

Abstract
Background
In patients with non-cardiac chest pain (NCCP), gastroesophageal reflux disease (GERD) is thought to be the commonest cause. Ambulatory pH monitoring and/or endoscopy are usually performed in order to confirm GERD diagnosis. At present, clinical diagnosis of reflux in patients with NCCP is uncertain.The aim of the study was to determine clinical characteristics that could identify GERD in patients with NCCP.
Methods
A total of 52 (age 52.8±1.8 yrs, 29 women) patients with NCCP underwent combined impedance-pH monitoring and gastroscopy. GERD diagnosis was based on the presence of esophagitis and/or a positive impedance-pH study (symptom index >50% and/or esophageal acid exposure time >4.0%). Patients were then divided into 2 groups: GERD- and non-GERD-related NCCP. Demographic and clinical parameters were compared between these two groups.
Results
GERD-related NCCP was found in 30 (58%) patients. Demographic characteristics were similar in both groups. Chest pain showed no difference in severity, radiation, relation to exercise and relation to sleep between the two groups. In the GERD-related NCCP group, chest pain was more prevalent during the postprandial period (P<0.05) and was relieved by spontaneous use of antireflux drugs (P<0.05). The presence of typical reflux symptoms favored a GERD diagnosis (P<0.05).
Conclusions
A proportion of patients with NCCP showed clinical characteristics suggesting a GERD diagnosis. Typical reflux symptoms, postprandial chest pain and use of anti-reflux drugs for pain relief were the best predictors for GERD-related NCCP.
Keywords: Non-cardiac chest pain, GERD, clinical characteristics
Introduction
Non cardiac chest pain (NCCP) is defined as recurrent chest pain that is indistinguishable from ischemic heart pain after a reasonable workup has excluded a cardiac cause [1]. The annual prevalence of non-cardiac chest pain is approximately 25% [2]. It is a benign condition with no impact in mortality but with impaired quality of life [3]. In patients without cardiac disease, the esophagus is the most common source of NCCP. Gastroesophageal reflux disease (GERD) is the most common esophageal cause for NCCP constituting up to 60% of the cases [3,4].
The major dilemma for clinicians is identifying whether GERD may be responsible for the patient's presentation [5]. Clinical diagnosis of GERD is difficult and often requires invasive tests such as gastroscopy, esophageal pH/impedance monitoring and esophageal manometry [4]. However, all these diagnostic modalities have limitations and none of them is considered the gold standard for the diagnosis. Recently, the empirical trial therapy with proton pump inhibitors (PPIs) has been proposed as the initial diagnostic test to identify GERD as the etiology of NCCP [6,7]. Although the PPI test is a simple, non-invasive test with a relatively high sensitivity in identifying GERD as a cause of NCCP, it is still far from being considered perfect.
Given the fact that there is a lack of clinical criteria to determine which patients would benefit from these tests, all of them are indiscriminately subjected to the above tests. To date, very few studies have been conducted regarding the clinical presentation of patients with NCCP and the way their symptoms can direct our diagnostic work-up.
The purpose of our study is to determine clinical characteristics that could identify GERD in patients with NCCP.
Materials and methods
Study population
We included patients who had had at least 3 episodes of chest pain per week for a minimum of 3 months. Patients were referred by a cardiologist after a diagnostic evaluation excluded a cardiac source for their chest pain; they had either normal coronary angiogram or lack of ischemic heart disease on exercise treadmill or stress thallium testing. Patients were excluded if they were using non-steroid anti-inflammatory drugs (NSAIDs) or aspirin, had a history of upper gastrointestinal surgery, peptic stricture, gastric or duodenal ulcer, connective tissue disease, diabetes mellitus and severe liver, lung, renal or hematological disease. The study protocol was approved by the Attikon University General Hospital Institutional Review Board. Informed written consent was obtained from all participating patients.
