

Abstract
Background:
Healthcare-associated infections (HAIs) have been reported to be a serious problem in the healthcare services as they are common causes of illness and mortality among hospitalized patients including healthcare workers (HCWs). Compliance with these standard precautions has been shown to reduce the risk of exposure to blood and body fluids.
Aims:
This study therefore assesses the level of knowledge and compliance with standard precautions by the various cadre of HCWs and the factors influencing compliance in hospital environment in Nasarawa State, Northern Nigeria.
Settings and Design:
Nasarawa State has a current human immunodeficiency virus/acquired immunodeficiency syndrome (HIV/AIDS) prevalence rate of 10.0%, which was higher than most states in Nigeria with a high level of illiteracy and ignorance. Majority of the people reside in the rural areas while a few are found in the towns, informal settlements with no direct access to healthcare facilities are common.
Materials and Methods:
This study is an analytical, cross-sectional study. Proportional sampling technique was used to obtain a representative sample and a structured self-administered questionnaire was used to collect relevant information from the healthcare providers working in Nasarawa State from January to February 2009.
Statistical analysis used:
To describe patient characteristics, we calculated proportions and medians. For categorical variables, we compared proportions using chi-square tests. A logistic regression model was produced with infection control as outcome variable to identify associated factors.
Results:
A total of 421 HCWs were interviewed, Majority (77.9%) correctly describe universal precaution and infection control with 19.2, 19.2, and 28.0%, respectively unable to recognize vaccination, postexposure prophylaxis, and surveillance for emerging diseases as standard precaution for infection control. About 70.1% usually wear gloves before handling patients or patients’ care products, 12.6% reported wash their hand before wearing the gloves, 10.7% washed hands after removal of gloves, and 72.4% changed gloves after each patient. Only 3.3% had a sharp disposal system in their various workplaces. Majority (98.6%) of the respondents reported that the major reason for noncompliance to universal precautions is the nonavailability of the equipments. There was a statistically significant difference in the practice of standard precaution among those that were exposed to blood products and body fluid compared to those that had not been exposed in the last 6 months (χ2 = 3.96, P = 0.03), public healthcare providers when compared to private health workers (χ2 = 22.32, P = 0.001), among those working in secondary and tertiary facilities compared to primary healthcare centers (χ2 = 14.64, P = 0.001) and urban areas when compared to rural areas (χ2 = 4.06, P = 0.02). The only predictor of practice of standard precaution was exposure to blood and body fluid in the last 6 months odds ratio (OR) = 4.56 (confidence interval (CI) = 1.00-21.28).
Conclusions:
This study implies that inadequate workers’ knowledge and environment related problems, including the lack of protective materials and other equipments and utilities required to ensure safety of HCWs is a crucial issue that need urgent attention. Institution of a surveillance system for hospital acquired infection to improve consistent use of standard precautions among health workers is recommended in Nigeria and other low income countries in Africa.
Keywords: Health workers, Infection control, Northern Nigeria, Standard precaution practice
INTRODUCTION
Healthcare workers (HCWs) are at direct risk of exposure to blood and other body fluids during the course of their job. Consequently, they are at risk of infection of-blood borne viruses including hepatitis B virus (HBV), hepatitis C virus (HCV), and human immunodeficiency virus (HIV).[1] Occupational exposure to blood can result from percutaneous (needle stick or other sharps injury) and mucocutaneous injury (splash of blood or other body fluids into the eyes, nose, or mouth), or blood contact with non-intact skin.[2] Needle stick injury (NSI) is the most common form of occupational exposure to blood which results in transmission of blood borne infection. Healthcare-associated infections (HAIs) have been reported to be a serious problem in the healthcare services as they are common causes of illness and mortality among hospitalized patients including HCWs.[3,4,5,6,7]
Compliance with these standard precautions has been shown to reduce the risk of exposure to blood and body fluids.[8] The term “standard precautions” is replacing “universal precautions”, as it expands the coverage of universal precautions by recognizing that any body fluid may contain contagious and harmful microorganisms.[9] The level of practice of universal precautions by HCWs may differ from one type of HCW to another. The differences in knowledge of universal precautions by HCWs may be influenced by their varying type of training.[8] The absence of enabling environment in the health institution, such as a lack of constant running water or a shortage of personal protective equipment (PPE), would lead to poor compliance with universal precautions. It therefore, becomes importance to assess the level of compliance with universal precautions by the various types of HCWs (doctors, trained nurses, pharmacist, laboratory, scientist, other health workers, and domestic staff) who make direct contact with patients, and level of compliance by HCWs in the various types of health facilities.
