

Abstract
Background: This study was planned to assess the dental caries status among disabled children as dental health is an integral part of general body health and this group is deprived of health care needs.
Materials & Methods: A sample of 310 disabled children was gathered including 195- Hearing impaired, 115 – blind. Of which 226 were males and 84 were females. A study questionnaire was prepared to include demographic information and WHO oral health assessment form (1997) to record dental caries status.Data was analysed using student’s test and ANOVA test was used at p≤0.05. Results: The overall mean for DMFT scores for males and females was 2.11 (1.753) and 1.75 (1.275) respectively. Similarly overall mean for dft was 0.31 (0.254) for males and 0.27 (0.143) for females. Mean DMFT of blind students was more as compared to hearing impaired ones as 2.16 (2.005) and 1.80 (1.264) respectively. Age factor showed a significant increase in the mean DMFT scores with advancing age at p ≤ 0.001. Conclusion: Overall mean scores of caries was very high and it increased with increasing age. Blind children experienced more caries then hearing impaired children in permanent, whereas it was opposite in primary dentition. So there is urgent need of both comprehensive and incremental dental care for this subgroup of population.
How to cite the article: Sanjay V, Shetty SM, Shetty RG, Managoli NA, Gugawad SC, Hitesh D. Dental health status among sensory impaired and blind institutionalized children aged 6 to 20 years. J Int Oral Health 2014;6(1):55-8.
Key Words: : Blind, dental caries, hearing impaired children
Introduction
The disabled form a considerable section of the community, and it is estimated that there are about 500 million people with disabilities worldwide 1 and they are on the increase in proportion to the general population. 2 The American Health Association defines a child with disability as a child who for various reasons cannot fully make use of all his or her physical, mental and social abilities. 3 Patients with disabilities consist of a unique population deserving special consideration. Previously, they have been ignored or even hidden away in institutions.
Dental care is the most common unmet need of disabled children. 4 Good oral health is imperative for proper mastication; appearance and speech. 5 Children with disabilities appear to have poorer oral health than their non-disabled counterparts. Variable access to dental care, inadequate oral hygiene and many other disability-related
factors may account for differences however their diet, medication, physical limitations, lack of oral hygiene and the attitude of their parents and the health care providers all contribute to the poor oral health. Individuals with various impairments have greater limitations in oral hygiene performance due to their potential motor, sensory and intellectual disabilities and are thus are prone to poor oral health. 6
Dental Caries is the most common chronic oral disease of childhood that interferes with normal nutrition intake, speech and daily regular activities, because its pain adversely affects the normal food eating. A normal child gets the benefits of love and affection from parents and
society whereas the disadvantaged children such as physically handicapped, mentally handicapped and socially handicapped are neglected by their own nearest and dearest ones as well as society. 7 This negligence adversely affects the psychological as well as oral status. Till now, only a few studies have been conducted to determine the oral health status and dental caries prevalence of handicapped children in India. Therefore the current study was conducted to find out nature and severity of dental problems among handicapped children so that measures can be taken accordingly.
Materials and Methods
This cross-sectional study was planned to assess dental health status of sensory impaired and blind children in an Institute aged 6 to 20 years children. Before the onset of the study, official permission and ethical clearance was obtained from both the Institutes.
Inclusion & Exclusion Criteria
All the children present in the Institutes (Sensory impaired & Blind) during the study period were included in the
study. Children with handicapping conditions other than sensory and visual impaired were excluded. So a total of 310 children were selected which were fulfilling the inclusion criteria.
Questionnaire
A self-administered structured pretested questionnaire which was written in English was used to gather information regarding demographic details. Also WHO assessment 8 form was used to get dentition status of the study population.
Calibration
Examiners were calibrated and validated in the department by doing examination on 20 subjects. The inter examiner reliability was done using Kappa statistics and it was found to be 85% for dft, 88% for DMFT.
Data Analysis
Statistical software namely SPSS 16.0 was used for data analysis. Data was analyzed by student’s t and ANOVA test to find out the statistical significance of the comparisons among children at p≤ 0.05.