All patients filled out a detailed questionnaire about symptoms including presence of typical symptoms of GERD (heartburn and/or regurgitation) and presence of atypical symptoms such as sleep disturbances, chronic cough, chronic laryngitis, asthma, sinusitis, pharyngitis, hoarseness and dental erosions. Heartburn was defined as a burning sensation in the retrosternal area (behind the breastbone) and regurgitation as the perception of flow or refluxed gastric content into the mouth or hypopharynx [8]. The patients were asked to mention chest pain severity, duration, radiation, relation to exercise, relation to food intake, relief with water intake and improvement with spontaneous use of antireflux or other drugs. Symptom severity was measured on a 10-point Likert scale ranging from 1 (very mild) to 10 (very severe). Basic demographic data including weight, height, body mass index, age, alcohol consumption, smoking and use of drugs were recorded.
All patients underwent upper endoscopy esophageal manometry in order to exclude the presence of any esophageal motility disorder and to identify the position of the lower esophageal sphincter (LES), and 24-h ambulatory impedance-pH monitoring.
Upper endoscopy
After an overnight fast, all patients underwent an upper endoscopy using a forward viewing video endoscope. If necessary, they were sedated for the procedure by intravenous administration of midazolam (up to 5 mg). During endoscopy, the presence of esophagitis was noted and graded according to the Los Angeles classification [9].
Ambulatory impedance-pH monitoring
A 6-channel impedance catheter (outer diameter 2.3 mm) with attached pH recording at 5 cm above the manometrically localized LES was used. Before each study, the catheter was calibrated in buffer solutions of pH 7 and 4. For intraluminal impedance, the catheter enabled recordings from 6 segments, each recording segment being 2 cm. The recording segments were located at 2-4, 4-6, 8-10, 10-12, 14-16 and 17-19 cm above the manometrically localized LES. The pH and impedance signals were stored in a digital system (Omega, MMS, Enschede, The Nederlands) using a sample frequency of 50 Hz [10].
Study protocol
All patients underwent an upper gastrointestinal endoscopy, followed by stationary esophageal manometry. Patients were off PPIs for the gastroscopy. Ambulatory 24-h esophageal impendance-pH monitoring was performed on one of the next 7 to 10 days. PPIs were discontinued for at least 15 days. Drugs that may affect gastrointestinal motility and gastrointestinal secretion were also discontinued at least 1 week prior to the study. Data collection device was worn in a belt on the patient's chest. Patients were instructed to resume normal activity and diet, maintain a daily diary that included the time of meal consumption, the occurrence of symptoms, posture changes and activities.
Data analysis
For the 24-h esophageal impendance-pH monitoring analysis the periods of meal consumption were marked and excluded. Percentage of time with esophageal pH<4 was calculated and pathological esophageal acid reflux was present when esophageal pH was <4 for 4% of time. The symptom index (SI) was calculated in relation to acid and non-acid reflux episodes. Symptom was considered to be associated with reflux if it was preceded within 2 minutes by a reflux episode [11]. A positive SI was defined if >50% of the symptoms were associated with pathological reflux [12]. If pathological esophageal acid reflux and/or positive SI were present, it was considered as evidence suggestive of GERD diagnosis.
Patients with erosive esophagitis in gastroscopy and/or abnormal 24-h ambulatory impedance-pH monitoring were classified as GERD-related NCCP. Patients with gastroscopy without esophagitis and negative 24-h ambulatory impedance-pH monitoring were classified as non-GERD-related NCCP.
Statistical methods
Values were expressed as mean ± SD. Statistical analysis was performed by Student's t test or Chi-square testing wherever appropriate. All P-values <0.05 were considered to be significant.
Results
Fifty two patients (29 women; mean age: 52.8±1.8 years) with NCCP were included in our study. GERD-related NCCP was identified in 30 patients (58%). Flow chart summarized the findings of gastroscopy and impedance-pH monitoring for the classification of patients with GERD-related NCCP (Fig. 1). Erosive esophagitis was found in 9 (17%) patients; five had grade A, 3 grade B and 1 grade C. Abnormal impedance-pH monitoring was found in 25 (48%) patients. Pathological esophageal acid reflux was present in 17 patients and SI was positive in 8 patients; four had a positive SI for acid and 4 a positive SI for non-acid. Four patients with esophagitis also had pathologic impedance-pH monitoring. Esophageal manometry was normal in all patients.