In 1987 the Centers for Disease Control and Prevention (CDC) developed standard precautions to help protect both HCWs and patients from infection with blood-borne pathogens in the healthcare setting.[10] These recommendations stress that blood is the most important source of HIV, HBV, and other blood-borne pathogens and that infection control efforts should focus on the prevention of exposures to blood as well as the receipt of HBV immunizations. In 1995, the CDC’s Hospital Infection Control Practices Advisory Committee (HICPAC) introduced the concept of standard precautions, which synthesizes the major features of universal precautions and body substance isolation into a single set of precautions to be used for the care of all patients in hospitals regardless of their presumed infection status.[11] Blood, certain other body fluids (e.g., semen; vaginal secretions; and amniotic, cerebrospinal, pericardial, peritoneal, and synovial fluids), and tissues of all patients should be considered potentially infectious.[10,12] Standard precautions apply to blood; all body fluids, secretions, and excretions (except sweat); non-intact skin; and mucous membranes.[11] The core elements of standard precautions comprise (i) hand washing after patient contact, (ii) the use of barrier precautions (e.g., gloves, gowns, and facial protection) to prevent mucocutaneous contact, and (iii) minimal manual manipulation of sharp instruments and devices and disposal of these items in puncture-resistant containers.[10,11,12]
The significance of infection control in healthcare settings cannot be overemphasized as both the patients and HCWs are capable of spreading microorganism if adequate infection control measures are not strictly adhered to. In addition, healthcare is increasingly being provided outside hospitals in facilities such as nursing homes, free standing surgical and outpatient centers, emergency care clinics, and in patients’ homes or during prehospital emergency care. The importance of airborne transmission of microorganisms in the hospital setting and the risk of cross infection between patients and HCWs especially in respect of blood-borne pathogens are widely documented.[13] Hospital-based personnel and personnel who provide healthcare outside hospital may acquire infections from or transmit infections to patients, other personnel, household members, or other community contacts.[14] This study therefore assesses the level of compliance with standard precautions by the various cadre of HCWs and the factors influencing compliance in hospital environment in Northern Nigeria. This will aid in adapting infection control measures to protect patients, staff, and the general public.
MATERIALS AND METHODS
Study design
This study is an analytical, cross-sectional study. The information was collected from the healthcare providers working in Nasarawa State from January to February 2009.
Study area
Nasarawa Sate was created on 1st October, 1996 from the present Plateau State by the regime of late General Sanni Abacha, and has Lafia as its capital city. It covers a land area of approximately 27,116.8 km2 . It comprises of 13 local government areas namely; Akwanga, Awe, Doma, Karu, Keana, Keffi, Kokona, Lafia, Nasarawa, Eggon, Obi, Toto, and Wamba.
The state has the following boundaries: In the northwest by the federal capital territory (FCT), Abuja, northeast by Plateau State, north by Kaduna State, south by Benue State, southwest by Kogi sate, and southeast by Taraba State. Nasarawa State lies within the guinea savannah region and has tropical climate. Rainfall is moderate with a mean annual rainfall of about 1,311.75 cm. It is made up of plain lands and hills measuring up to 300 feet above the sea level at some points. According to 2006 census by the National Population Commission (NPC) Nasarawa State has a total population of 1,863,275.
Nasarawa State is a multiethnic state. The major ethnic groups found in the state are; Eggon, Mada, Gwandara, Bassa, Alago, Rindre, Nyamkpa, Migilli, Koro, Kantana, Arum, Afo, Tiv, Hausa, Fulani, and Kanuri. Three major religious groups are predominant in the state namely; Christianity, Islam, and traditional worshipers. Nasarawa State is predominantly a rural and agrarian state. Majority of the people reside in the rural areas while a few are found in the towns of Lafia, Keffi, Akwanga, Nasarawa, and Karu. Therefore, informal settlements with no direct access to healthcare facilities are common.
There is high level of illiteracy and ignorance in the state. The state has two tertiary health institutions which are Specialist Hospital Lafia and Federal Medical Centre Keffi. There are 13 general hospitals and comprehensive healthcare centers cited in each local government area and several private clinics and public health centers scattered all over the state. Nasarawa State has a current HIV/acquired immunodeficiency syndrome (AIDS) prevalence rate of 10.0% (NASACA, 2008), which was higher than most states in Nigeria. Similarly, Lafia the state capital with HIV/AIDS prevalence of 19.0% (NASACA, 2008) was ranked fifth after Otukpo, Calabar, Kafanchan, and Abakaliki in terms of HIV/AIDS prevalence. Hence, the impact of this condition on the HCWs in the state cannot be overemphasized.
