

Abstract
Aim
To determine the efficacy of infliximab in the treatment of chronic refractory pouchitis, following ileo-pouch anal anastomosis (IPAA) for ulcerative colitis (UC).
Methods
Seven patients (4 females, 3 males) with chronic refractory pouchitis were included in an open study. Pouchitis was diagnosed by clinical plus endoscopic and histological criteria. Three patients also had fistulae (pouch-bladder in 1 and perianal in 2). Extraintestinal manifestations were also present in 4 patients (erythema nodosum in 2, arthralgiae in 2). All patients were refractory to standard therapy. Crohn’s disease was carefully excluded in all patients after re-evaluation of the history and examination of the small bowel with enteroclysis or small bowel capsule endoscopy. Patients received Infliximab 5 mg/kg at 0, 2 and 6 weeks and thereafter every 2 months for 1 year. Clinical response was classified as complete, partial, and no response. Fistulae closure was classified as complete, partial, and no closure. The pouchitis disease activity index (PDAI) was also used as an outcome measure.
Results
Clinically, all patients improved. After 1 year of follow-up, 5 of the 7 patients had a complete clinical response, and 2 of the 3 patients with a fistula had complete fistulae closure. At the end of the follow-up period the median PDAI dropped from 11 (baseline) (range, 10-14) to 5 (range, 3-8). Extraintestinal manifestations were in complete remission at the end of the followup period as well.
Conclusions
Our results indicate that infliximab may be recommended for the treatment of chronic refractory pouchitis complicated or not by fistulae following IPAA for UC.
Keywords: Ulcerative colitis, ileal pouch anal anastomosis, chronic refractory pouchitis
Introduction
Despite advances in medical therapy, a substantial number of patients with ulcerative colitis (UC) will require colectomy at some point during the course of their disease. In these cases, proctocolectomy with ileal pouch-anal anastomosis (IPAA) is considered the procedure of choice [1]. Although IPAA retains intestinal continuity and avoids the development of a stoma, it can be associated with troublesome complications, the most common of which is pouchitis [2].
Pouchitis is characterized by increased stool frequency and liquidity, abdominal cramping, urgency, tenesmus and pelvic discomfort. Pouchoscopy and pouch mucosal biopsy are necessary to confirm the diagnosis [3].
On the basis of duration of symptoms pouchitis is divided into acute (< 4 weeks) and chronic (> 4 weeks) [3]. While in patients with acute pouchitis, antibiotic therapy is usually effective, approximately 10-15% of these patients develop chronic pouchitis, refractory to the standard 4-week medical therapy [4]. In the literature, many drugs such as mesalamine, corticosteroids, immunosuppressants and probiotics have been tried for these refractory patients with conflicting or disappointing results [5]. Recently, the administration of infliximab has been tried for the medical management of chronic refractory pouchitis [6-10]; however, literature data are limited.
The aim of this study was to determine the efficacy of infliximab in the treatment of chronic refractory pouchitis, following IPAA for ulcerative colitis.
Methods
This was an open, prospective cohort study, carried out in a referral center for inflammatory bowel disease patients. All patients with pouchitis, followed-up in our Department, were eligible to enter the study. The diagnosis of pouchitis was based on the Pouch Disease Activity Index (PDAI) as confirmed by a combination of clinical, endoscopic and histological criteria. Pouchitis was defined as a total PDAI score ≥ 7 points.
Patients were included if they had chronic refractory pouchitis, defined as no response to at least 4 weeks of standard antibiotic therapy (ciprofloxacin 1 g b.i.d. or metronidazole 500 mg t.d.s.).
Patients were excluded if they had been taking NSAIDs during the last month before screening; had Crohn’s disease, severe cardiovascular, respiratory, hepatic (including primary sclerosing cholangitis) or renal conditions; had a history of or active tuberculosis; had been infected with HIV or HBV/ HCV; were pregnant or breast feeding or had a history of malignancy (including lymphomas).
Crohn’s disease was excluded, using a careful re-evaluation of the patients’ history, including histologic re-evaluation of the surgically excised colonic specimens. In patients in whom doubt remained, wireless capsule endoscopy of the small bowel was done and patients with lesions suggestive of Crohn’s disease were excluded.
In all patients, stool examinations for bacteria and parasites were negative. Infections with shigella, salmonella, toxoplasma, Epstein-Barr virus, cytomegalovirus, Campylobacter and C. difficile were excluded with serological tests and the histology results.
