

Abstract
Background
Reliable models for massive hepatectomy in the mouse are required for experimental liver research.
Methods
We analyzed anatomical findings in 100 mice following massive hepatectomy induced by liver reduction >70%. The impact of various factors in the different models was also analyzed, including learning curves, operative time, survival curves and histopathological findings.
Results
According to anatomical results, murine models with 75%, 80% and 90% of liver resection produced massive hepatectomy. Learning curves and operative times were most optimal with the clip technique. Each hepatectomy performed using the clip technique produced a reasonable survival curve, and there were no differences in histopathological findings between the suture and clip techniques.
Conclusion
Massive hepatectomy by the clip technique is simple and can provide reliable and relevant data.
Keywords: Hepatectomy, animal model, clip, mouse, microsurgery, surgical technique
Introduction
New insights into mechanisms in the hepatology field have been established from experimental animal models. The rodent hepatectomy model is mainly employed to examine liver regeneration, liver failure and tumor metastasis. The 70% hepatectomy by en bloc ligation of the lobes is well established in the rat [1,2]. However, mouse models allow for the use of gene-altered or knockout strains and for laboratory assays because of the development of specific agents and antibodies [3]. At present there are a number of murine hepatectomy models [4-10], of which the 70% hepatectomy (termed 2/3 partial hepatectomy) is the most common. Introduction of microsurgical techniques has also enabled high rates of successful surgery, especially in individualized dissection and ligation of vessels [6,11,12]. However, murine hepatectomy remains challenging because of the delicate nature of the liver, the lack of intravenous access and the risk of hemorrhage [9], resulting in high rates of mortality and morbidity [5,13].
Despite the widespread use of the 70% hepatectomy [4-7], alternative hepatectomy models with resected volumes >70% are required to provide more clinically relevant experiments on liver regeneration and hepatic failure. Nikfarjam et al reported the benefits of the hemostatic clip in 37% and 70% hepatectomy models in the mouse [5]. Furthermore, we have performed thousands of massive hepatectomy procedures using the clip technique at our institution. Herein, we investigated the segmental volume in the murine liver, and describe detailed surgical procedures of our innovative hepatectomy model in the mouse. To the best of our knowledge, this is the first report of the benefits of hemostatic clip for massive hepatectomy model in the mouse.
Materials and Methods
Animals
Inbred C57BL/6 mice (male, 10-20 weeks of age, approximately 25 g body weight) were used (C57BL/6NHsd; Harlan Laboratories, Indianapolis, IN 46250, USA). All mice were maintained under specific pathogen-free conditions. Mice were kept well hydrated prior to surgery because subtle dehydration can easily result in death during anesthesia and surgery. All experimental protocols were approved by the ethical committees of the Mayo Clinic (Protocol No. IACUC 33307 and 24907). Animal handling and care met the requirements of our institutional guidelines for animal welfare.
Electrocautery scalpels
Bipolar forceps (Martin ME 102 Electrosurgical unit and Bipolar Accessory Set for ME 102; Harvard Apparatus, Holliston, MA 01746, USA) were used as a conventional scalpel. Fine-tipped and delicate scalpels were prepared separately for microsurgery and ultra-microsurgery. We used a monopolar type (Bovie, low temperature cautery kit; Aaron Medical, Clearwater, FL 33710, USA).
Microscopes
We used a surgical microscope at 5-10× magnification (Surgical Scope M680, Type 10445496; Leica Microsystems Inc., Bannockburn, IL 60015, USA). Even though a high magnification (12.5-20× magnification) was not required, a sufficient light source was indispensable.
Surgical threads for hepatectomy by suture technique
We used monofilament polypropylene sutures (MPS) (7-0 Prolene, BV-1, 8304H-X, or 8-0 Prolene, BV130-5, 8732H; Ethicon, Inc., Somerville, NJ 08876-0151, USA), for suture of the hepatic surface. Monofilament nylon suture (10-0 Ethilon, BV130-3, 2820G; Ethicon, Inc.) was used for additional suture for well-focused hemostasis.
Hemostatic clip for hepatectomy by clip technique
Hemostatic clips were prepared in several sizes (Microclip size: M, ML and L; Horizon Ligation System; Teleflex Medical, Durham, NC 27709, USA) (Fig. 1A). Several sizes of applying forceps (Microclip applicators; Teleflex Medical) were also prepared.
Figure 1.
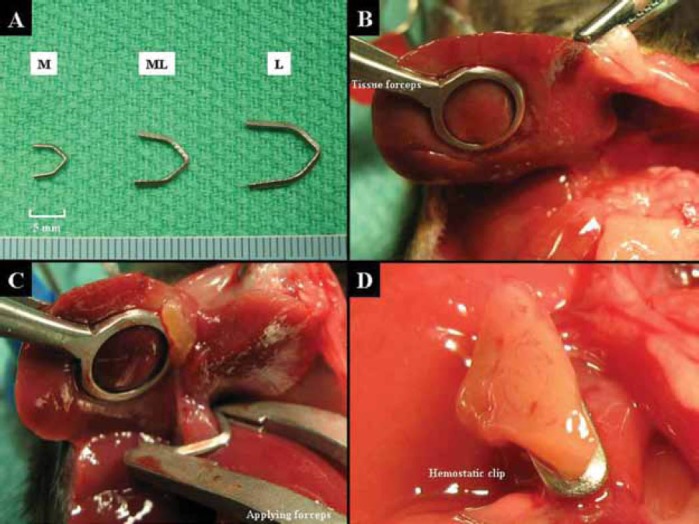
Hemostatic clip and hepatectomy by clip technique. A. Hemostatic clips are prepared in several sizes (M, ML and L). B. The hepatic segment is retracted using tissue forceps when the clip is applied. C. We mainly use an M-sized or ML-sized clip. The clip is applied at a point near to the divide of each segment, and the PHM is approximately 1 mm from a segmental divide. D. The relevant segment is cut with a 3-5 mm of DHM.