Study population
There were 1,680 HCWs as on December 2007. This comprised of 1,357 in public/government Health Institutions and 323 registered health workers in private hospitals/clinics throughout the state (MOH, Nasarawa State). This is as shown in Table 1 below.
Table 1.
Universal precaution and socio-dermographic characteristics
Sample size determination
The total number of registered HCWs in both public and private health facilities representing aforementioned health professionals at December 2007 was 1,680 (Nasarawa State Ministry of Health (MOH), Lafia). The sample size used for this study was calculated with the formula (used when total study population is less than 10,000):
nf = n/1 + (n)/(N)
Where nf = the desired sample size when population is less than 10,000.
n = the desired sample size when population is more than 10,000.
N = the estimate of population size.
Hence, if n is approximated to be 400 derived from the formula, n = z2 pq/d2 , and N is 1,680 then nf = 400/1 + (400)/(1680) = 322.
Sampling technique
A multistage sampling technique was used to obtain a representative sample of the HCWs in the state.
Stage 1: Selection of local government areas
The first stage was the grouping or categorization of the two tertiary, 13 secondary, 13 comprehensive model primary healthcare facilities, and 36 registered private hospitals in the 12 local government areas in the state. In order to obtain a representative sample, two local government areas was selected by random sampling technique.
Stage 2: Selection of facilities surveyed
A total of 12 health facilities were sampled. This comprises of two tertiary facilities, two general hospitals, two comprehensive health facilities present in the local governments selected, and six registered private healthcare centers. The six registered private healthcare centers were selected using simple random sampling (by balloting).
Stage 3: Selection of study participants
Equal no of respondents (112 HCWs) were allocated to each tertiary, secondary, PHC, and private (mostly primary healthcare delivery) hospitals. Proportional sampling technique was used to obtain a representative sample of the HCWs in the state. The ratio of doctors to nurses in each hospital was used as the sampling scheme and hospital laboratory scientists and pharmacists were oversampled to allow for their adequate representation in the analysis.
A total of 421 randomly selected HCWs participated in the self-administered survey between January and February, 2009, with less than 5% refusal rate.
Research instrument
The instrument or tool used in this study was a self-administered questionnaire. The questionnaire was structured into three sections, namely: Biodata (demographic characteristics); knowledge of infection control, and universal precaution practice.
Assessment of knowledge of infection control was made by asking about the knowledge and practice of the core elements of universal precaution as developed by CDC.[10]
Single multiple response choice questions “Do you change gloves after each patient” was used to determine standard precaution practice.
Occupational exposure was determined by asking: Have you had needle stick injury or infected blood touches or splash on your skin cuts or wounds in the last 6 months?
This questionnaire was pretested on randomly selected 45 HCWs in the state representing about 10% of the required sample size. This was done to determine if the questions were clearly understood, hence necessary corrections or amendments were effected on the questionnaire before conducting the study.
Data collection
Data were collected from three different local government areas in a Nasarawa State. Participants consisted of service providers who were currently working at the healthcare facilities in the area. Most private hospitals in Nigeria are primary healthcare centers and usually unregistered with the State MOH especially those located in the rural areas. Public healthcare facilities in Nigeria are organized on three different levels: Tertiary, secondary, and primary healthcare. Generally, hospitals at higher levels (secondary and primary healthcare) serve a broader region and are more likely to have technologically advanced equipment and a more highly educated staff. Such hospitals have the capacity and resources to perform more sophisticated operations, and therefore also are more likely to attract more patients.
The questionnaire was pretested in November 2008 on 45 respondents who were randomly selected HCWs. All the necessary adjustments and corrections were made in the question sequence. Most of the questions except a few were close-ended. Precoding was done to allow for easy data capturing. Data collection was carried out by the investigator and a research assistant who possessed Senior Secondary School Certificate. The assistant was trained by the investigator on the research methodology and data collection procedure before the commencement of the research. At each selected health facility, the investigator explained to subjects the reasons for the study and its voluntary nature and sought for their cooperation before the distribution of questionnaires. An incentive of two biros (blue and red in color) was given to each participant.
Ethical consideration
Ethical approval was sort from the Ethics and Research Committee of the Nasarawa State MOH, evidence of which was an approval letter. It would be noteworthy to state that although the Specialist Hospital Lafia and the Federal Medical Centre Keffi had their own ethical and research committee, their management consented on presentation of the approval letter of the state MOH. A consent information sheet/form including information on confidentiality was designed which was used in seeking informed consent from healthcare facilities and individual respondents after explaining thoroughly the purpose, objectives, procedure, and methodology of the study to them. Respondents were informed that they were free to withdraw from the research at any point if they so wished. All survey data were collected anonymously. Individual informed consent was obtained prior to administration of the survey.
