

Abstract
A 55-year-old female presented with bilateral progressive retinal vasculitis. She was on systemic and intravitreal steroids on the basis of uveitis work-up result (negative result including rapid plasma reagin), but her visual acuity continued to deteriorate to light perception only. Ocular examination showed retinal vasculitis, multiple yellow placoid lesions and severe macula edema in both eyes. Repeated work-up revealed positivity of fluorescent treponemal antibody-absorption in serum and subsequently in cerebrospinal fluid. Ocular syphilis was diagnosed. And intravenous penicillin G resulted in rapid resolution of vasculitis and macular edema. To avoid delay in the diagnosis of ocular syphilis, high index of suspicion and repeating serological tests (including both treponemal and non-treponemal tests) are warranted.
Keywords: Delayed diagnosis, intravitreal triamcinolone injection, ocular syphilis, rapid plasma reagin test, retinal vasculitis
Ocular syphilis has no typical manifestation and the serologic tests are insufficiently sensitive, especially in late-stage syphilis. These often lead to delayed diagnosis and antibiotic management.[1,2] We herein, describe a case of delayed diagnosis of ocular syphilis with manifestation of bilateral progressive steroid-resistant retinal vasculitis, resulting in serious visual loss.
Case Report
A 55-year-old female patient hospitalized with a history of bilateral progressive visual loss for 4 months. Initial work-up done elsewhere revealed all tests including rapid plasma reagin (RPR) were negative. She then, had been treated with the high dose systemic steroids followed by bilateral intravitreal triamcinolone injection, but her eyes continued to deteriorate.
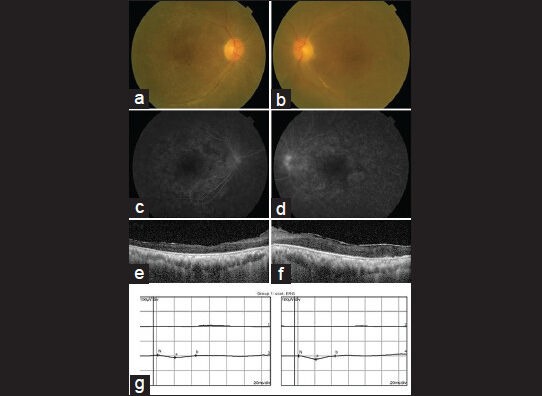
Best corrected visual acuity (VA) was light perception in both eyes. Biomicrocopy revealed a few inflammatory cells and fundoscopy showed disc edema, multiple yellow placoid lesions and vasculitis in both eyes [Fig. 1a and b]. Fluorescein angiography demonstrated early hypofluorescence and late leakage from the placoid lesions [Fig. 1c and, d]. Indocyanine green angiography was not performed. Optical coherence tomography revealed severe macular intraretina edema in both [Fig. 1e and f] eyes as well as a serous retinal detachment in the right eye [Fig. 1e].
Figure 1.

(a and b) Fundus photograph shows multiple retinal placoid lesions, disc edema and vasculitis. (c and d) Fluorescein angiogpaphy showed hypofluorescent placoid lesion in the early phase (c) and late leakage from retinal vessels and lesions (d). (e and f) Optical coherence tomography shows severe intraretinal edema in both eyes (e: right eye, f: left eye) as well as a serous retinal detachment in the right eye (e)
We repeated serologic tests including viral polymerase chain reaction, toxoplasma antibody, rheumatoid factor, antinuclear antibody, human leukocyte antigen B27, human immunodeficiency virus (HIV) antigen/antibody and fluorescent treponemal antibody-absorption (FTA-ABS). Whereas all other tests were negative, FTA-ABS test was positive. Subsequent tests for cerebrospinal fluid also revealed positivity in FTA-ABS and Venereal Disease Research Laboratory (VDRL). The titer of VDRL was 1:8. While she denied any history of previous systemic diseases, systemic evaluation revealed recent skin rashes on her palms and soles, which appeared to be characteristic signs of secondary syphilis [Fig. 2a and b].
Figure 2.