PHM, proximal hepatic margin; DHM, distal hepatic margin; M, medium; ML, medium large; L, large.
Anatomy
The liver is divided into three lobes (right, left, and caudate lobes) arranged into six segments: right anterior segment (RAS), right middle segment (RMS), right posterior segment (RPS), left anterior segment (LAS), left posterior segment (LPS) and omental segment (OS) (Fig. 2A) (4-6). We measure the weight of each segment in a total of 100 mice, and segmental percentages were calculated as segmental weight (g)/whole liver weight (g) in each mouse. Of note, the murine gallbladder (GB) can be easily detected between the RAS and the LAS (Fig. 2B), while the rat does not have a GB.
Figure 2.
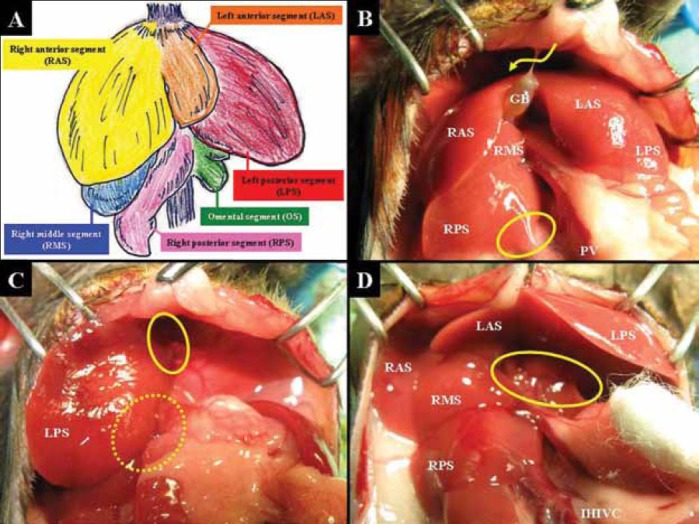
Hepatic segments and transparent membranes. A. The murine liver is divided into six segments (RAS, RMS, RPS, LAS, LPS and OS). B. GB is detected between the RAS and LAS. The falciform ligament is located near the GB. The falciform and triangular ligaments are sharply cut to the surface level of the supra-hepatic inferior vena cava (arrow). The IHIVC should be skeletonized from the RPS (circle). C. The thin and transparent membranes that fix LPS to diaphragm (solid circle) and the OS (dotted circle) are sharply cut. D. The membrane that fixes the LAS and LPS to the hepatic hilum and gastroduodenal tract is sharply cut.
RAS, right anterior segment; RMS, right middle segment; RPS, right posterior segment; LAS, left anterior segment; LPS, left posterior segment; OS, omental segment; GB, gallbladder; IHIVC, infrahepatic inferior vena cava.
Anesthesia
General anesthesia was performed using a commercial anesthesia system (VetEquip Inc., Pleasanton, CA 945880785, USA), including an evacuation canister (f/air; Bickford Inc., New York, NY 14169, USA) and induction chamber (2-Liter Induction Chamber; VetEquip Inc.). All operative procedures are performed under general anesthesia using isoflurane (Isoflurane USP, 250ml; Webster Veterinary, Sterling, MA 01564, USA) with oxygen, and inhalational anesthesia is induced and maintained by isoflurane using an anesthesia system. A sufficient depth of anesthesia is required for microsurgical procedures. Isoflurane with oxygen flow at 5 L/min is used in the introduction phase, and is reduced to 0.5-2.0 L/min in the maintenance phase. Body weight is measured after anesthesia. The abdominal wall is shaven using electric clippers, and all feet of each mouse are fixed to the operating table by pins. The body position is adjusted to obtain optimal surgical field.
Laparotomy
The abdominal wall is sterilized using a surgical scrub including povidone iodine. Any liver damage should be avoided during laparotomy. A transverse incision is performed and complete homeostasis is obtained using an electrocautery scalpel. An adequate surgical field is achieved using retractors for optimal retention of the bilateral costal bows and the fixation forceps to pull the lower abdominal wall. Note that the transverse incision, which is too close to the costal bow, will disturb cardiac and respiratory function because retraction is performed during surgery.
We prepare isotonic normal saline (0.9% Sodium Chloride Injection USP; Hospira Inc., Lake Forest, IL 60045, USA), and warm saline is arbitrarily dripped onto the intraperitoneal organs to prevent drying after laparotomy. The gastrointestinal tract is moistened with warm saline and positioned to the outside of the left abdominal cavity and coated with gauze. The liver must be handled delicately by blunt and soft materials such as a cotton swab (Cotton tipped applicators; Hardwood Products Company, Guilford, ME 04443-0149, USA), and the liver must not be touched directly during surgery to avoid unexpected injury. A delicate subtraction using wet gauze works well to temporarily move organs to one side of the surgical field. Mice received only laparotomy (Control group) in this study.
Mobilization of each segment
The membranes and ligaments that fix each lobe to the surrounding organs are all thin and transparent. The falciform ligament is located near the GB. Recognition of the relationship between the hepatic segment and the inferior vena cava (IVC) is important. The falciform and triangular ligaments are sharply cut to the surface level of the supra-hepatic IVC (SHIVC). The hepatic IVC (HIVC) runs into the RMS and the RPS. The retroperitoneum on the infra-hepatic IVC (IHIVC) is dissected, and the IHIVC should be skeletonized enough from the RPS (Fig. 2B). The LPS is fixed to the diaphragm and the OS by membranes. Each membrane is cut sharply (Fig. 2C).
The portal vein (PV), pulsating hepatic artery (HA) and common bile duct can be detected under a microscopic surgical field. The membrane that fixes the LAS and the LPS to the hepatic hilum and gastroduodenal tract is sharply cut (Fig. 2D). Thus, the membranes and ligaments around the liver that fix each lobe to the surrounding organs are cut under careful retention of liver, resulting in mobilization of liver.