Figure 1.
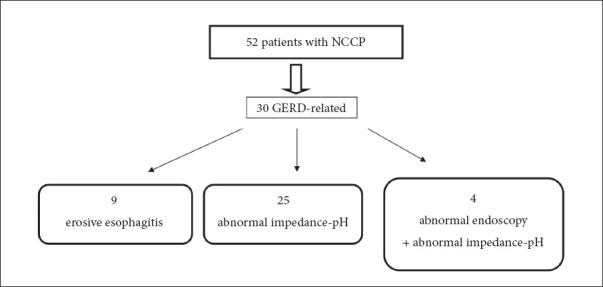
Flow chart of our study population
NCCP, non-cardiac chest pain; GERD, gastroesophageal reflux disease
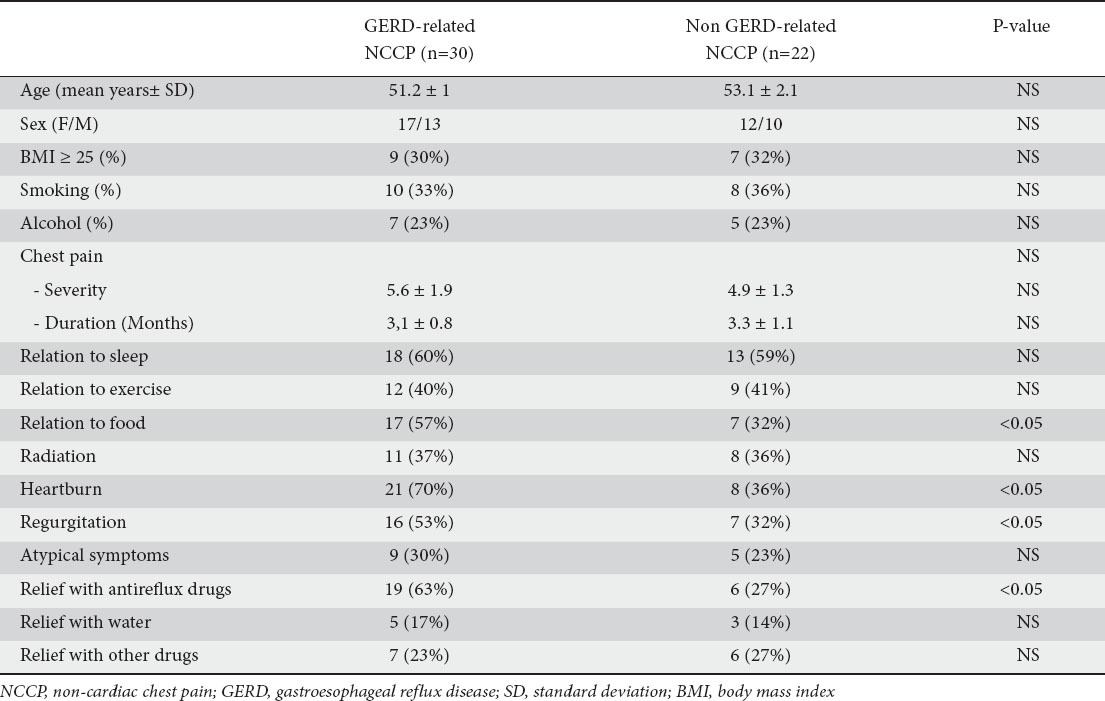
The presence of typical GERD symptoms was more pronounced in GERD-related NCCP patients; heartburn was mentioned by 21 (70%) patients compared to 8 (36%) patients with non-GERD-related NCCP (P<0.05) whereas regurgitation was mentioned by 16 (53%) and 7 (32%) patients, respectively (P<0.05). Moreover, significantly more patients with GERD-related NCCP observed chest pain at the postprandial period compared to those without GERD-related NCCP (17 vs. 7 patients respectively, P<0.05). Relief of chest pain by spontaneous use of antireflux drugs was also seen more frequently in patients with GERD-related NCCP (19 vs. 6 patients respectively, P<0.05).