Patients were treated with infusions of infliximab (5 mg/ kg body weight) at 0, 2 and 6 weeks and thereafter, every 2 months for a period of 1 year.
Clinical response was defined at the end of the follow-up period and was classified as complete, partial and no response. Complete clinical response was defined as cessation of diarrhea, urgency, incontinence, blood loss and abdominal pain. A partial clinical response was defined as a marked clinical improvement, but with persisting symptoms. All other outcomes were defined as no response.
Similarly, in patients with fistula, response was categorized as complete, partial, or no response. A complete fistula response was defined as cessation of fistula drainage, while partial fistula response was defined as reduction in drainage. All other outcomes were categorized as no fistula response.
For all patients the PDAI was again calculated at the end of the follow-up period, 1 year after the initiation of the infliximab administration.
The study was performed in accordance with the Declaration of Helsinki and all patients gave written informed consent.
Statistical analysis was performed using SPSS 15.0 (SPSS, Chicago, IL) and comparisons for patients were made using chi-square statistics, Fisher’s exact test and Mann-Whitney U-tests. The threshold for statistical significance was predefined as p<0.05.
Results
From December 2007 till December 2010, a total of 9 patients with chronic refractory pouchitis were seen at our Department and were considered for entry into the study. The total number of patients with ulcerative colitis undergoing proctocolectomy with IPAA in our hospital during the study period and the sort of pouch that was performed is not reported, since no precise data are available from the relevant surgical departments. The mean time interval between surgery and onset of pouchitis was 4.6 months (range 2-14 months). Of these patients, one had apthous ulcerations in the small bowel as seen in capsule endoscopy and was therefore excluded, since Crohn’s disease could not be ruled out; while another patient had a history of cardiac failure and was excluded as well. Seven patients (4 females, 3 males) fulfilled all inclusion and exclusion criteria and were finally included in the study.
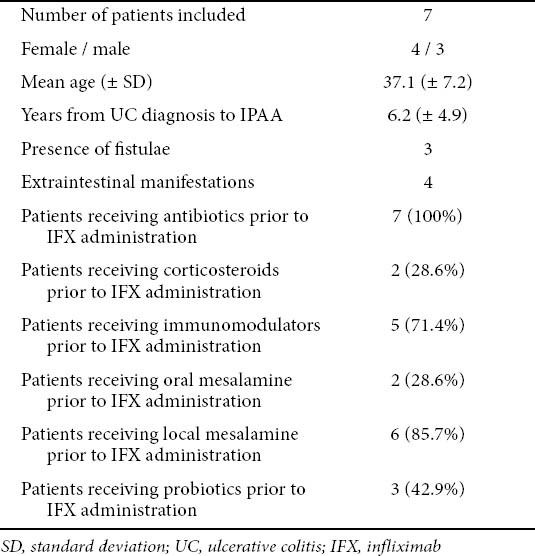
Of those 7 patients, 3 also had fistulae (pouch-bladder in 1 and perianal in 2). Extraintestinal manifestations were also present in 4 patients (erythema nodosum in 2, arthralgiae in 2). All patients were refractory to antibiotics, while 5 patients were refractory to azathioprine and 2 to corticosteroids as well. Two patients had received oral mesalamine, 6 local mesalamine and 3 probiotics with no favorable results. The only combination therapy that patients received was antibiotic therapy plus azathioprine or corticosteroids. No patient received azathioprine and corticosteroids concurrently. Mesalamine and or probiotic therapy was combined with antibiotic and/or azathioprine: corticosteroid therapy. The main patient characteristics, together with the medications they were receiving prior to infliximab administration are listed in Table 1.
Table 1.
Patient characteristics
At the end of the follow-up period all patients improved clinically. After 1 year of infliximab administration, 5 of 7 patients (71.4%) had a complete clinical response, 1 patient had partial response (14.3%) and one other (14.3%) had no response. As regards patients with fistulae, 2 out of the 3 (66.7%) patients had a complete fistulae closure (complete fistulae response), while the third patient had a partial fistulae response. Extraintestinal manifestations were in complete remission at the end of the follow-up period in all patients. At the end of the follow-up period the median PDAI dropped from 11 (baseline) (range, 1014) to 5 (range, 3-8).
There were no major complications noted from the infliximab administration, apart from a slight rash seen in one of our patients. The rash appeared at the beginning of the second infusion and disappeared after reduction in the flow.