Hepatectomy by suture technique
In our institution, we never perform temporal clump of the PV and/or the HA during hepatectomy. Hepatectomy by suture technique requires a proximal hepatic margin (PHM) for suture bait. An atraumatic clamp (Micro Vascular Clip, RS-6470 or RS-6472; Roboz Surgical Instrument Co., Gaithersburg, MD 20898-0710, USA) is placed on the hepatic segment, and the optimal PHM is 2-3 mm from the division of each segment. The clamped segment is sharply cut with a 1 mm distal hepatic margin (DHM) (Fig. 3A).
Figure 3.
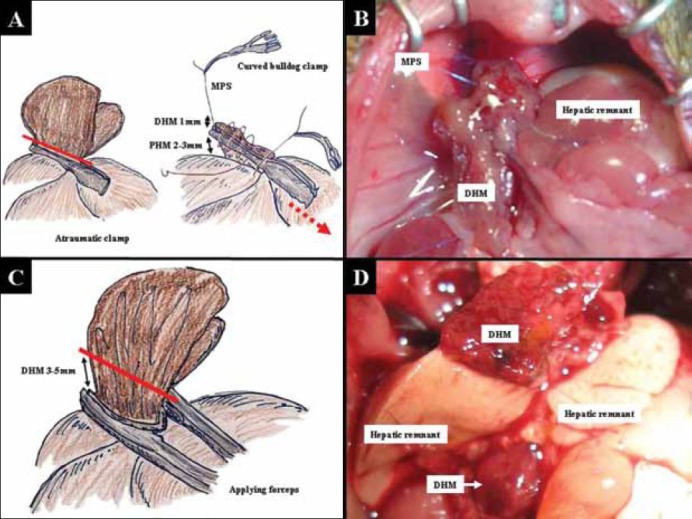
Hepatectomy by suture and clip techniques. A. An atraumatic clamp is placed on the hepatic segment, with an optimal PHM of 2-3 mm from a divide of each segment. The clamped segment is sharply cut with 1 mm of DHM (red line). Sutures that do not involve the clamp are placed bilaterally. These bilateral sutures are ligated, and each suture is grasped with a curved bulldog clamp. By using the suture of the left-side ligation, the cut surface of the liver is sutured from the left side to the right side. The liver is sutured with a loose continuous suture that involves a clamp, and the last suture reaches the right side. B. The clamp is removed (dotted red arrow) and the hepatic margin is immediately treated by tightening the continuous suture. The thread of the tightened continuous suture is ligated with the stay suture of the right side without over-tightening. A continuous suture is made from the right side to the left side. The last suture is ligated with the stay suture of the left side without over-tightening. C. The relevant segment is cut with a 3-5 mm of DHM (red line). D. Ischemic change of DHM at 24 h after 80% hepatectomy is shown. Although the liver remnants after massive hepatectomy showed color change due to vacuolization, DHM clearly showed necrotic changes. Color change between liver remnant and DHM was more enhanced at autopsy.
PHM, proximal hepatic margin; DHM, distal hepatic margin.
Sutures that are not involved in clamping are placed bilaterally. These bilateral sutures are ligated, and each suture is grasped with a curved bulldog clamp (Cooley Bulldog clamps, curved, serrated, MB586R or MB587R; V. Mueller, Aesculap Inc., Center Valley, PA 18034, USA). Under bilateral retention using the stay sutures, the cutting segment is set in an adequate position. By using the suture of the left-side ligation, the cut surface of the liver is sutured from the left side to the right side. The liver is sutured by a loose continuous suture that initially involves the clamp, and the last suture reaches the right side. The clamp is removed and the hepatic margin is immediately treated with a tightened continuous suture. The thread of the tightened continuous suture is ligated with the stay suture of the right side without over-tightening.
A continuous suture is made from the right side to the left side. The last suture is ligated with the stay suture of the left side without over-tightening (Fig. 3B). The presence of bleeding points should be carefully checked using a cotton swab. Additional suture is made with a monofilament nylon suture for well-focused hemostasis if required. A cotton-like regional haemostatic agent (microfibrillar collagen, Avitene; C.R. Bard, Inc., Murray Hill, NJ 07974, USA) can also be used to stop oozing. Any coagula are removed by gauze, and the intra-peritoneal cavity is cleaned.
Hepatectomy by hemostatic clip technique
In our institution, we never perform temporal clamp of PV and/or HA during hepatectomy. Clip application is performed under a limited direction. Therefore, the hepatic segment is retracted using tissue forceps when the clip is applied (Fig. 1B). We cut each segment separately, and mainly used M-sized clips for hepatectomy in the manner of one clip to one segment. Only RAS and LAS are often treated together, using an ML-sized clip (Fig. 1C and 3C). We usually do not use an L-sized clip, except for an unexpected rare anomaly.
A key step in this clip method is the hepatic margin. The clip is applied near the point of division of each segment (Fig. 1C), and the PHM is approximately 1 mm from a segmental division. On the other hand, a relevant segment is cut with a 3-5 mm of DHM (Fig. 1D and 3C). The cut surface is carefully checked. Additional suture for complete hemostasis is not typically required. The intra-peritoneal cavity is cleaned by gauze. Even during surgery, color change of the clipped segment due to ischemia is confirmed, and color change between the liver remnant and DHM was more enhanced at autopsy (Fig. 3D).
Abdominal closure
The intraperitoneal cavity and organs are washed with warm saline. The peritoneum and fascia are closed with a continuous suture using absorbable thread (5-0 Coated Vicryl Plus; Ethicon, Inc.). The skin layer is closed separately using the same method.