Results
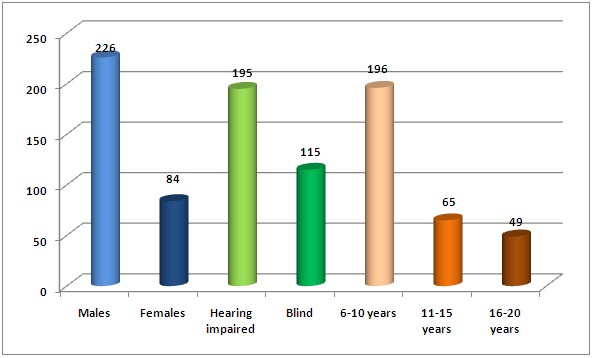
The final study sample was consisted of 310 subjects out of whom 226 were males and 84 females. They were also categorized according to type of disability as 195 were hearing impaired and 115 were blind. According to age groups as 196 belong to age group of 6-10 years, 65 belong to 11-15 years and 49 to 16-20 years ( Graph 1 ).
Graph 1: Showing demographic details of the study population.
The overall mean for DMFT scores for males and females was 2.11 (1.753) and 1.75 (1.275) respectively. Most of the subjects had decayed component followed by missing and filled. Similarly overall mean for dft was 0.31 (0.254) for males and 0.27 (0.143) for females and in those no subject was having filled component. (Table 1)
Table 1: Dental caries prevalence among disabled children according to gender.
| Gender | DT | MT | FT | DFMT | dt | Ft | Dft |
| Male | 1.78 | 0.32 | 0.05 | 2.11 | 0.31 | - | 0.31 |
| (1.023) | (0.533) | (0.024) | (1.753) | (0.254) | (0.254) | ||
| Female | 1.45 | 0.23 | 0.07 | 1.75 | 0.27 | - | 0.27 |
| (0.563) | (0.212) | (0.016) | (1.275) | (0.143) | (0.143) | ||
| p-value | 0.001 | 0.075 | 0.864 | 0.032 | 0.051 | - | 0.054 |
Mean DMFT of blind students was more as compared to hearing impaired ones as 2.16 (2.005) and 1.80 (1.264) respectively. But overall mean of dft scores was more for hearing impaired children 0.33 (0.242) compared to blind children 0.25(0.265) as shown in Table 2.
Table 2: Dental caries prevalence among children according to type of disability.
| Type of disability | DT | MT | FT | DFMT | dt | Ft | dft | |
| Hearing | 1.64 | 0.14 | 0.02 | 1.80 | 0.33 | - | 0.33 | |
| (0.866) | (0.643) | (0.016) | (1.264) | (0.242) | (0.242) | |||
| Blind | 1.92 | 0.18 | 0.06 | 2.16 | 0.25 | - | 0.25 | |
| (1.543) | (0.757) | (0.069) | (2.005) | (0.265) | (0.265) | |||
| p-value | 0.001 | 0.164 | 0.864 | 0.014 | 0.043 | - | 0.045 |
According to age groups there was a significant increase in the mean DMFT scores with advancing age at p ≤ 0.001. Whereas dft mean scores was more among 6 to 10 years age group as compared to older age groups (Table 3).
Table 3: Dental caries prevalence among disabled children according to age .
| Age groups | DT | MT | FT | DFMT | dt | ft | dft |
| 6-10 years | 0.87 | 0.07 | 0.04 | 0.99 | 0.31 | - | 0.31 |
| (1.265) | (0.261) | (0.045) | (1.075) | (0.213) | (0.213) | ||
| 11-15 years | 1.74 | 0.14 | 0.05 | 1.95 | 0.11 | - | 0.11 |
| (1.098) | (0.177) | (0.429) | (1.432) | (0.213) | (0.213) | ||
| 16-20 years | 2.18 | 0.27 | 0.34 | 2.79 | - | - | - |
| (2.643) | (0.184) | (1.896) | (2.346) | ||||
| p-value | 0.001 | 0.03 | 0.644 | 0.001 | 0.03 | - | 0.03 |
Discussion
Children with physical disabilities comes under a group as “special needs population”. 9 They have little about their oral health; also experience considerably higher levels of dental diseases and also more difficulty for accessing oral health care. 10 These disabled subjects need same standards of health care facilities as the general population, but there is evidence that they experience poor oral as well as general health. 11 So, to design proper oral health care for these children with physical disabilities would require data about the dental health status.