The presence of atypical symptoms was similar in both groups. There was no significant difference between the two groups in chest pain duration, severity, radiation, relation to exercise, relation to sleep, relief on water intake and other drugs. The two groups did not differ significantly in sex, age, BMI, smoking history and history of alcohol consumption. Table 1 summarizes the comparison of clinical and demographic characteristics in patients with GERD and without GERD-related NCCP.
Table 1.
Demographic and clinical characteristics
Discussion
Our study showed that in patients with NCCP the presence of certain clinical features such as typical reflux symptoms of heartburn and/or regurgitation, postprandial chest pain and use of anti-reflux drugs for pain relief could imply diagnosis of GERD. Using gastroscopy and combined impedance-pH monitoring, we found that the prevalence of GERD in patients with NCCP was 58%. This is in accordance with previous studies which showed GERD in up to 60% of patients with NCCP [3]. However, studies from Asia showed a lower prevalence of GERD in patients with NCCP ranging from 41% to 44.8% [13,14]. This discrepancy could be explained by the fact that GERD symptoms have been traditionally considered more frequent in Western populations compared to Asian ones [15].
The presence of esophageal mucosal abnormalities consistent with GERD appears to be quite low in patients with NCCP questioning the utility of upper endoscopy in this population. Indeed, we found that only a minority of patients (17%) had evidence of erosive esophagitis in gastroscopy. This rate was consistent with studies which showed that the prevalence of reflux esophagitis in NCCP patients was between 10 to 19% [16]. Thus, ambulatory 24-h esophageal pH testing is particularly helpful in those patients who had normal endoscopy. The recently developed combined impedance-pH technology has the ability to detect all reflux episodes independent of the pH of the refluxate with impedance and concomitant pH recording to determine their acidity classifying them as acid or non-acid [17]. Impedance-pH monitoring has greater sensitivity than pH monitoring alone in the detection of gastroesophageal disease [18,19].
Using combined impedance-pH monitoring we revealed that 25 (48%) patients with NCCP had evidence of GERD indicators. Pathological esophageal acid reflux was found in 17 (68%) of these patients and positive SI in 8 (32%). Four (16%) patients had a positive SI for acid reflux and another 4 (16%) for non-acid reflux. The 4 patients with positive SI for non-acid reflux would have been identified as negative for GERD and represent the increased diagnostic yield of the combined impedance-pH monitoring compared to pH monitoring alone.
We tried to identify clinical predictors of GERD as a cause of NCCP and so we found the presence of typical symptoms, pain at the postprandial period and relief of pain with antireflux drugs to be predictors. Firstly, we observed a high prevalence of typical symptoms of GERD (heartburn and/or regurgitation) in the GERD-related NCCP patients. Our study was in accordance with the results of a previous study showing that typical GERD symptoms were more often present in GERD-related NCCP patients, but we found significantly higher rates of typical GERD [13]. This result suggests that the co-existence of typical GERD symptoms in patients with NCCP means a higher possibility of GERD as a cause of pain in these patients. In addition, we found that in GERD-related NCCP patients, chest pain was more prevalent during the postprandial period. Keeping in mind that in patients with GERD the majority of symptoms occur postprandially, our results seem logical. However, previous studies failed to confirm that GERD-related NCCP patients had an association between pain and relation to food [13]. Finally, we observed that in GERD-related NCCP patients, chest pain was relieved by spontaneous use of anti-reflux drugs. A similar finding was reported by others [13]. Anti-reflux drugs are the treatment of choice for patients with GERD, so the fact that there is pain relief with such drugs in GERD-related NCCP suggests that GERD is the cause of pain.
