

Sir,
Kawasaki disease (KD) is a self-limiting vasculitis of small vessels with special tropism for coronary arteries. It usually affects infants and children, and its main complication is the development of coronary aneurysm or ectasias.
Treatment is aimed at reducing the risk of coronary injuries (20% incidence in untreated or treatment-resistant patients). Actual guidelines recommend intravenous gamma globulin (IVIG) as the first-line treatment and high doses of corticosteroids for refractory cases. Infliximab has been used as a rescue treatment in refractory cases of KD.[1]
We report a case of severe KD in a 7-year-old boy who developed cardiac congestive failure due to myocarditis and a giant coronary aneurism in the acute phase of the disease [Figure 1]. In this case, treatment with two doses of IVIG and various pulses of intravenous corticoids was ineffective. Finally, the patient was responsive to a single dose of infliximab [Figure 2]. Besides, we treated him with enalapril and furosemide for the congestive heart failure and with low-molecular-weight heparin and aspirin to prevent thrombotic events.
Figure 1.
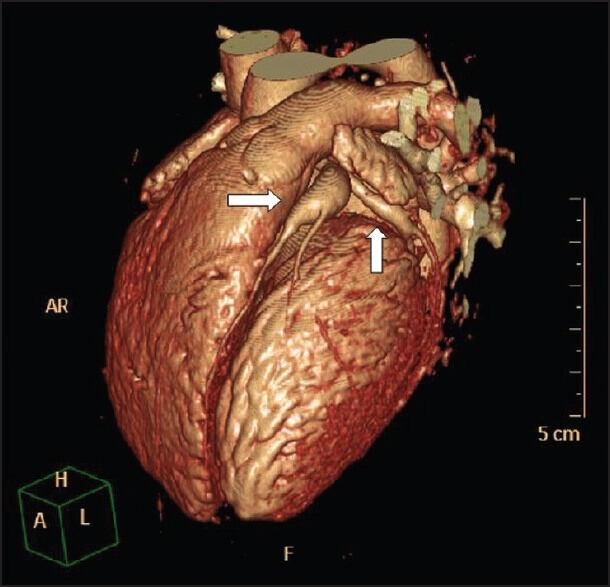
3D reconstructed image of coronary CT angiography, showing aneurysm in the anterior descending coronary artery (9 × 22 mm) and ectasia of circumflex coronary artery (5 × 3.5 mm) (arrows)
Figure 2.
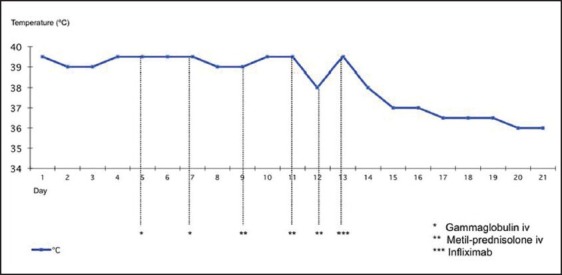
Graph representing the clinical course (fever) of the patient. Note the persistence of fever with the application of conventional treatment and first-line rescue therapy (IVIG and corticoids). After administering infliximab (on the 13th day of disease), a progressive decrease in body temperature was observed until it reached normal levels
Eighteen months after being discharged, the patient remained asymptomatic, revealing no ischemic events. Nevertheless, the echocardiography revealed persistence of the same coronary lesions as the only pathological finding, so the patient was continued on a double platelet antiaggregant and oral anticoagulation treatment.
Although the first-line IVIG treatment is widely accepted and supported by broad evidence for the prevention of coronary aneurysms, up to ≥10% of patients do not respond to this treatment. In addition to the treatment of refractory cases, which present with greater incidence of severe coronary lesions, some experts recommend a new infusion of IVIG without strong evidence to support this measure, as it occurs with corticoid therapy and other treatments such as pentoxyfiline or plasmapheresis.[1]
Infliximab is a chimeric IgG1 monoclonal antibody that binds specifically to tumor necrosis factor-alpha (TNF-α), which is implicated in the physiopathology of KD.[2] Although its use is not widespread, it has been successfully applied in certain cases of KD which are refractory to first-line therapy.[3,4,5]
According to some case reports, this biological therapy appears to be superior to IVIG as the second-line treatment in terms of fever duration and length of hospitalization,[3,4] although it has not been proven to be as efficient in terms of coronary aneurysm development.[4] In our case, treatment with infliximab was delayed. It was only started after administration of two doses of IgG with no success, as well as corticosteroid treatment in pulses. Even though more trials with greater statistical power are required to assess the efficiency of infliximab as the rescue therapy for KD, we propose its use as a first option in the second-line treatment, after an unsuccessful first dose of IVIG in KD patients, especially in those with severe cardiac involvement, such as the case that is presented here.
REFERENCES
- 1.Newburger JW, Takahashi M, Gerber MA, Gewitz MH, Tany LY, Burns JC, et al. Diagnosis, treatment and long-term management of Kawasaki disease: A statement for health professionals from the committee of rheumatic fever, endocarditis and Kawasaki disease, council on cardiovascular disease in the young, American Heart Association. Pediatrics. 2004;114:1708–33. doi: 10.1542/peds.2004-2182. [DOI] [PubMed] [Google Scholar]
- 2.Díaz-Orta MA, Rojas-Serrano J. Biologic therapies in the systemic vasculitides. Reumatol Clin. 2011;7(Suppl 3):S33–6. doi: 10.1016/j.reuma.2011.09.001. [DOI] [PubMed] [Google Scholar]
- 3.Burns JC, Best BM, Mejias A, Mahoney L, Fixler DE, Jafri HS, et al. Infliximab treatment of intravenous immunoglobulin-resistant Kawasaki disease. J Pediatr. 2008;153:833–8. doi: 10.1016/j.jpeds.2008.06.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Son MB, Gauvreau K, Burns JC, Corinaldesi E, Tremoulet AH, Watson VE, et al. Infliximab for intravenous immunoglobulin resistance in Kawasaki disease: A retrospective study. J Pediatr. 2011;158:644–9. doi: 10.1016/j.jpeds.2010.10.012. [DOI] [PubMed] [Google Scholar]
- 5.Mori M, Imagawa T, Hara R, Kikuchi M, Hara T, Nozawa T, et al. Efficacy and limitation of Infliximab treatment for children with Kawasaki disease intractable to intravenous immunoglobulin therapy: Report of an open-label cases series. J Rheumatol. 2012;39:864–7. doi: 10.3899/jrheum.110877. [DOI] [PubMed] [Google Scholar]