Post-operative care and estimation of animal condition
A warmer (RightTemp, RTHS-SM; Kent Scientific Co., Torrington, CT 06790, USA) was used to maintain body temperature immediately after surgery, and a heating pad (E12107; Sunbeam, Gainesville, FL, 32608-1604, USA) was used to warm the cage until mice completely recovered from anesthesia and surgery. Postoperative observation was performed every 2 h until the first 12 h after surgery, and thereafter every 4 h. An analgesic agent (0.1 µg/g body weight, i.m.; buprenorphine 100 µg/Ml; Cerilliant, Round Rock, TX 78655) was routinely given intramuscularly every 12 h until 5 days after surgery.
Antibiotics (30 µg/g body weight, i.p.; Cephalexin Hydrate; MP Biomedicals, Cleveland, OH 44139, USA) are administered every 12 h, from 0-24 h after surgery. For each mouse, 1 mL of lactate Ringer’s solution (Lactated Ringer’s Injection USP; B. Braun Medical Inc., Irvine, CA 92614-5895, USA) was routinely administered every 6 h, from 0-24 h after surgery. A total of 0.5 mL of this solution was injected intravenously via the tail vein using a 31 gauge fine needle, if required.
Learning curves and operative time
The learning curve for surgery is important for reliability of the massive hepatectomy model. To compare hepatectomy using the suture technique versus the clip technique, we examined learning curves and operative time at our institutions. Learning curves were investigated in one surgeon without any experience of massive hepatectomy in the mouse. For each technique, ten cases were set as one unit for training. The required units that showed no differences in survival curves after massive hepatectomy with those at the next unit were analyzed. The survival curves of massive hepatectomy after the training period were compared between two techniques. Operative time data were also collected from experienced surgeons in 20 cases for each technique.
Survival curves after massive hepatectomy by clip technique
Survival curves after massive hepatectomy and laparotomy only from experienced surgeons were investigated. Because more close observation is required for reliable survival curves, we intensively observed mice every 2-4 h even after 12 h post-surgery.
Histopathological findings of liver remnant near the PHM and DHM in massive hepatectomy by the clip technique
In the clip technique, it has been proposed that the clip may secondarily obstruct the outflow of biliary ducts near the PHM or hepatic remnant. To determine this, we investigated histopathological findings of a clip-touched hepatic remnant near the PHM and the DHM.
Focal and/or patchy necrosis after massive hepatectomy
Focal and/or patchy necrosis is an important histopathological finding after hepatectomy [4]. To calculate the rate of appearance of focal and/or patchy necrosis in hepatectomy by the suture and clip techniques, we examined ten cases for each technique. Histopathological analyses were performed at 6 h after massive hepatectomy. These sets were repeated three times for each technique.
Statistical analysis
Data are presented as mean ± standard deviation. Univariate and multivariate analyses were used for the between-group comparisons as follows: Student’s t test for unpaired variables between two groups and Kaplan-Meier method (the log-rank) for survival rates. Statistical calculations were performed using StatView Version 5.0 (SAS, Cary, NC 27513-2414, USA). A p value < 0.05 was considered statistically significant.
Results
Hepatic volumes of each segment
The percentages of total volume for each of the segments were 21.2±3.3% for RAS, 11.5±2.1% for RMS, 14.8±4.0% for RPS, 11.9±1.7% for LAS, 31.6±3.6% for LPS and 9.0±1.6% for OS (Fig. 4A).
Figure 4.
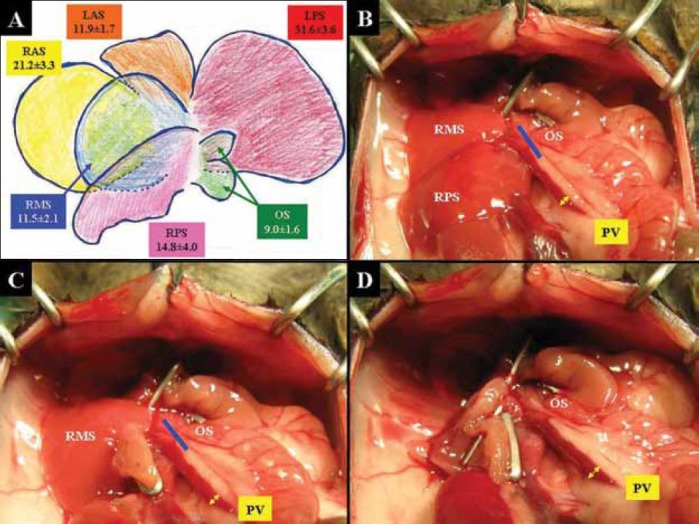
Hepatic volume of each segment and massive hepatectomy models. A. The percentages of total volume of each segment were 21.2±3.3% for RAS, 11.5±2.1% for RMS, 14.8±4.0% for RPS, 11.9±1.7% for LAS, 31.6±3.6% for LPS and 9.0±1.6% for OS. B. Traditional 2/3 hepatectomy of RMS+RPS+OS (35.4±4.0%) is shown. Additional resection of OS (blue line) will make a 75% hepatectomy (RMS+RPS, 26.4±3.8 %). C. Hepatic remnant in 80% hepatectomy was RMS+OS (20.6± 2.6%). Additional resection of OS (blue line) will make an RMS-remnant 90% hepatectomy (RMS, 14.8±4.0%). D. OS-remnant 90% hepatectomy is shown (OS, 9.0±1.6%). Dilation of the PV due to portal hypertension is confirmed, in reverse proportion to the volume of hepatic remnant (yellow arrows in B-D).
RAS, right anterior segment; RMS, right middle segment; RPS, right posterior segment; LAS, left anterior segment; LPS, left posterior segment; OS, omental segment.