Discussion
The results of this open, single-center study indicate that one-year infliximab administration resulted in a complete clinical response in 71.4% of patients with chronic refractory pouchitis, while another 14.3% of the study population experienced a partial response. Complete fistulae closure was noted in 66.7% of the patients studied, whereas the remaining patients experienced partial fistulae response.
Patients with chronic refractory pouchitis, with or without fistulae form a group difficult to treat. There are limited data suggesting which therapy should be administered in these patients when antibiotic therapy fails. Corticosteroids, mesalamine, immunomodulators and probiotics have all been tried in clinical trials with either conflicting or disappointing results [5]. Since there have been data showing TNF-a to be elevated in mucosal biopsies of inflamed pouches, the administration of anti-TNF therapy in patients with chronic refractory pouchitis has gained interest in the literature.
Viscido et al [6] reported the efficacy of infliximab in a group of 7 patients with chronic refractory pouchitis complicated by a pouch fistula. After 10 weeks of therapy, 6 patients had a complete clinical response, while 5 also had a complete fistula response.
Colombel et al [7] reviewed the medical records of 26 patients with fistulizing disease of the pouch and/or prepouch ileitis and showed that infliximab administration resulted in 50% complete short-term fistula response.
In a third trial by Calabrese et al [8], 10 patients with refractory pouchitis complicated by ileitis received an induction scheme with infliximab and were evaluated at week 10. Clinical remission was achieved in 9 of the 10 enrolled patients.
More recently, Shen et al [9] reported the efficacy of adalimumab in patients with Crohn’s disease related complications of the pouch. At week 4, 41% of the patients had a complete clinical response, while 35.3% had a partial response.
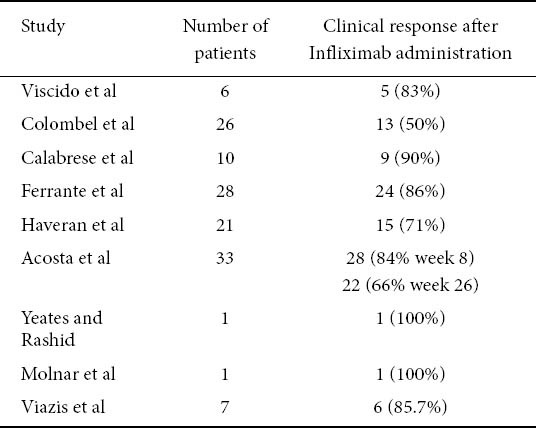
One of the largest series so far has been published in 2010, by Ferrante et al [10]. In their retrospective study 28 patients with pouchitis and/or pre-pouch ileitis and/ or pouch fistula were included. At week 10 following the onset of infliximab administration, 88% of patients with refractory luminal inflammation showed clinical response, while 86% of patients showed fistula response. After a median follow up of 20 months, 56% showed sustained clinical response, while 42.9% showed sustained fistula response. Finally, there have been two more reports and two case reports with favorable results as noted in Table 2 [11-14].
Table 2.
Summary of literature data
One of the strengths of our study is the fact that every effort has been made to exclude patients with possible Crohn’s disease. For some clinicians, the development of complications such as prepouch ileitis is a sufficient reason to change the diagnosis from ulcerative colitis to Crohn’s disease. That is the reason why all the patients included in our study underwent a wireless capsule endoscopy if the diagnosis was in doubt and they were excluded if lesions in the small bowel were noted. Of course there are limitations to our study as well, since it was an open study in which only 7 patients where finally included. It is true that a prospective multicenter randomized controlled trial is needed; however, such a study is difficult to conduct. In the meantime, the results of our study, together with those of the literature indicate a beneficial role for infliximab in the treatment of patients with chronic refractory pouchitis, although medication had to be discharged in some patients.
In conclusion, one-year infliximab administration can be recommended for the treatment of chronic refractory pouchitis, with or without fistula, following an IPAA for ulcerative colitis.
Summary Box.
