, and a bad thing if used to terminate. Some participants also chose more than one option related to the same attitude, for example, eight participants felt that diagnostic testing is a good thing as it helps with making decisions and it helps with preparing. Similarly, 8 participants felt that prenatal screening tests were bad because they can induce anxiety and results could be used as a reason to terminate.
The following definition for prenatal screening tests was provided at the top of the page on which the participants’ opinions about them were sought: Prenatal screening tests: These do NOT provide definite yes or no answers about whether or not a baby has Down syndrome. Screening tests give an estimate of the chance that the baby is affected. For example, someone may get an estimated chance of 1/150 of having a child with Down syndrome. Examples of screening tests for Down syndrome that can be done during pregnancy include the triple marker screen (blood test), or a special kind of ultrasound.
The following definition for prenatal diagnostic tests was provided at the top of the page on which the participants’ opinions about them were sought: Prenatal Diagnostic Tests: These provide definite yes or no answers about whether a baby has Down syndrome. Examples of diagnostic tests for Down syndrome that can be done during pregnancy include amniocentesis and chorionic villus sampling (CVS).
In order to assess participants’ perspectives on whether and how maternal age should be used to guide eligibility criteria for prenatal diagnostic testing for DS, we asked: “To whom do you think prenatal diagnostic tests (like amniocentesis) for Down syndrome should be available?” All possible response options began: “I think that diagnostic tests for Down syndrome should….”, but there were four different endings from which respondents could choose:
be available to all pregnant women, regardless of their age.
be available only to pregnant women who are 40 years or older, or women who have had a screening test (e.g. a triple marker screen) that shows that there is a higher chance that the baby has Down syndrome.
be available only to pregnant women who are 35 years or older, or women who have had a screening test (e.g. a triple marker screen) that shows that there is a higher chance that the baby has Down syndrome.
not be available to any women during pregnancy.
The survey was piloted among the members of the LMDSS board (n=11), which is comprised of parents of individuals with DS, and changes to wording were made based on their feedback prior to distribution of the survey to potential participants (Fink, 1995).
Participants
To protect the personal information of the LMDSS members (including families with members with DS as well as other interested parties such as health care professionals), their contact information was not shared with the researchers. Instead, the LMDSS board distributed the anonymous surveys to their entire membership (N=260) by mail in November 2008 and January 2009. Due to database limitations, the LMDSS was unable to limit the mail-out to only parents of individuals with DS. After the initial survey mail-out, a reminder letter was sent approximately three weeks later. Each of the survey packages included a self-addressed, stamped envelope as well as the study material. Respondents were considered eligible if they were a parent or step-parent of an individual with DS. The study was approved by the Institutional Review Boards of the University of British Columbia and British Columbia Women’s Hospital (H08-01118).
Data Analysis
Descriptive statistics were used to explore the primary (quantitative) data, and verbatim quotes were chosen from the participants’ open-ended responses to illustrate key points. One-way ANOVAs were conducted to compare participants’ age, age of child with DS, and estimated age of participant at the time of giving birth to their child with DS with respect to the outcome variables of interest (opinion of prenatal screening, opinion of prenatal testing, and opinion of the age at which testing should be offered).
RESULTS
Response Rate
260 study packages were mailed out to the LMDSS membership. Four were returned to sender and ten ineligible participants were excluded. It is unknown how many of the remaining 246 potentially eligible LMDSS members were actually eligible, but 101 surveys were returned, thus response rate can be conservatively estimated at 41% (a typical response rate for surveys of this kind) [Kaplowitz et al, 2004]. No information was obtained on non-responders.
Demographics
The majority of respondents were females (87.1%) of European ancestry (79%), but the sample was diverse in terms of age (Range: 29–97; M=49) and religious affiliation (Table II). Information surrounding the timing of their child’s diagnosis, and whether or not participants had prenatal testing or screening during their pregnancy was also collected and is found in Table II.
Table II.