Massive hepatectomy models in the mouse
Hepatic remnant in the 75% hepatectomy was RMS+RPS (26.4±3.8%), while for traditional 2/3 hepatectomy, this value was RMS+RPS+OS (35.4±4.0%) (Fig. 4B). Hepatic remnant in the 80% hepatectomy was RMS+OS (20.6±2.6%) (Fig. 4C). We had two surgical options for 90% hepatectomy, and the hepatic remnant in the 90% hepatectomy was chosen from the OS (9.0±1.6%) (Fig. 4D) or the RMS (11.5±2.1%). Dilation of the PV due to portal hypertension was confirmed, in reverse proportion to the volume of the hepatic remnant (Fig. 4B-3D).
Learning curves
Survival curves of each 10 cases at early term in training in the 80% hepatectomy by the suture technique are shown in Fig. 5A. The p values between the first 10 cases and the second 10 cases, between the second 10 cases and the third 10 cases, between the third 10 cases and the fourth 10 cases and between the fourth 10 cases and the fifth 10 cases were 0445, 0.0471, 0.4790 and 0.8941, respectively. Survival curves of each 10 cases at early term in training in the 80% hepatectomy by the clip technique are shown in Fig. 5B. The p values between the first 10 cases and the second 10 cases, between the second 10 cases and the third 10 cases, between the third 10 cases and the fourth 10 cases and between the fourth 10 cases and the fifth 10 cases were 0.0363, 0.6854, 0.9127 and 0.9007, respectively.
Figure 5.
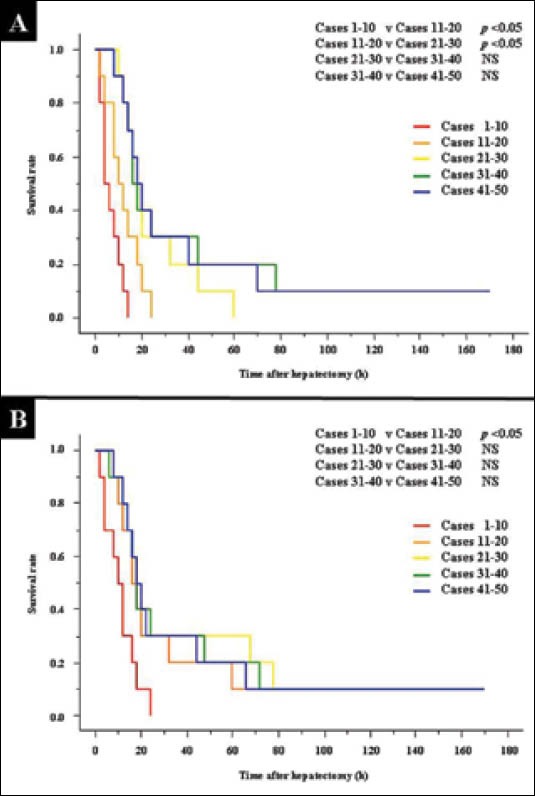
Learning curves for massive hepatectomy in the suture and clip techniques. A. In 80% hepatectomy by the suture technique, survival curves of each 10 cases at early term in training are shown. The p values between the first 10 cases and the second 10 cases, between the second 10 cases and the third 10 cases, between the third 10 cases and the fourth 10 cases and between the fourth 10 cases and the fifth 10 cases were 0445, 0.0471, 0.4790 and 0.8941, respectively. B. In 80% hepatectomy by the clip technique, survival curves of each 10 cases at early term in training are shown. The p values between the first 10 cases and the second 10 cases, between the second 10 cases and the third 10 cases, between the third 10 cases and the fourth 10 cases and between the fourth 10 cases and the fifth 10 cases were 0.0363, 0.6854, 0.9127 and 0.9007, respectively.
NS, not significant
In the 80% hepatectomy, the fifth 10 cases (i.e., 10 cases after the experience of 40 cases) in the suture technique and the fourth 10 cases (i.e., 10 cases after the experience of 30 cases) in the clip technique showed similar survival curves (p = 0.8516) (Fig. 6A) even though 30 cases in the suture technique and 20 cases in the clip techniques seemed to be enough statistically. Our institution has similar results in a 90% hepatectomy model.
Figure 6.
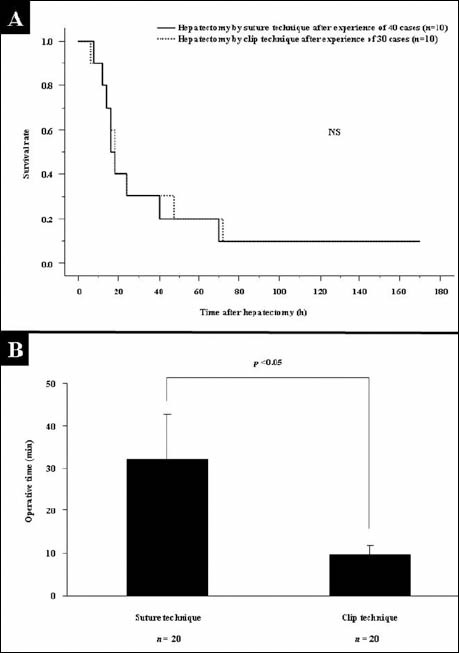
Survival curves and operative times in massive hepatectomy after initial training. A. In 80% hepatectomy, the fifth 10 cases (i.e., 10 cases after experience of 40 cases) by the suture technique and the fourth 10 cases (i.e., 10 cases after experience of 30 cases) by the clip technique showed similar survival curves (p = 0.8516). B. In each technique, the operative time was investigated in 20 cases of 80% hepatectomy. These data were corrected by experienced surgeons. Operative times of 80% hepatectomy by the suture and clip techniques were significantly different (p <0.0001).
Operative time
Even in experienced surgeons, operative times for hepatectomy using the suture technique and the clip technique were significantly different (p <0.0001) (Fig. 6B). Operative time was clearly shortened in the clip techniques.