Data analysis
To describe patient characteristics, we calculated proportions and medians. For categorical variables, we compared proportions using chi-square tests and when appropriate, Fisher’s exact test. Chi-square was used to determine association between categorical variables and a P-value of less than 0.05 was considered significant. Data was presented in tabular form.
A logistic regression model was produced with infection control as outcome variable to identify associated factors. All explanatory variables that were associated with the outcome variable in bivariate analyses, variables with a P-value of ≤0.05 were included in the logistic models.
RESULTS
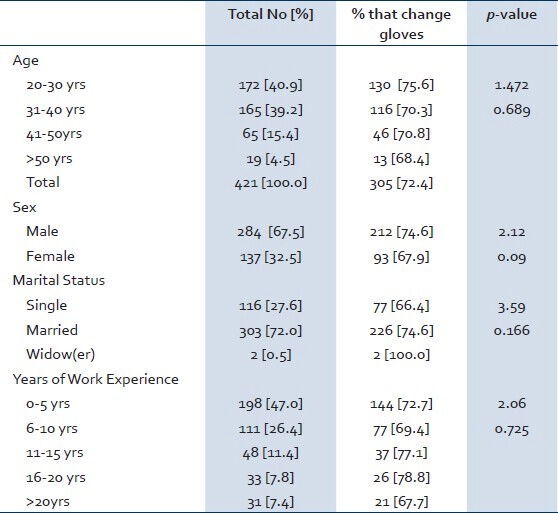
A total of 421 health workers were interviewed, 284 (67.5%) were males and 137 (32.5%) were females. Majority (77.2%) of the participants were aged 20-39 years, and only one (0.25%) and two (0.5%) were less than 20 years and greater than 60 years, respectively. The mean age of the health workers studied was 34.09 years (standard deviation (SD) = 8.1) and the mean year of experience at work was 8.24 years (SD = 7.53). Among the health workers, 47.0% have been working for 5 years or less, 26.4% for 6-10 years, 11.4% for 11-15 years and 15.2% for more than 15 years and above. Three hundred and three (72.0%) were married and 116 (27.6%) were singles, and only two (0.5%) were widower. Precisely, 309 (73.4%) were selected from government hospital and 112 (26.6%) from private health facilities. Fifty-two (12.4%) were medical doctors, 78 (18.5%) were nurses, 54 (12.8%) were laboratory scientists, 53 (12.6%) were pharmacists, 57 (13.5%) were community health workers, 74 (17.6%) were hospital orderlies, and 53 (12.6%) were from other professions in the hospital. The sociodemographic characteristics of the participants are summarized in Table 1. Sixty-four percent of the facilities surveyed reported not having antiretroviral medications in their facility. Moreover, the availability of other medications and dietary supplements was limited, and protective materials and other supplies and utilities were not always available.
Knowledge of infection control in hospital environment
Majority (77.9%) of the respondents were able to correctly describe universal precaution and infection control. Almost all of the respondents were able to recognize hand washing technique (100%), sterilization process (100%), and various equipments used for personal protection (99.8%), appropriate handling of the patients care equipments and soiled linen (96.2%), prevention of NSI (99.8%), environmental cleaning and spills management (99.3%), and appropriate handling of waste (99.5%) as essential technique of universal precautions for infection control. However, some of the HCWs could not recognize vaccination (19.2%), postexposure prophylaxis (19.2%), and surveillance for emerging diseases (28.0%) as standard precaution for infection control. Only 2.1% are aware of National Injection Safety Policy and 1.9% aware of Policy on Sharps Disposal. Only 8.1% had attended any workshop or training in infection control in the last 2 years and almost all of the respondents admit training needs on infection control and express willingness to attend such trainings if organized.
Standard precaution practices
Only 70.1% usually wear gloves before handling patients or patients’ care products, but 2.6% reported hand washing before wearing the gloves, 10.7% wash hands after removal of gloves, and 72.4% change gloves after each patient. About 20.2% usually wear face mask and 35.6% wear protective garments when necessary.
Furthermore, 14.3% reported that they do not sterilize instruments before use and 39.7% could not disinfect working surfaces when necessary. Only 3.3% of respondents reported reuse of needles and blades and 5.7% reuse disposable items regularly. Only 3.3% had a sharp disposal system in their various workplaces. Majority 98.6% of the respondents reported that the major reason for noncompliance to universal precautions is the nonavailability of the equipments. However, 39.7% reported that they do not have a functioning autoclave.