Summary of Demographic Information for Participants and their Children with DS
| Discrete variables: n (%) | |
|---|---|
| Continuous variables: Range (Mean) | |
| Participant Demographics | |
| Female | 88 (87.1) |
| Male | 13 (12.9) |
| European | 79 (79) |
| Asian | 6 (6) |
| Mixed | 8 (8) |
| Othera | 7 (7) |
| Religious | 55 (56.7) |
| Non-religious | 42 (43.2) |
| Demographics related to Pregnancy/Delivery of Child with DS | |
| Had prenatal screening | 18 (18.2) |
| Did not have prenatal screening | 78 (78.8) |
| Unsure whether had prenatal screening | 3 (3.0) |
| Had diagnostic testing | 7 (7.0) |
| Did not have diagnostic testing | 92 (92.0) |
| Unsure whether had diagnostic testing | 1 (1.0) |
| Maternal Age at Delivery b | 23–47 (33.7) |
| Demographics for Children with DS | |
| Female | 53 (52.0) |
| Male | 49 (48.0)c |
| Age | 5 months–54 years (15 years) |
| DS Diagnosis made Prenatally | 7 (7.1) |
| DS Diagnosis made at Birth | 78 (79.6) |
| DS Diagnosis made >1 day post deliveryd | 13 (13.3) |
We also included the response options “African” and “Aboriginal” but no respondents selected these options.
This represents the 85 biological mothers who responded to this survey.
This includes one set of twins.
This ranged from days to months after birth; one child was not diagnosed until 11 months.
Three children were adopted and were not included in these percentages.
Attitudes Regarding Prenatal Screening and Diagnostic Testing
Just over half of participants (n=49, 55.1% and n=57, 64.7 %) expressed only positive attitudes towards prenatal screening and diagnostic testing for DS respectively (see Table I). A total of 28 (31.5%) and 15 (17%) parents expressed only negative attitudes towards prenatal screening and diagnostic testing respectively. Those who were not sure how they felt about prenatal screening and diagnostic testing constituted 11.2% (n=10) and 12.5% (n=11) respectively. Some of the participants (n=2, 2.2% and n=5, 5.7%) chose more than one option, indicating both positive and negative attitudes (depending on circumstances relating to how the information would be used) towards prenatal screening and diagnostic testing respectively.
Many participants provided narrative comments in relation to these questions. One participant who expressed negative attitudes towards both prenatal screening and diagnostic testing commented: “I feel that many people don’t know enough about DS and living with DS when ending a pregnancy. I also believe that people don’t realize their own capacity for caring for a child with DS.” (Mother of a 13-year-old daughter with DS). Another participant who expressed positive attitudes towards both prenatal screening and diagnostic testing commented: “I love my daughter to pieces but find that parents should have a choice. Parenting a child with special needs is not for everyone (I wish it was:)).” (Mother of a 15-year-old daughter with DS).
Opinions on Maternal Age Use for Eligibility Criteria for Diagnostic Testing
More than half of the participants (n=53, 60.2%) indicated that prenatal diagnostic testing should be available to all women (see Figure 1). One participant who felt diagnostic testing for DS should be available for all women commented: “Because of our age, we are in a financial position to offer our son a lot, and we can afford the help we need. A lot of the parents I know are younger than 35 and struggling to manage the cost and cannot access the available help.” (Mother of an 8-year-old son with DS). Another two participants expressed different views for why testing should be available to all women. One said: “I believe all tests etc should be available to all women and the info results provided to them to make an informed decision. To deny one group of women access to a test on the basis of age seems to me a very paternalistic or patronizing action by the medical decision makers.” (Mother of a 5 ½ year old son with DS). The other reported: “I would probably (have) terminated our pregnancy (out of ignorance) had I known our baby had DS. I can not say for sure as I did not have to make that decision. But not knowing allowed our girl to be born and she is the foundation of our family’s love (along with her brother). To us she is not our DS child... She is our child with DS. I am thankful we did not test but it is not my place to take that option from others.” (Father of a 4 ½-year-old daughter with DS).
Figure 1.