Survival curves after massive hepatectomy by each technique
In massive hepatectomy, actual survival curves of each hepatectomy are shown in Fig. 7A and 7B. Twenty cases were followed for each of the following conditions. In the 90% hepatectomy, two types of hepatectomy were available; OS-remnant 90% hepatectomy (Fig. 4C) and RMS-remnant 90% hepatectomy (Fig. 4D). Ten cases were followed in each of the 90% hepatectomy models by the suture technique, and there were no significant differences in survival curves between the OS-remnant and the RMS-remnant (p = 0.3784) (Fig. 7C). Ten cases were followed in each of the 90% hepatectomy models by the clip technique, and there were no significant differences in survival curves between the OS-remnant and the RMS-remnant (p = 0.3588) (Fig. 7D).
Figure 7.
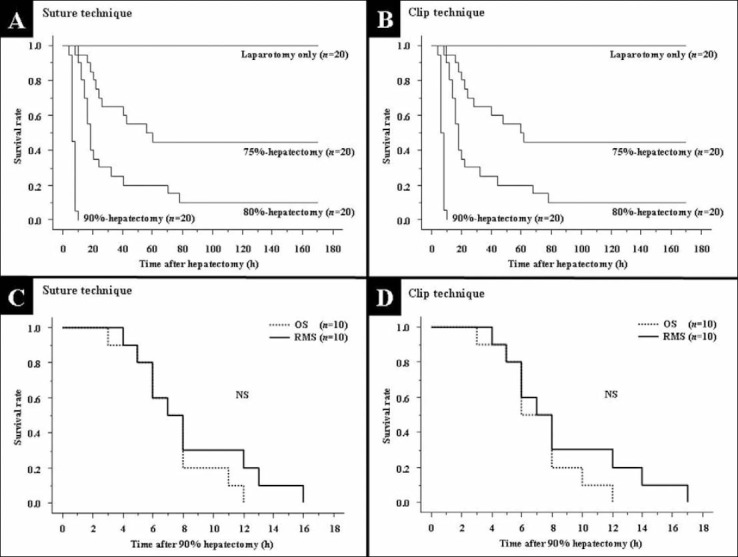
Actual survival curves after massive hepatectomy. A. Actual survival curves of each hepatectomy by suture technique are shown. In each hepatectomy, twenty cases were observed. B. Actual survival curves of each hepatectomy by clip technique are shown. In each hepatectomy, twenty cases were observed. C. A total of 9.0±1.6% of the liver remains in OS-remnant 90% hepatectomy. A total of 11.5±2.1% of liver remains in the RMS-remnant 90% hepatectomy. There were no differences in survival curves after 90% hepatectomy by clip technique between the OS-remnant (n=10) and the RMS-remnant (n=10) (p = 0.3784). D. A total of 9.0±1.6% of the liver remains in OS-remnant 90% hepatectomy. A total of 11.5±2.1% of liver remains in the RMS-remnant 90% hepatectomy. There were no differences in survival curves after 90% hepatectomy by clip technique between the OS-remnant (n=10) and the RMS-remnant (n=10) (p = 0.3588).
RMS, right middle segment; OS, omental segment.
Histopathological findings of clip-touched hepatic remnant and DHM in hepatectomy by the clip technique
Histopathological findings of the clip-touched hepatic remnant near the PHM at 6 h after 80% hepatectomy are shown in Fig. 8 and 8B. There were no findings that suggested obstructions by the hemostatic clip, except for those consistent with massive hepatectomy. Histopathological findings of DHM at 6 h after 80% hepatectomy are shown in Fig. 8C and 8D. Severe ischemic and massive necroses were confirmed.
Figure 8.
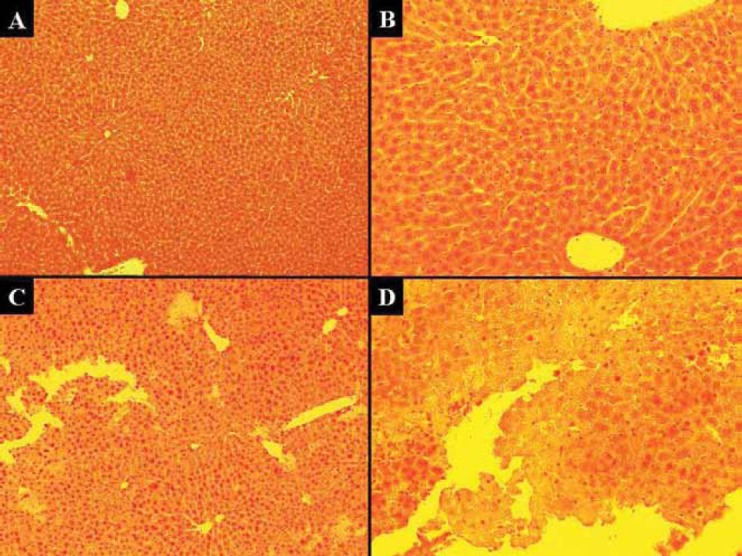
Histopathological findings of clip-touched hepatic remnant near the PHM and DHM. A. and B. There were no findings which suggested obstructions by the hemostatic clip in the clip-touched hepatic remnant near the PHM (findings at 6 h after 80% hepatectomy). Findings by H-E staining at 100× (A) and 200× (B) magnification. C. and D. In the DHM, severe ischemic and massive necrosis were confirmed (findings at 6 h after 80% hepatectomy). Findings by H-E staining at 100× (C) and 200× (D) magnification.
PHM, proximal hepatic margin; DHM, distal hepatic margin.
Focal and/or patchy necrosis after hepatectomy
Focal and patchy necrosis (Fig. 9A) was usually observed after massive hepatectomy, although 90% hepatectomy showed this finding in our institution. In our experience, this finding was observed at several hours post-operation. At 6 h after 80% hepatectomy, there was no difference in the rate of appearance of focal and/or patchy necrosis between the suture technique and the clip technique (p = 0.6202) (Fig. 9B). Similar results were obtained at 6 h after 75% hepatectomy.