In this study mean DMFT and dft scores were found to be 3.86 (2.176) and 0.58 (0.231) respectively. These results were higher than study conducted by Nagaraja Rao in 1985. 12 However in some other studies mean dft was 5.3 for hearing impaired and 3.7 for blind children in Kuwait 13 and the mean DMFT of 5.12 in Saudi Arabia among disabled subjects. 14 These results of caries in handicapped children might be attributed to low level of awareness and negligence of oral hygiene practices.
This deficiency of dental treatment is the main reason that D component of DMFT was 1.64 with impaired hearing and 1.92 among blind subjects. This data is similar to the findings of Jain et al study in Udaipur. 11 It was also found that mean DMFT for blind students was 1.92 (1.543) which was significantly higher than their counterparts 1.64 (0.866) and the results were in contrast to Jain et al study. 11 But Gupta DP et al (1993), have shown more prevalence of dental caries among blind subjects than in deaf and dumb ones. 15 In case of mean dft, hearing-impaired had more mean value than blind subjects.Others mentioned that the mostobvious challenge is the physical inability to adequately clean the oral cavity. 16
DMFT scores were more among male children than females but the findings were in contrast to other studies done by Yee R (2002) 17 and Basil FM in 1989. 18 The DMFT scores significantly increased with advancing age in both the disabled groups and this data is similar to other studies. 2 , 19 Whereas Al-Qahtani observed that blind children of 6-7-year-oldhad caries with a mean dmft of 6.58 and of 11-12-year with a mean DMFT of 3.89.14 Lack of motivation and facilities for regular oral health check-up & treatment also poor socioeconomic status of the parents and cost of treatment are the main factors for the accumulated treatment needs.
Conclusion
Overall mean scores of caries was very high and it increased with increasing age. Blind children experienced more caries then hearing impaired children in permanent, whereas it was opposite in primary dentition. Males had more decayed component than females in all the age groups. So there was high level of unmet needs for dental treatment in this group of children. Dentists should play an important role in improving the dental health of disabled children by early diagnosis and prompt treatment.
Footnotes
Source of Support: Nil
Conflict of Interest: None
Contributor Information
Venkataraam Sanjay, Department of Oral Medicine & Radiology, Coorg Institute of Dental Sciences, Karnataka, India.
Sumanth M Shetty, Department of Pedodontics & Preventive Dentistry, SGT Dental College, Gurgaon, Haryana, India.
Rashmi G Shetty, Department of Conservative Dentistry & Endodontics, SGT Dental College, Gurgaon, Haryana, India.
Noopur A Managoli, Department of Oral & Maxillofacial Pathology, Dr. D. Y. Patil Vidyapeeth, Pune; Dr. D. Y. Patil Dental College & Hospital, Pimpri, Pune, Maharashtra, India.
Sachin C Gugawad, Department of Pedodontics & Preventive Dentistry, School of Dental Sciences Krishna Dental College and Hospital, Karad, Maharashtra, India.
D Hitesh, Kharghar, Mumbai, Maharashtra, India.