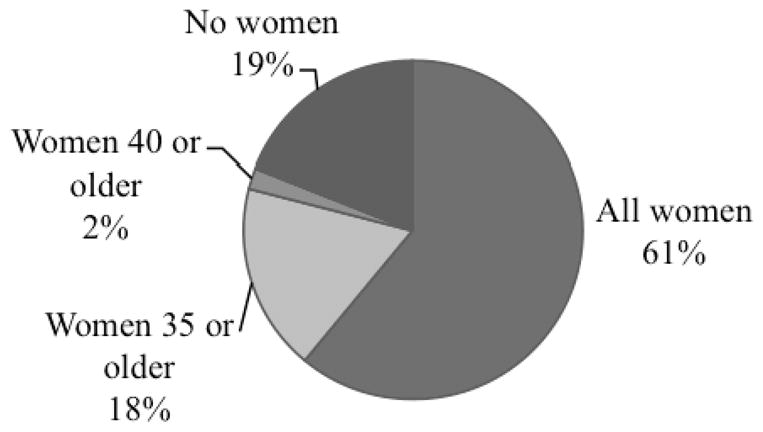
The opinions of parents of individuals with DS regarding to whom diagnostic prenatal genetic tests for DS should be available
One participant who felt diagnostic testing should be limited to women ≥35 years old commented: “Even amniocentesis has it’s risks and the outcome is not always positive. I know younger women are having babies with DS. But the age of 35 seems reasonable to me. If I was young and in my 20’s I wouldn’t think of having such a test. There is always the risk of a miscarriage.” (Mother of a 22-year-old daughter with DS). Another participant, who also felt diagnostic testing should be limited to those women ≥35 years old, commented: “While I advocate for choice, I worry that younger parents would be less able to handle the stresses associated with early false-positive or even with true positive indicators of DS.” (Father of a 4 ½-year-old daughter with DS).
Of the two participants who felt diagnostic testing should only be available to women ≥40 years old, only one chose to comment on her answer: “…… to have a DS child at 40 is, or can be, extra hard on a new mother. I don’t know if I could have handled all the years of sleepless nights. Especially for a single, older mother. Wow! Just the thought.” (Mother of a 17-year-old son with DS).
In contrast, one participant who was against diagnostic testing for all women commented: “If these tests were only used to be able to prepare the families for Down syndrome then I would not be opposed to them at all. Because these tests are there to give the option to abort the baby then I am very strongly opposed to them. It is barbaric to believe that just because a person is not as normal as someone else then we have the right to kill them. What kind of society are we? Can you actually look into my son’s eyes and tell me that he should have been aborted? It’s sick.” (Mother of a 3 ½-year-old son with DS).
Sub-analyses of Outcome Variables
The ANOVAs comparing age variables to opinions on prenatal screening and opinions on prenatal diagnostic testing were non-significant. The ANOVAs comparing age variables to opinion on age eligibility for prenatal diagnostic testing were non-significant.
Of those participants who underwent prenatal screening but did not report having diagnostic testing (n=13), seven expressed positive attitudes towards prenatal screening, three indicated negative attitudes and one was unsure. Of this group, ten expressed positive attitudes towards prenatal diagnosis and two expressed negative attitudes. Nine felt diagnostic testing should be available to all women, one thought it should be restricted to those women who are 35 and older and one participant felt it should not be available to any women.
There were two participants who underwent diagnostic testing but did not report having prenatal screening. Both expressed positive attitudes toward prenatal screening and while one did not respond to the question asking about their attitude towards prenatal diagnostic testing, the other expressed a positive attitude. One felt diagnostic testing should be limited to women 35 years and older, the other felt it should be available to all women.
Of those participants who underwent prenatal screening and diagnostic testing (n=5), four expressed only positive attitudes towards prenatal screening and one participant was not sure what they thought of screening. All five expressed only positive attitudes towards prenatal diagnostic testing and four participants felt it should be available to all women while one thought it should be limited to those women who are 35 years or older.
Of the thirteen fathers of individuals with DS who responded to this survey, seven expressed positive attitudes towards prenatal screening, three felt negatively towards it and one was unsure what he thought of it. Similarly, six fathers had positive attitudes towards prenatal diagnostic testing, two expressed negative attitudes, two expressed both positive and negative attitudes and one was unsure what he thought about it. Six fathers felt prenatal diagnostic testing should be available to all women, three indicated that it should be restricted to women over the age of 35 and two felt it should not be available to any women. The small sizes of these groups precluded any comparisons of responses between those who did and who did not undergo prenatal screening and/or diagnostic testing, or between fathers and mothers.
DISCUSSION
More than half of parents of individuals with DS expressed positive attitudes towards prenatal screening tests for DS and nearly two thirds expressed positive attitudes towards prenatal diagnostic testing for DS. Indeed, the attitudes of parents of individuals with DS towards prenatal testing closely resembles those of female siblings of individuals with DS – 64% of whom were in favor of the availability of prenatal diagnostic testing for DS [Bryant et al., 2005].