Figure 9.
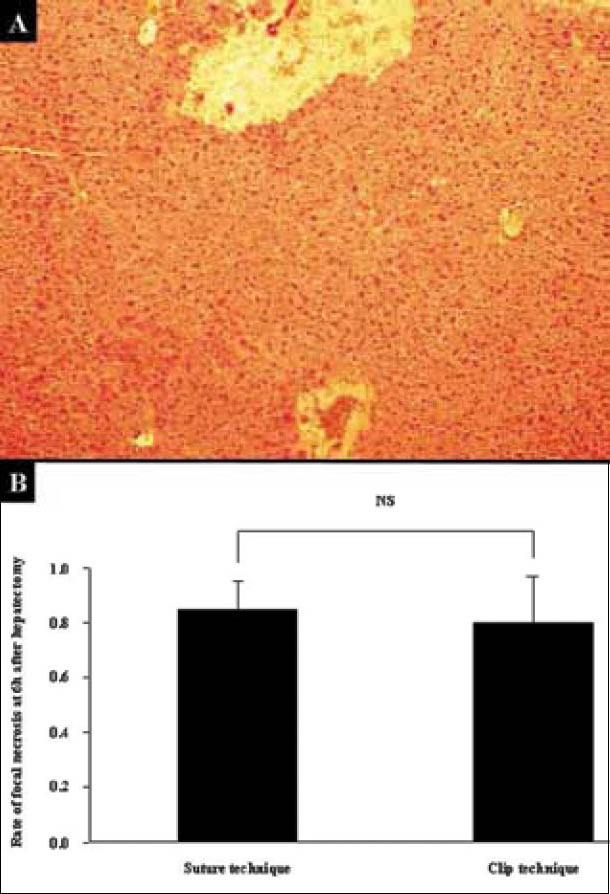
Focal and patchy necrosis after massive hepatectomy. A. Focal and patchy necrosis was usually observed after massive hepatectomy. Findings by H-E staining at 100× magnification are shown. B. The rates of appearance of focal and/or patchy necrosis in hepatectomy were calculated from ten cases in each technique. Experiments were repeated three times. Histopathological analyses were performed at 6 h after 80% hepatectomy. There was no difference in the rate of appearance of focal and/or patchy necrosis between the suture technique and the clip technique (p = 0.6202).
Discussion
A number of different survival curves have been previously reported following massive hepatectomy in the mouse. Differences in study design and institutional methodology as well as various complications may explain these discrepancies [4]. As such, we recommend that survival curves should be checked beforehand according to institutional methodology and study design in each laboratory. In our institution we have two types of 90% hepatectomy models available, while other models of approximately 90% hepatectomy exist [1,7]. Anatomical analysis of each institution’s animal strain is crucial for development of reliable models. All mice that receive 90% hepatectomy eventually die after surgery, although 90% hepatectomy has some advantages, especially in studies of liver failure and hepatic surgery. Inderbitzin et al [8] reported that OS exhibits different behaviors according to the degree of liver-volume, and will not work in small-volume hepatectomy. Currently, our massive hepatectomy models employed the OS in only the 80% hepatectomy model, because we have a surgical option in the 90% hepatectomy model. In our experience, the OS of some mice exhibit a few branches from veins, except for the PV, because swelling due to portal hypertension was often mild even after 90% hepatectomy and color change was often not enhanced after ligation of the PV trunk. Overall, we consider that RMS-remnant 90% hepatectomy will provide more relevant data from the viewpoint of strict effects (i.e., liver damages) due to portal hypertension.
The outcomes of murine hepatectomy can vary greatly if surgical procedures are not performed properly. We consider that approximately 30 cases are required in hepatectomy by the suture technique for initial achievement of reliable survival curves, and that approximately 50 cases are required to start the study. By contrast, approximately 20 cases are enough in hepatectomy by the clip technique for reliable samples. Our operative time study for massive hepatectomy clearly indicated that the procedures in the suture technique were more complicated than those in the clip method. Overall, we consider that massive hepatectomy by the clip technique is advantageous because of its simplicity, although its safety may be still questionable.
The hepatocyte is the first cell to start the proliferation reaction after hepatectomy [4]. Although histopathological injury can be confirmed from several hours after hepatectomy, some important signals for liver regeneration start in the later phase. As such, a suitable hepatectomy model must be selected according to experimental purpose. Jin et al [14] reported no focal and/or patchy necrosis even after massive hepatectomy model, although this necrosis is an important finding after hepatectomy [4]. These histopathological findings are confirmed at several hours after hepatectomy [4]. However, in our study a few mice that received 80% or 75% hepatectomy did not demonstrate necrosis, while all mice that received 90% hepatectomy showed necrosis in the early postoperative period. These discrepancies are consistent with survival curves because a few mice that received 80% or 75% hepatectomy survived long term. These survivors can be used to provide liver samples with long-term observation after massive hepatectomy, and are useful for many studies that require long recovery times after massive hepatectomy. Based on our data on the rate of appearance of this characteristic necrosis, the clip technique can provide reliable and relevant data in massive hepatectomy mouse models.
Focal and patchy necroses are also observed as secondary findings after biliary stasis and/or congestion by outflow obstruction. Some surgical problems including in- and outflow obstructions, massive bleeding and bile stasis will invalidate results. All mice move well after complete recovery, and it is possible that the clip may slide following aggressive movements after recovery from anesthesia and surgery, although our results showed similar phenomena between the clip and suture techniques. During surgery, the hepatic margin may be changed according to clip size. Large-sized clips require more PHM for flow safety and more DHM for complete hemostasis. Although we often treat RAS and LAS in an en bloc manner using an ML-sized clip, only one of the smallest feasible clips to one segment should be used to prevent unexpected surgical issues. Surgeons should also note any unexpected findings after hepatectomy procedures. Dilated IHIVC is a sign of disturbed flow of the IVC, because clipping of the RAS, LAS and LPS may cause a twist of the SHIVC, while clipping of the RMS and RPS may cause stenosis of the HIVC. Segmental congestion and partial color change in the liver also suggest outflow and/or inflow obstruction. During autopsy, unexpected color changes of the liver, massive coagula and bile leakage are informative for unstable postoperative course. To produce reliable samples, mice that indicate unexpected signs during surgery or autopsy should not be used to take samples.