Factors associated with practice of standard precaution
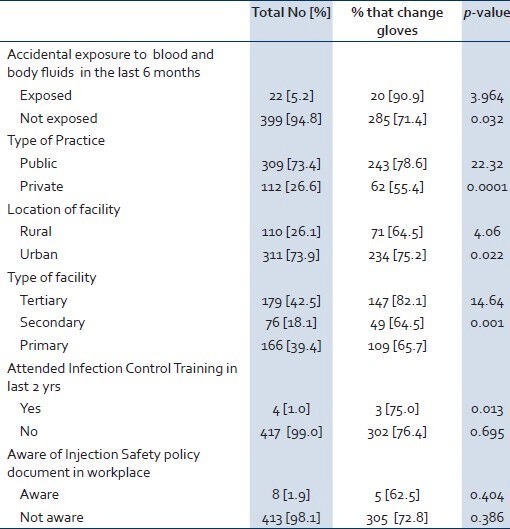
There was a statistically significant difference in the practice of standard precaution among those that were exposed to blood products and body fluid compared to those that had not been exposed in the last 6 months (χ2 = 3.96, P = 0.03), public healthcare providers when compared to private health workers (χ2 = 22.32, P = 0.001), among those working in secondary and tertiary facilities compared to primary healthcare centers (χ2 = 14.64, P = 0.001), and urban areas when compared to rural areas (χ2 = 4.06, P = 0.02).
There was however no statistically significant difference in the practice of standard precaution among the male providers compared to females (P = 0.09), age of health workers (P = 0.69), years of experience on the job (P = 0.73), and marital status (P = 0.17). Awareness of National policy on injection safety was not statistically significantly associated with practice of universal precaution among healthcare providers (χ2 = 0.404, P = 0.39). Similarly, recent training in infection control practices was not significantly associated with the practice of universal precaution (χ2 = 0.013, P = 0.70). This is illustrated in Table 2.
Table 2.
Universal precaution and workplace characteristics
In the multiple logistic regression models, four variables were entered into the model. The only factor found to be independently associated with the practice of universal precaution was exposure to blood and body fluid in the last 6 months odds ratio (OR) = 4.56 (confidence interval (CI) = 1.00-21.28). This is shown in Table 3.
Table 3.
Multivariate analysis

DISCUSSION
The study shows that many of the facilities in this study did not even have equipments and sufficient medication. The lack of protective materials and other supplies and utilities documented in the health facility survey and cited also by professionals as the main reason for not applying standard precautions may be a major factor in noncompliance to universal precautions. Health worker surveys and observations in Nigeria and elsewhere in Africa document that health workers often fail to practice standard precautions consistently and correctly.[15,16,17,18,19,20,21,22,23] Although there has been controversy about how much HIV transmission in Africa is due to unsafe healthcare practices[24,25] eliminating all unsafe practices in health facilities should be an urgent priority for HIV prevention and for overall infection control.
In this study, incorrect practices which include failure to wash hands and to use gloves, unsafe handling and disposal of sharps, and unsafe cleaning procedures were predominant among private healthcare providers when compared to public health workers, and among those working in the rural areas when compared to urban areas. This study implies that the issue of access to affordable treatment and the lack of equipment required to ensure safety of HCWs and prevent the spread of infectious disease from patients to health workers is a crucial issue that need urgent attention in Nigeria and other low income countries in Africa. This will prevent the spread of HIV and related conditions among the health workers and may reduce discriminatory behavior.[26]
Majority of the respondents were able to correctly describe standard precaution in infection control. However, some of the HCWs could not recognize vaccination, postexposure prophylaxis, and surveillance for emerging diseases as standard precaution for infection control. Inadequate worker knowledge and health system problems, including staff shortages, and inadequate staff training and supervision, contribute to these unsafe practices.[27,28,29] Implementing a training package may help, but systems need to be in place as well. Universal precautions provide protection from a range of blood-borne pathogens, but their effectiveness relies upon the knowledge of HCWs and the level of compliance in their use.[30]
Only 3.3% had a sharp disposal system in their various workplaces and very few workers are aware of National Injection Safety Policy and Policy on Sharps Disposal. Several effective evidence based interventions for reducing the occurrence of hospital acquired infections (HAIs) have been proposed, and specific guidelines aimed at preventing the transmission of pathogens within the hospital setting developed, but maintenance of a surveillance system for HAIs has been found to be of utmost importance.[31] Other strategies that may facilitate adoption of universal precautions may include initiation of institutional NSI quality improvement project, vigorous education, and regular audits.[32]
The fact that a significantly higher proportion of those that were exposed to blood products and body fluid began to practice universal precaution shows that the wearing of gloves is an important line of defense. This has been reported by several studies.[33,34,35] As a consequence of inconsistent use of universal precautions, health workers put themselves and their clients at potential risk. African health workers fear occupational exposure, this may further undermines their morale.[17,18,33,34] Institution of a surveillance system for HAIs is hereby recommended to improve consistent use of universal precautions among health workers.