More than half of participants (60.2%) felt that prenatal diagnostic testing for DS should be available to all women regardless of age. As one participant said: “Tests are available - they cannot be denied if someone requests them. Maybe the focus should be on why people request them? Why send a child into a situation where they are not wanted?” (Mother of a 20-year-old son with DS). Another participant commented: “I don’t think it’s fair to deny anyone testing if they wish it. I think it is heartbreaking when people choose to abort a child because it has DS or something else, but I’m not walking in their shoes. Maybe they could not cope with it - would I rather a child be born to parents who can’t rise to the occasion? It is so hard to say.” (Mother of a 3-year-old son with DS). While the LMDSS (the organization from which we recruited study participants) does not have a position statement regarding access to prenatal testing, the US-based NDSS adopts the position that all women should have access to prenatal testing, regardless of age. As parents and caregivers of individuals with DS are key stakeholders represented by the NDSS, it would seem that there is some agreement between the sentiments of US-based and Canada-based parents of individuals with DS on this issue.
Interestingly, the proportion of parents of individuals with DS who were in favour of offering diagnostic testing to all women was greater than the two other groups of individuals who were recently studied. Kooij et al (2009) found that 45% of pregnant women and 11% of female medical students agreed that prenatal diagnostic testing should be available to all women. There are a number of potential reasons for the observed difference. With respect to the medical students in particular, these individuals were young (mean age of 21.6 years old) [Kooij et al, 2009], and were therefore likely to be approaching the question more from a medical professional perspective rather than a potential parent perspective (indeed, this was noted by the authors as a reason for selecting this group for study). Second, Kooij et al., (2009) noted the risks related to the amniocentesis and chorionic villus sampling procedures in their questionnaire. Many participants in the current study were aware of the risk associated with amniocentesis, and spontaneously made comments such as: “Even amniocentesis has it’s risks …..There is always the risk of a miscarriage.”. However, as we did not include a reference to the risk of miscarriage in the definition of diagnostic testing that was provided, this may have influenced some participants’ answers. Third, perhaps parents of individuals with DS are more likely to support the idea of diagnostic testing being available to all women as a result of their lived experience. Indeed, the only other study [Elkins et al, 1986] to have asked similar questions to parents of individuals with DS found that a large proportion (86.6%) were in favor of offering diagnostic testing to women of all ages. In the current study, few of the parents of individuals with DS had undergone prenatal testing of any kind themselves, and many of those who were in favor of offering diagnostic testing to all women made reference to having been under the age of 35 when their child with DS was born and that diagnostic testing was not offered to them; for example one participant who felt diagnostic testing should be available to all women stated: “I was 29 years old when I had my child with Down syndrome. There were no indicators in my pregnancy no family history hence no-one felt the need to check for it. Had I been screened, maybe my life would be different today.” (Mother of a 15-year-old son with DS). Others mentioned that they had many friends who were under the age of 35 when they had their child with DS; “I have met many young moms who had their child with Down syndrome in their 20’s. It’s a personal choice. Knowing would help prepare you better.” (Mother of a 15-year-old daughter with DS).
Not only did most participants feel that prenatal diagnostic testing should be available to all women, only two participants felt that this kind of testing should only be available to those ≥40 years old. Overall, the views of the Canadian parents of individuals with DS who participated in this study align more closely with the policy recently adopted in the US (whereby any woman, regardless of age, can opt for prenatal diagnostic testing) than they do with Canadian policy (whereby age-related eligibility for diagnostic testing had increased from 35 to 40 years old at the time of the study). While Canadian guidelines have more recently removed age as an eligibility criterion for prenatal diagnostic testing, the guidelines do not allow women of any age to choose prenatal diagnostic testing. Instead, women without any prior risk factors are required to go through the process of prenatal screening before having the option of diagnostic testing, and will not have the option of diagnostic testing if their risk of DS is not deemed by the medical community to be high enough to merit the test. These guidelines are contrary to the position statement of the NDSS and the views expressed by Canadian participants in this study.
It is important to consider that healthcare policy decision makers and consumers of medical tests may approach the same issue from very different perspectives and, perhaps too, with different values. Healthcare policy decisions tend to depend heavily on cost-benefit analyses, which are often of a more fiscal nature. These decisions seldom take into consideration other, less tangible or measurable costs, e.g. anxiety that persists in the face of a “negative” screening test result. The move to make greater use of non-invasive screening tests in Canada was based – at least in part – on the motivation to reduce the number of pregnancies lost as a result of invasive prenatal diagnostic procedures (Chitayat et al., 2011). The value implicit in this goal is that the worst possible outcome would be to lose a pregnancy with a normal karyotype as a result of an invasive procedure, and that policy measures need to be implemented to reduce the risk of this outcome. But, this study indicates that some parents of individuals with DS may not share the perspective of policy makers regarding the ultimate worst outcome in this situation. Additionally, their cost-benefit analysis may look very different than that of the policy makers.