In conclusion, our clip technique models for massive hepatectomy in the mouse are simple and require only basic surgical skills, and provide reproducible results.
Summary Box.
What is already known:
Murine model of hepatectomy is so important in the research field.
Despite the widespread use of the 70% hepatectomy, alternative hepatectomy models with resected volumes >70% are required to provide more clinically relevant experiments on liver regeneration and hepatic failure.
The benefits of the hemostatic clip in the murine hepatectomy models with resected volumes <70 % had been reported.
What the new findings are:
Herein, we investigated the segmental volume in the murine liver, and describe detailed surgical procedures of our innovative hepatectomy model in the mouse.
Our clip technique is useful even for hepatectomy with resected volumes >70%.
Moreover, our models with clip technique for massive hepatectomy in the mouse are simple and require only basic surgical skills, and provide reproducible results.
Acknowledgments
We are grateful to Dennis W. Dickson, Monica Castanedes-Casey, Virginia R. Phillips, Linda G. Rousseau and Melissa E. Murray (Department of Neuroscience, Mayo Clinic in Florida, Jacksonville, FL 32224, USA) for their technical support in histopathological evaluations. We are also grateful to Christopher B Eckman and Aimee R Herdt (Department of Neuroscience, Mayo Clinic in Florida, Jacksonville, FL 32224, USA) for their support.
Biography
Mayo Clinic in Florida, Jacosonville, FL, USA
Footnotes
Conflict of Interest: None
Financial disclosures: This work was supported by grants to J.H. Nguyen from the Deason Foundation, Sandra and Eugene Davenport, Mayo Clinic CD CRT-II, AHA 0655589B and NIH R01NS051646-01A2, and partially supported by a grant to T. Hori from the Uehara Memorial Foundation (No. 200940051, Tokyo 171-0033, Japan).
References
- 1.Higgins G, Anderson R. Experimental pathology of the liver. I. Restoration of the liver of the white rat following partial surgical removal. Arch Path Lab Med. 1931;12:186–202. [Google Scholar]
- 2.Madrahimov N, Dirsch O, Broelsch C, et al. Marginal hepatectomy in the rat: from anatomy to surgery. Ann Surg. 2006;244:89–98. doi: 10.1097/01.sla.0000218093.12408.0f. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Hori T, Nguyen JH, Zhao X, et al. Comprehensive and innovative techniques for liver transplantation in rats: a surgical guide. World J Gastroenterol. 2010;16:3120–3132. doi: 10.3748/wjg.v16.i25.3120. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Mitchell C, Willenbring H. A reproducible and well-tolerated method for 2/3 partial hepatectomy in mice. Nat Protoc. 2008;3:1167–1170. doi: 10.1038/nprot.2008.80. [DOI] [PubMed] [Google Scholar]
- 5.Nikfarjam M, Malcontenti-Wilson C, Fanartzis M, et al. A model of partial hepatectomy in mice. J Invest Surg. 2004;17:291–294. doi: 10.1080/08941930490502871. [DOI] [PubMed] [Google Scholar]
- 6.Martins PN, Neuhaus P. Hepatic lobectomy and segmentectomy models using microsurgical techniques. Microsurgery. 2008;28:187–191. doi: 10.1002/micr.20478. [DOI] [PubMed] [Google Scholar]
- 7.Makino H, Togo S, Kubota T, et al. A good model of hepatic failure after excessive hepatectomy in mice. J Surg Res. 2005;127:171–176. doi: 10.1016/j.jss.2005.04.029. [DOI] [PubMed] [Google Scholar]
- 8.Inderbitzin D, Studer P, Sidler D, et al. Regenerative capacity of individual liver lobes in the microsurgical mouse model. Microsurgery. 2006;26:465–469. doi: 10.1002/micr.20271. [DOI] [PubMed] [Google Scholar]
- 9.Greene AK, Puder M. Partial hepatectomy in the mouse: technique and perioperative management. J Invest Surg. 2003;16:99–102. [PubMed] [Google Scholar]
- 10.Boyce S, Harrison D. A detailed methodology of partial hepatectomy in the mouse. Lab Anim (NY) 2008;37:529–532. doi: 10.1038/laban1108-529. [DOI] [PubMed] [Google Scholar]
- 11.Rodriguez G, Lorente L, Duran HJ, et al. A 70% hepatectomy in the rat using a microsurgical technique. Int Surg. 1999;84:135–138. [PubMed] [Google Scholar]
- 12.Aller MA, Mendez M, Nava MP, et al. The value of microsurgery in liver research. Liver Int. 2009;29:1132–1140. doi: 10.1111/j.1478-3231.2009.02078.x. [DOI] [PubMed] [Google Scholar]
- 13.Cornell RP, Liljequist BL, Bartizal KF. Depressed liver regeneration after partial hepatectomy of germ-free, athymic and lipopolysaccharide-resistant mice. Hepatology. 1990;11:916. doi: 10.1002/hep.1840110603. [DOI] [PubMed] [Google Scholar]
- 14.Jin X, Zhang Z, Beer-Stolz D, et al. Interleukin-6 inhibits oxidative injury and necrosis after extreme liver resection. Hepatology. 2007;46:802–812. doi: 10.1002/hep.21728. [DOI] [PubMed] [Google Scholar]