Few health workers had attended any workshop or training in infection control in the last 2 years and almost all of the respondents admit training needs on infection control and express willingness to attend such trainings if organized. Awareness of National Policy on Injection Safety was not statistically significantly associated with practice of universal precaution among healthcare providers. Similarly, recent training in infection control practices was not significantly associated with the practice of universal precaution. Few health worker training programs have been systematically evaluated. Two interventions in Nigeria significantly improved health workers’ HIV-related knowledge, attitudes, and perceived counseling and treatment skills.[35,36] However, one of these studies did not address health system barriers, and the use of universal precautions did not improve due to continued lack of supplies.[36] Another study found that mental healthcare providers in South Africa had more knowledge and felt more comfortable about HIV care after training.[37] Some African countries have successfully trained selected health workers in counseling and testing and/or home-based care.[35] However, studies have reported that education, ongoing quality improvement projects, and preventive programs play a major role in augmentation of knowledge and safe behavior of HCWs.[38,39]
Given the cross-sectional nature of the results, interpretation of study results is restricted. Future research with a longitudinal approach would be valuable. Our analyses identified significant relations, but their relative strengths were often weak. A major limitation is that our research investigated occupational exposure retrospectively; this may be faced with recall bias. However, our study findings might represent the actual situation since we dealt with professionals and such experience of occupational exposure in times of pandemic of the HIV/AIDS disease may be very difficult to forget. It would be interesting to conduct a follow-up study to gain insight into whether and how disease state could emerge from these occupational exposures.
CONCLUSION
This study concludes that inadequate workers’ knowledge and environment related problems, including lack of protective materials and other equipments and utilities required to ensure safety of HCWs is a crucial issue that needs urgent attention. Institution of a surveillance system for hospital acquired infection to improve consistent use of standard precautions among health workers is recommended in Nigeria and other low income countries in Africa.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- 1.Shiao J, Guo L, McLaws ML. Estimation of the risk of blood borne pathogens to health care workers after a needlestick injury in Taiwan. Am J Infect Control. 2002;30:15–20. doi: 10.1067/mic.2002.119928. [DOI] [PubMed] [Google Scholar]
- 2.Worker Health Chart book 2004. Blood borne Infections and Percutaneous Exposures DHHS (NIOSH) Publication No. 2004:146. [Google Scholar]
- 3.Eriksen HM, Iversen BG, Aavitsland P. Prevalence of nosocomial infections in hospitals in Norway, 2002 and 2003. J Hosp Infect. 2005;60:40–5. doi: 10.1016/j.jhin.2004.09.038. [DOI] [PubMed] [Google Scholar]
- 4.Pittet D, Allegranzi B, Sax H, Bertinato L, Concia E, Cookson B, et al. Considerations for a WHO European strategy on health-care-associated infection, surveillance, and control. Lancet Infect Dis. 2005;5:242–50. doi: 10.1016/S1473-3099(05)70055-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Hopmans TE, Blok HE, Troelstra A, Bonten MJ. Prevalence of hospital-acquired infections during successive surveillance surveys conducted at a university hospital in the Netherlands. Infect Control Hosp Epidemiol. 2007;28:459–65. doi: 10.1086/512640. [DOI] [PubMed] [Google Scholar]