What is already known:
Pouchitis is a common problem in patients with proctocolectomy with ileal pouch-anal anastomosis (IPAA)
10-15% of patients with pouchitis develop chronic pouchitis, refractory to the standard 4 week medical therapy; therefore, management of these patients is difficult
What the new findings are:
After 1 year of infliximab administration, 71.4% of the patients included in the study had a complete clinical response
As regards patients with fistulae, 66.7% of them had a complete fistulae closure
One-year infliximab administration can be recommended for the treatment of chronic refractory pouchitis, with or without fistula, following an IPAA for ulcerative colitis
Biography
Evangelismos Hospital, Athens, Greece
Footnotes
Conflict of Interest: None
References
- 1.Melville D, Ritchie J, Nicholls R, et al. Surgery for ulcerative colitis in the era of the pouch: the St Mark's Hospital experience. Gut. 1994;35:1076–1080. doi: 10.1136/gut.35.8.1076. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Fazio V, Ziv Y, Church J, et al. Ileal pouch-anal anastomoses complications and function in 1005 patients. Ann Surg. 1995;222:120–127. doi: 10.1097/00000658-199508000-00003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Biancone L, Michetti P, Travis S, et al. for the European Crohn's and Colitis Organisation (ECCO) European evidence-based Consensus on the management of ulcerative colitis: Special situations. J Crohns Colitis. 2008;2:63–92. doi: 10.1016/j.crohns.2007.12.001. [DOI] [PubMed] [Google Scholar]
- 4.Ferrante M, Declerck S, De Hertogh G, et al. Outcome after proctocolectomy with ileal pouch-anal anastomosis for ulcerative colitis. Inflamm Bowel Dis. 2008;14:20–28. doi: 10.1002/ibd.20278. [DOI] [PubMed] [Google Scholar]
- 5.Sandborn W, Pardi D. Clinical management of pouchitis. Gastroenterology. 2004;127:1809–1814. doi: 10.1053/j.gastro.2004.10.011. [DOI] [PubMed] [Google Scholar]
- 6.Viscido A, Habib F, Kohn A, et al. Infliximab in refractory pouchitis complicated by fistulae, following ileo-anal pouch for ulcerative colitis. Aliment Pharamcol Ther. 2003;17:1263–1271. doi: 10.1046/j.1365-2036.2003.01535.x. [DOI] [PubMed] [Google Scholar]
- 7.Colombel J, Ricart E, Loftus V, et al. Management of Crohn's disease of the ileoanal pouch with infliximab. Am J Gastroenterol. 2003;98:2239–2244. doi: 10.1111/j.1572-0241.2003.07675.x. [DOI] [PubMed] [Google Scholar]
- 8.Calabrese C, Gionchetti P, Rizzello F, et al. Short term treatment with infliximab in chronic refractory pouchitis and ileitis. Aliment Pharmacol Ther. 2008;27:759–764. doi: 10.1111/j.1365-2036.2008.03656.x. [DOI] [PubMed] [Google Scholar]
- 9.Shen B, Remzi F, Lavery I, et al. Administration of adalimumab in the treatment of Crohn's disease of the ielal pouch. Aliment Pharmacol Ther. 2009;29:519–526. doi: 10.1111/j.1365-2036.2008.03920.x. [DOI] [PubMed] [Google Scholar]
- 10.Ferrante M, D’Haens G, Dewit O, et al. Efficacy of infliximab in refractory pouchitis and Crohn's disease-related complications of the pouch: A Belgian case series. Inflamm Bowel Dis. 2010;16:243–249. doi: 10.1002/ibd.21037. [DOI] [PubMed] [Google Scholar]
- 11.Haveran LA, Sehgal R, Poritz LS, McKenna KJ, Stewart DB, Koltun WA. Infliximab and/or azathioprine in the treatment of Crohn's disease-like complications after IPAA. Dis Colon Rectum. 2011;54:15–20. doi: 10.1007/DCR.0b013e3181fc9f04. [DOI] [PubMed] [Google Scholar]
- 12.Acosta MB, Garcia-Bosch O, Souto R, et al. Efficacy of infliximab rescue therapy in patients with chronic refractory pouchitis: a multicenter study. jInflamm Bowel Dis. 2011 doi: 10.1002/ibd.21821. in press. [DOI] [PubMed] [Google Scholar]
- 13.Yeates J, Rashid M. Successful long-term use of infliximab in refractory pouchitis in an adolescent. Gastroenterol Res Pract 2010. 2010:860394. doi: 10.1155/2010/860394. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Molnar T, Farkas K, Nagy F, Wittmann T. Successful use of infliximab for treating fistulizing pouchitis with severe extraintestinal manifestation: a case report. Inflamm Bowel Dis. 2008;14:1752–1753. doi: 10.1002/ibd.20485. [DOI] [PubMed] [Google Scholar]