Multiple rashes, typical skin lesions of secondary syphilis were observed at palms (a) and soles (b)
Taken all together, she was diagnosed as secondary syphilis. After 2 weeks of intravenous penicillin G treatment (4 million units of aqueous penicillin G, 6 times a day), her vision slightly improved to hand motion in the right eye and finger count 30 cm in the left eye. Ocular examination showed a resolution of vasculitis and macular edema in her both eyes.
Due to the delayed diagnosis, despite the massive intravenous antibiotic treatment, visual recovery was poor. On the last follow-up of 4 months following treatment, her VA was hand motion in the right eye and 0.03 in the left eye. There was no sign of active inflammation, but visual recovery was poor due to optic atrophy [Fig. 3a and b] and macular ischemic thinning [Fig. 3c and d]. While the central retinal thickness was significantly decreased, the subfoveal choroidal thickness seemed to be unaffected when examined with an enhanced depth imaging optical coherence tomography (Spectralis HRA-OCT; Heidelberg Engineering, Heidelberg, Germany) [Fig. 3e and f]. Scotopic electroretinogram showed extinguished wave in both eyes.[Fig. 3g]
Figure 3.
(a and b) Fundus photographs taken 4 months after penicillin treatment showed complete resolution of active inflammation. However, entire retina became atrophic with retinal vascular attenuation. (c and d) Fluorescein angiographiy of the late stage showed macular ischemia. (e and f) Spectral domain-optical coherence tomography images of both eyes revealed resolution of macular edema. Whereas the central retinal thickness decreased markedly with a total disruption of photoreceptor inner/outer-segment band, the subfoveal choroidal thickness seemed to be unaffected. (e: right eye, f: left eye) (g) Scotopic electroretinogram showed extinguished wave in both eyes
Discussion
We have shown a patient with bilateral ischemic retinal vasculitis who resulted in serious visual loss due to delayed diagnosis of ocular syphilis. Although the advent of antibiotics had decreased the incidence of syphilis significantly, there are still about 12 million patients suffering from syphilis world-wide. In addition, there has been a recent increase of syphilis, most particularly among homosexual males as a co-infection with HIV.[1,2,3,4] Therefore, the importance of accurate and early diagnosis of ocular syphilis has again become significant.
Early diagnosis of ocular syphilis is quite difficult.[5] Several other conditions, which could be manifested as retinal vasculitis and focal chorioretinitis including infectious conditions such as tuberculosis or toxoplasmosis, as well as non-infectious inflammatory conditions such as sarcoidosis or Vogt-Koyanaki-Harada syndrome should be ruled out. As there are no established criteria for Ophthalmologists directing when to suspect syphilis and order serologic tests, high index of suspicion and early accurate diagnostic intervention are crucial for the differential diagnosis of ocular syphilis. The non-treponemal tests such as VDRL or RPR are insufficiently sensitive especially in the late stages of syphilis and in the very early stages. The sensitivity and specificity of treponemal tests are higher; however, false-negative and false-positive results could be observed. Therefore, if syphilis is suspected, both treponemal and non-treponemal tests should be considered. Furthermore, the possibility of syphilis should not be ignored with just a single negative test result.
Our case represents an example of ocular syphilis with a delay in diagnosis due to lack of accuracy, which led to serious visual loss. In our case, the low sensitivity of the test itself, laboratory error or the prozone phenomenon, which means a falsely negative test due to very high titers of antibody could be considered to be the cause for the negative result of initial RPR test.[6] Recently, acute syphilitic posterior placoid chorioretinitis have been reported in immunocompromised hosts such as HIV infected patients[7] or patients with intravitreal steroid injection.[8] Our case also showed acute syphilitic posterior placoid chorioretinitis after intravitreal steroid injection, which might have activated a dormant syphilitic infection inside the eye. In our case, the patient had been treated with intravitreal triamcinolone based on the false-negative result of serum RPR test. Although the previous report[7] recommended a high index of suspicion for syphilitic uveitis among patients without a history of syphilis, our case emphasizes the possibility of false-negative result of serum rapid plasma reagin test. Our case is suitable for reminding important two points that are often overlooked in uveitis cases. First, infectious cause should be excluded before steroid is prescribed. Second, doctors should not rely on serological tests only, especially non-treponemal tests such as RPR or VDRL.
Conclusion
It is very important to make an early diagnosis of ocular syphilis for the best outcome. To reach the goal, high index of suspicion is warranted considering the lack of diagnostic accuracy in a single serologic test.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
References
- 1.Aldave AJ, King JA, Cunningham ET., Jr Ocular syphilis. Curr Opin Ophthalmol. 2001;12:433–41. doi: 10.1097/00055735-200112000-00008. [DOI] [PubMed] [Google Scholar]
- 2.Muldoon EG, Hogan A, Kilmartin D, McNally C, Bergin C. Syphilis consequences and implications in delayed diagnosis: Five cases of secondary syphilis presenting with ocular symptoms. Sex Transm Infect. 2010;86:512–3. doi: 10.1136/sti.2009.041863. [DOI] [PubMed] [Google Scholar]
- 3.Chao JR, Khurana RN, Fawzi AA, Reddy HS, Rao NA. Syphilis: Reemergence of an old adversary. Ophthalmology. 2006;113:2074–9. doi: 10.1016/j.ophtha.2006.05.048. [DOI] [PubMed] [Google Scholar]
- 4.Chhablani JK, Biswas J, Sudharshan S. Panuveitis as a manifestation of ocular syphilis leading to HIV diagnosis. Oman J Ophthalmol. 2010;3:29–31. doi: 10.4103/0974-620X.60019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Kiss S, Damico FM, Young LH. Ocular manifestations and treatment of syphilis. Semin Ophthalmol. 2005;20:161–7. doi: 10.1080/08820530500232092. [DOI] [PubMed] [Google Scholar]
- 6.Singh AE, Wong T, De P. Characteristics of primary and late latent syphilis cases which were initially non-reactive with the rapid plasma reagin as the screening test. Int J STD AIDS. 2008;19:464–8. doi: 10.1258/ijsa.2007.007302. [DOI] [PubMed] [Google Scholar]
- 7.Eandi CM, Neri P, Adelman RA, Yannuzzi LA, Cunningham ET, Jr International syphilis study group. Acute syphilitic posterior placoid chorioretinitis: Report of a case series and comprehensive review of the literature. Retina. 2012;32:1915–41. doi: 10.1097/IAE.0b013e31825f3851. [DOI] [PubMed] [Google Scholar]
- 8.Song JH, Hong YT, Kwon OW. Acute syphilitic posterior placoid chorioretinitis following intravitreal triamcinolone acetonide injection. Graefes Arch Clin Exp Ophthalmol. 2008;246:1775–8. doi: 10.1007/s00417-008-0928-y. [DOI] [PubMed] [Google Scholar]