References
- 1.M Jain, A Mathur, S Kumar, RJ Dagli, P Duraiswamy, S Kulkarni. Dentition status and treatment needs among children with impaired hearing attending a special school for the deaf and mute in Udaipur, India. J Oral Sci. 2008;50(2):161–165. doi: 10.2334/josnusd.50.161. [DOI] [PubMed] [Google Scholar]
- 2.N Chi, K Yang. A study on the dental disease of the handicapped. J Dent Child. 2003;70:153–158. [PubMed] [Google Scholar]
- 3.C Altun, G Guven, OM Akgun, MD Akkurt, F Basak, E Akbulut. Oral health status of disabled individuals attending special schools. Eur J Dent. 2010;4(4):361–366. [PMC free article] [PubMed] [Google Scholar]
- 4.WE Mouradian. The face of a child: children’s oral health and dental education. J Dent Educ. 2001;65(9):821–831. [PubMed] [Google Scholar]
- 5.J Fiske, DM Davis, C Frances, S Gelbier. The emotional effects of tooth loss in edentulous people. Br Dent J. 1998;184:90–93. doi: 10.1038/sj.bdj.4809551. [DOI] [PubMed] [Google Scholar]
- 6.T Graber. The “three M's”: Muscles, malformation, and malocclusion. Am J Orthod. 1963;49(6):418–450. [Google Scholar]
- 7.J Ainamo, D Barmes, G Beargrie. Development of WHO Community Periodontal Index for treatment needs. Int Dent J. 1982;32:281–291. [PubMed] [Google Scholar]
- 8.Organization World Health. Oral health surveys basic method, 4th ed. Geneva:WHO. 1987:760–871. [Google Scholar]
- 9.H Vignehsa, G Soh, G Lo, N Chellappah. Dental health of disabled children in Singapore. Aust Dent J. 1991;36(2):151–156. doi: 10.1111/j.1834-7819.1991.tb01345.x. [DOI] [PubMed] [Google Scholar]
- 10.A Pradhan, GD Slade, AJ Spencer. Factors influencing caries experience among adults with physical and intellectual disabilities. Community Dent Oral Epidemiol. 2009;37(2):143–154. doi: 10.1111/j.1600-0528.2008.00455.x. [DOI] [PubMed] [Google Scholar]
- 11.M Jain, SP Bharadwaj, LS Kaira, D Chopra, P Duraiswamy, S Kulkarni. Oral Health Status and Treatment Need Among Institutionalised Hearing-Impaired and Blind Children and Young Adults in Udaipur, India - A Comparative Study. Oral Health Dent Manag. 2013;12(1):41–49. [PubMed] [Google Scholar]
- 12.SM Rawlani, G Gupta, M Thadani. Prevalence of dental caries in physically challenged children. J Indian Dent Assoc. 2001;72:154–155. [Google Scholar]
- 13.M Shyama, SA Al-Mutawa, RE Morris, T Sugathan, E Honkala. Dental caries experience of disabled children and young adults in Kuwait. Comm Dent Health. 2001;18(3):181–186. [PubMed] [Google Scholar]
- 14.Z Al-Qahtani, AH Wyne. Caries experience and oral hygiene status of blind, deaf and mentally retarded female children in Riyadh, Saudi Arabia. Odontostomatol Trop. 2004;27(105):37–40. [PubMed] [Google Scholar]
- 15.DP Gupta, KS Roy Chowdury, S Sarkar. Prevalence of dental caries in handicapped children of Calcutta. J Indian Soc Pedo Prev Dent. 1993;11:23–27. [PubMed] [Google Scholar]
- 16.R Johnson, D Albertson. Plaque control for handicapped children. J Am Dent Assoc. 1972;84:824–828. doi: 10.14219/jada.archive.1972.0142. [DOI] [PubMed] [Google Scholar]
- 17.R Yee, N McDonald. Caries experience of 5-6 year old and 12-13 year old school children in central and western Nepal. Int Dent J. 2002;52:453–460. doi: 10.1111/j.1875-595x.2002.tb00642.x. [DOI] [PubMed] [Google Scholar]
- 18.FM Basil, TN Athanassouli. Dental caries prevalence in the permanent teeth in Greek school children related to age, sex urbanization and social status. Community Dent Health. 1989;6:131–137. [PubMed] [Google Scholar]
- 19.K Pieper, B Dirks, P Kessler. Oral hygiene and periodontal disease in handicapped adults. Community Dent Oral Epidemiol. 1986;14:28–30. doi: 10.1111/j.1600-0528.1986.tb01489.x. [DOI] [PubMed] [Google Scholar]