- 6.Klevens RM, Edwards JR, Richards CL, Jr, Horan TC, Gaynes RP, Pollock DA, et al. Estimating health care-associated infections and deaths in U.S. hospitals, 2002. Public Health Rep. 2007;122:160–6. doi: 10.1177/003335490712200205. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Pittet D, Allegranzi B, Storr J, Bagheri Nejad S, Dziekan G, Leotsakos A, et al. Infection control as a major World Health Organization priority for developing countries. J Hosp Infect. 2008;68:285–92. doi: 10.1016/j.jhin.2007.12.013. [DOI] [PubMed] [Google Scholar]
- 8.Chan R, Molassiootis A, Chan E, Chan V, Ho B, Lai CY, et al. Nurses’ knowledge of and compliance with universal precaution in an acute care hospital. Int J Nurs Stud. 2002;39:157–63. doi: 10.1016/s0020-7489(01)00021-9. [DOI] [PubMed] [Google Scholar]
- 9.Sridhar MR, Boopathi S, Lodha R, Kabra SK. Standard precautions and post exposure prophylaxis for preventing infection. Indian J Paediatr. 2004;71:617–25. doi: 10.1007/BF02724121. [DOI] [PubMed] [Google Scholar]
- 10.Centers for Disease Control (CDC) Recommendations for prevention of HIV transmission in health-care settings. MMWR Morb Mortal Wkly Rep. 1987;36:1–18S. [PubMed] [Google Scholar]
- 11.Centers for Disease Control. Update: Universal precautions for prevention of transmission of human immunodeficiency virus, hepatitis B virus, and other bloodborne pathogens in health-care settings. MMWR Morb Mortal Wkly Rep. 1988:377. [PubMed] [Google Scholar]
- 12.Garner JS. The Hospital Infection Control Practices Advisory Committee. Guideline for isolation precautions in hospitals The Hospital Infection Control Practices Advisory Committee. Infect Control Hosp Epidemiol. 1996;17:53–80. doi: 10.1086/647190. [DOI] [PubMed] [Google Scholar]
- 13.Leganani P, Checchi L, Pellicioni GA, D’Achille C. Atmospheric contamination during dental procedures. Quintessence Int. 1994;25:435–9. [PubMed] [Google Scholar]
- 14.Center for disease control and prevention (CDC) and hospital control practices advisory committee (HICPAC) Guideline for disinfection and sterilization in health care facilities. 2008 [Google Scholar]
- 15.Garbus L. HIV and AIDS in Malawi: Country AIDS policy analysis project. San Francisco, CA: Policy Research Center, University of California San Francisco; 2003. [Google Scholar]
- 16.Mbanya DN, Zebaze R, Kengne AP, Minkoulou EM, Awah P. Beure Knowledge, attitudes and practices of nursing staff in a rural hospital of Cameroon: How much does the health care provider know about the human immunodeficiency virus/acquired immune deficiency syndrome? Int Nurs Rev. 2001;48:241–9. doi: 10.1046/j.1466-7657.2001.00090.x. [DOI] [PubMed] [Google Scholar]
- 17.Newsom DH, Kiwanuka JP. Needle-stick injuries in an Ugandan teaching hospital. Ann Trop Med Parasitol. 2002;96:517–22. doi: 10.1179/000349802125001186. [DOI] [PubMed] [Google Scholar]
- 18.Nsubuga FM, Jaakkola MS. Needle-stick injuries among nurses in sub-Saharan Africa. Trop Med Int Health. 2005;10:773–81. doi: 10.1111/j.1365-3156.2005.01453.x. [DOI] [PubMed] [Google Scholar]
- 19.Orji EO, Fasubaa OB, Onwudiegwu U, Dare FO, Ogunniyi SO. Occupational health hazards among health workers in an obstetrics and gynaecology unit of a Nigerian teaching hospital. J Obstet Gynaecol. 2002;22:75–8. doi: 10.1080/01443610120101781. [DOI] [PubMed] [Google Scholar]
- 20.Reis C, Heisler M, Amowitz LL, Moreland RS, Mafeni JO, Anyamele C, et al. Discriminatory attitudes and practices by health workers towards patients with HIV/AIDS in Nigeria. PLos Med. 2005;2:e246. doi: 10.1371/journal.pmed.0020246. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Sadoh WE, Fawole AO, Sadoh AE, Oladimeji AO, Sotiloye OS. Practice of universal precautions among healthcare workers. J Natl Med Assoc. 2006;98:722–6. [PMC free article] [PubMed] [Google Scholar]
- 22.Talashek ML, Kaponda CP, Jere DL, Kafulafula U, Mbeba MM, McCreary LL, et al. Identifying what rural health workers in Malawi need to become HIV prevention leaders. J Assoc Nurses AIDS Care. 2007;18:41–50. doi: 10.1016/j.jana.2007.05.007. [DOI] [PubMed] [Google Scholar]
- 23.Walusimbi M, Okonsky JG. Knowledge and attitude of nurses caring for patients with HIV/AIDS in Uganda. Appl Nurs Res. 2004;17:92–9. doi: 10.1016/j.apnr.2004.02.005. [DOI] [PubMed] [Google Scholar]