In Western culture, a high value is placed on individual autonomy in decision-making, and women are already required to provide informed consent before undergoing a prenatal diagnostic testing procedure. This, taken together with the data from this study, suggests that the approach recently adopted in the US of allowing all women regardless of age to make an autonomous, informed decision for themselves about whether to undergo invasive diagnostic testing, non-invasive screening testing (perhaps followed by invasive testing), or no testing at all, is an approach that may be preferable to consumers in Canada. Although there are obvious health service differences between the US and Canada, it will nevertheless be interesting to see how the US experience of implementing this policy unfolds over time, particularly with respect to uptake frequency of different testing options which may allow estimations to be made regarding the implications of adopting a similar policy in Canada.
Strengths and Limitations
A significant strength of this study is that the questionnaire was anonymous, which allowed participants to share their perspectives candidly, without fear of repercussions. One participant discussed that it is “taboo” within the DS community to say anything negative about your child with DS. Another wrote “I had amnio done with my 3rd child and would have terminated the pregnancy if the baby had Down syndrome.” (Mother with a 28-year-old son with DS). This participant may not have been comfortable with this disclosure if the questionnaire was not anonymous.
Only a small proportion of our respondents reported having had prenatal testing for DS. Some of our participants were older and likely to have been pregnant with their child with DS before the introduction of routine prenatal testing. Additionally, data show that of those individuals who receive prenatal diagnoses of DS, most terminate their pregnancies [Mansfield et al, 1999; Shaffer et al, 2006]. Thus, it may be reasonable to anticipate that a relatively small proportion of parents of live-born children with DS would have had prenatal testing. However, we cannot exclude the possibility of response bias whereby individuals who had not had prenatal testing were more likely to respond to a survey of attitudes towards prenatal testing.
Only a small number of fathers of individuals with DS (n=13) responded to this survey, which limited our ability to make statistical comparisons between the opinions of mothers and fathers. However, to our knowledge, this is the first report in which any data about the attitudes of fathers towards prenatal testing for DS have been reported. The thoughts and opinions of fathers of individuals with DS is an area that warrants further research.
It is important to note that this was not a population-based study. There may be systematic differences between individuals who are members of support organizations and those who are not. Thus, the results from this study cannot be generalized to all parents of individuals with DS. Attempting to access the views and opinions of parents of individuals with DS who are not members of support organizations could be a fruitful area for future work.
Although the geographic region in which the survey was conducted (Vancouver, BC) has a large Asian population, very few respondents were of Asian ancestry. This may be due to a language barrier, as the questionnaire was only made available in English. It would be valuable to conduct future research with a trans-cultural focus.
Last, this was a cross-sectional study. We did not attempt to address whether and how participants’ views varied over time. This too could be an area worthy of future work.
Conclusions
This study provides insight into the opinions of parents of individuals with DS with regards to prenatal testing for DS. This population has a lived experience that offers a unique perspective that is hugely pertinent to discussions around prenatal diagnostic testing for DS, including which individuals have access to this testing. As we move towards collaborative decision-making models in medicine and increasingly seek the expertise of more diverse groups of stakeholders, including the perspectives of groups such as this will be important as we develop future testing guidelines.
Supplementary Material
Acknowledgments
The National Society of Genetic Counselors (NSGC) Prenatal Special Interest Group and The Rare Disease Foundation provided funding that made this research possible. A. I. was a student of the University of British Columbia (UBC) MSc in Genetic Counselling program when this research was conducted. JA was supported by the Canadian Institutes of Health Research, the Michael Smith Foundation for Health Research, and the BC Provincial Health Services Authority. Special thanks to the board members of the Lower Mainland Down Syndrome Society, Theresa Preston, Rachelle Blais and the parents who took the time to participate in this study.
Footnotes
In this case, “positive” results refer to results indicating a risk for DS that is greater than or equal to the age related risk for DS for a 35-year-old woman, often defined as 1 in 270.