- 24.Gisselquist D, Potterat JJ. Review of evidence from risk factor analyses associating HIV infection in African adults with medical injections and multiple sexual partners. Int J STD AIDS. 2004;15:222–33. doi: 10.1258/095646204773557730. [DOI] [PubMed] [Google Scholar]
- 25.Schmid GP, Buve A, Mugyenyi P, Garnett GP, Hayes RJ, Williams BJ, et al. Transmission of HIV-1 infection in sub-Saharan Africa and effect of the elimination of unsafe injections. Lancet. 2004;363:482–8. doi: 10.1016/S0140-6736(04)15497-4. [DOI] [PubMed] [Google Scholar]
- 26.Smith DR, Smyth W, Leggat PA, Wang RS. Needlestick and sharp injuries among nurses in a tropical Australian hospital. Int J Nurs Pract. 2006;12:71–7. doi: 10.1111/j.1440-172X.2006.00553.x. [DOI] [PubMed] [Google Scholar]
- 27.Ansa VO, Udoma EJ, Umoh MS, Anah MU. Occupational risk of infection by human immunodeficiency and hepatitis B viruses among health workers in south-eastern Nigeria. East Afr Med J. 2002;79:254–6. doi: 10.4314/eamj.v79i5.8863. [DOI] [PubMed] [Google Scholar]
- 28.Chelenyane M, Endacott R. Self-reported infection control practices and perceptions of HIV/AIDS risk amongst emergency department nurses in Botswana. Accid Emerg Nurs. 2006;14:148–54. doi: 10.1016/j.aaen.2006.03.002. [DOI] [PubMed] [Google Scholar]
- 29.Hesse A, Adu-Aryee N, Entsua-Mensah K, Wu L. Knowledge, attitude and practice universal basic precautions by medical personnel in a teaching hospital. Ghana Med J. 2006;40:61–4. doi: 10.4314/gmj.v40i2.36019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Metcalfe A. Universal precautions: A review of knowledge, compliance and strategies to improve practice. J Res Nurs. 2005;10:549–50. [Google Scholar]
- 31.Siegel JD, Rhinehart E, Jackson M, Chiarello L. The Health Care Infection Control Practices Advisory Committee 2007. Guideline for isolation precautions: Preventing transmission of infectious agents in healthcare settings. [Last Accessed on 2007 Jun 30]. Available from: http://www.cdc.gov/ncidod/dhqp/pdf/guidelines/Isolation2007.pdf . [DOI] [PMC free article] [PubMed]
- 32.Williams CO, Campbell S, Henry K, Collier P. Variables influencing workers compliance with universal precautions in the emergency department. Am J Infect Control. 1994;122:138–48. doi: 10.1016/0196-6553(94)90002-7. [DOI] [PubMed] [Google Scholar]
- 33.Whitby RM, McLaws ML. Hollow-bore needlestick injuries in a tertiary teaching hospital: Epidemiology, education and engineering. Med J Aust. 2002;177:418–22. doi: 10.5694/j.1326-5377.2002.tb04881.x. [DOI] [PubMed] [Google Scholar]
- 34.Ebrahimi H, Khosravi A. Needlestick injuries among nurses. J Res Health Sci. 2007;7:56–62. [PubMed] [Google Scholar]
- 35.Ezedinachi EN, Ross MW, Meremiku M, Essien EJ, Edem CB, Ekure E, et al. The impact of an intervention to change health workers’ HIV/AIDS attitudes and knowledge in Nigeria: A controlled trial. Public Health. 2002;116:106–12. doi: 10.1038/sj.ph.1900834. [DOI] [PubMed] [Google Scholar]
- 36.Uwakwe CB. Systematized HIV/AIDS education for student nurses at the University of Ibadan, Nigeria: Impact on knowledge, attitudes and compliance with universal precautions. J Adv Nurs. 2000;32:416–24. doi: 10.1046/j.1365-2648.2000.01492.x. [DOI] [PubMed] [Google Scholar]
- 37.Collins PY, Mestry K, Wainberg ML, Nzama T, Lindegger G. Training South African mental health care providers to talk about sex in the era of AIDS. Psychiatr Serv. 2006;57:1644–7. doi: 10.1176/appi.ps.57.11.1644. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Sokas RK, Simmens S, Scott J. A training pro gram in universal precautions for second year medical students. Acad Med. 1993;68:374–6. doi: 10.1097/00001888-199305000-00022. [DOI] [PubMed] [Google Scholar]
- 39.Wang H, Fennie K, He G, Burgess J, Williams AB. A training program for prevention of occupational exposure to blood borne pathogens: Impact on knowledge, behavior and incidence of needle stick injuries among student nurses in Changsha, People’s Republic of China. J Adv Nurs. 2003;41:187–94. doi: 10.1046/j.1365-2648.2003.02519.x. [DOI] [PubMed] [Google Scholar]