References
- ACOG Practice Bulletin. Screening for fetal chromosomal abnormalities. Obstet Gynecol. 2007;109:217–227. doi: 10.1097/00006250-200701000-00054. [DOI] [PubMed] [Google Scholar]
- Bryant L, Hewison JD, Green JM. Attitudes towards prenatal diagnosis and termination in women who have a sibling with Down’s syndrome. J Reprod Infant Psychol. 2005;23:181–198. [Google Scholar]
- Charles C, Gafni A, Whelan T. Decision-making in the physician-patient encounter: revisiting the shared treatment decision-making model. Soc Sci Med. 1999;49:651–661. doi: 10.1016/s0277-9536(99)00145-8. [DOI] [PubMed] [Google Scholar]
- Chitayat D, Langlois S, Wilson RD. Prenatal Screening for fetal aneuploidy in singleton pregnancies. J Obstet Gynaecol Can. 2011;33:736–50. doi: 10.1016/S1701-2163(16)34961-1. [DOI] [PubMed] [Google Scholar]
- Delisle MF, Wilson DR. First trimester prenatal diagnosis: amniocentesis. Semin Perinatol. 1999;23:414–423. doi: 10.1016/s0146-0005(99)80007-x. [DOI] [PubMed] [Google Scholar]
- Driscoll DA, Gross SJ Professional Practice Guidelines committee. Screening for fetal aneuploidy and neural tube defects. Genet Med. 2009;11:818–21. doi: 10.1097/GIM.0b013e3181bb267b. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Elkins TE, Stovall TG, Wilroy S, Dacus JV. Attitudes of mothers of children with Down syndrome concerning amniocentesis, abortion, and prenatal genetic counseling techniques. Obstet Gynecol. 1986;68:181–184. [PubMed] [Google Scholar]
- Fink A, editor. The Survey Handbook. Vol. 1. Thousand Oaks, CA: Sage; 1995. [Google Scholar]
- Hook EB, Cross PK, Schreinemachers DM. Chromosomal abnormality rates at amniocentesis and in live-born infants. JAMA. 1983;249:2034–2038. [PubMed] [Google Scholar]
- info@cdss.ca [accessed Nov 2, 2011];Prenatal Genetic Screening and Testing. 2009 Jul; http://www.cdss.ca/positioning/positioning/prenatal-genetic-screening-and-testing.html.
- Kaplowitz MD, Hadlock TD, Levine R. A comparison of web and mail survey response rates. Public Opin Q. 2004;68:94–101. [Google Scholar]
- Kooij L, Tymstra T, van den Berg P. The attitudes of women toward current and future possibilities of diagnostic testing in maternal blood using fetal DNA. Prenat Diagn. 2009;29:164–168. doi: 10.1002/pd.2205. [DOI] [PubMed] [Google Scholar]
- Mansfield C, Hopfer S, Marteau TM. Termination rates after prenatal diagnosis of Down syndrome, spina bifida, anencephaly, and Turner and Klinefelter syndromes: a systematic literature review. European Concerted Action: DADA (Decision-making After the Diagnosis of a fetal Abnormality) Prenat Diagn. 1999;19:808–812. [PubMed] [Google Scholar]
- National Down Syndrome Congress. [accessed Nov 2, 2011];Position Statement on Prenatal Screening and Diagnosis. http://www.ndsccenter.org/resources/position1.php.
- National Down Syndrome Society. [accessed Mar 12, 2014];Position papers - Prenatal testing. 2011 http://ndsccenter.org/worpsite/wp-content/uploads/2012/02/Prenatal_Screening_Diagnosis.pdf.
- National Down Syndrome Society. [accessed Mar 12, 2014];National Down Syndrome Society Responds to American College of Obstetricians and Gynecologists’ New Recommendations for Prenatal Testing. 2007 http://ndsccenter.org/worpsite/wp-content/uploads/2012/02/Prenatal_Screening_Diagnosis.pdf.
- Summers AM, Langlois S, Wyatt P, Wilson RD Society of Obstetricians and Gynaecologists of Canada. Prenatal screening for fetal aneuploidy. J Obstet Gynaecol Can. 2007;29:146–179. doi: 10.1016/S1701-2163(16)32379-9. [DOI] [PubMed] [Google Scholar]
- Shaffer BL, Caughey AB, Norton ME. Variation in the decision to terminate pregnancy in the setting of fetal aneuploidy. Prenat Diagn. 2006;26:667–671. doi: 10.1002/pd.1462. [DOI] [PubMed] [Google Scholar]
- Wilson D, Langlois S, Johnson J Society of Obstetricians and Gynaecologists of Canada. Mid-trimester amniocentesis fetal loss rate. J Obstet Gynaecol Can. 2007;29:586–595. doi: 10.1016/S1701-2163(16)32501-4. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.