The current diagnostic approach in NCCP patients is an empirical trial therapy with a high dose of PPIs for all patients in order to determine acid-related pain. Following this therapeutic approach, PPIs should be given to all patients. According to our results, therapy with a high dose of PPIs could be given only to NCCP patients with typical reflux symptoms, pain at the postprandial period and relief of pain with spontaneous use of antireflux drugs. Therefore, patients with NCCP and one of the above predictors will benefit more from PPIs than those without any predictor. On the contrary, when predictors are absent, the response rate may be low after PPI treatment.
The main limitation of our study was the fact that although we ascribe GERD as the etiology of chest pain based on parameters observed on gastroscopy and 24-h impedance-pH monitoring, we did not evaluate the effectiveness of PPI therapy in those GERD-related NCCP patients.
In conclusion, a proportion of patients with NCCP showed clinical characteristics suggesting a GERD diagnosis. The presence of typical reflux symptoms, postprandial chest pain and spontaneous use of anti-reflux drugs for pain relief were the best predictors for GERD-related NCCP. Using these predictors it is possible to subgroup patients who are more likely to respond to PPI therapy avoiding excess use of drugs.
Summary Box.
What is already known:
Gastroesophageal reflux disease (GERD) is thought to be the commonest cause of non-cardiac chest pain (NCCP)
Empirical therapy with proton pump inhibitors, ambulatory pH monitoring and endoscopy are usually used to confirm GERD diagnosis
Clinical diagnosis of reflux in patients with NCCP is uncertain
What the new findings are:
GERD diagnosis was found in 58% of patients with NCCP
Clinical characteristics could be used to identify GERD as a cause of NCCP
Typical reflux symptoms, postprandial chest pain and use of anti-reflux drugs for pain relief were the best predictors for GERD-related NCCP
Biography
Athens Medical School, Laikon General Hospital; Athens Medical School, Attikon University General Hospital
Footnotes
Conflict of Interest: None
References
- 1.Fass R, Achem SR. Noncardiac chest pain: epidemiology, natural course and pathogenesis. J Neurogastroenterol Motil. 2011;17:110–123. doi: 10.5056/jnm.2011.17.2.110. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Eslick GD, Jones MP, Talley NJ. Non-cardiac chest pain: prevalence, risk factors, impact and consulting--a population-based study. Aliment Pharmacol Ther. 2003;17:1115–1124. doi: 10.1046/j.1365-2036.2003.01557.x. [DOI] [PubMed] [Google Scholar]
- 3.Richter JE. Chest pain and gastroesophageal reflux disease. J Clin Gastroenterol. 2000;30:39–41. [PubMed] [Google Scholar]
- 4.Faybush EM, Fass R. Gastroesophageal reflux disease in noncardiac chest pain. Gastroenterol Clin North Am. 2004;33:41–54. doi: 10.1016/S0889-8553(03)00131-6. [DOI] [PubMed] [Google Scholar]
- 5.Oranu AC, Vaezi MF. Noncardiac chest pain: gastroesophageal reflux disease. Med Clin North Am. 2010;94:233–242. doi: 10.1016/j.mcna.2010.01.001. [DOI] [PubMed] [Google Scholar]
- 6.Wang WH, Huang JQ, Zheng GF, et al. Is proton pump inhibitor testing an effective approach to diagnose gastroesophageal reflux disease in patients with noncardiac chest pain?: a meta-analysis. Arch Intern Med. 2005;165:1222–1228. doi: 10.1001/archinte.165.11.1222. [DOI] [PubMed] [Google Scholar]
- 7.Cremonini F, Wise J, Moayyedi P, et al. Diagnostic and therapeutic use of proton pump inhibitors in non-cardiac chest pain: a metaanalysis. Am J Gastroenterol. 2005;100:226–232. doi: 10.1111/j.1572-0241.2005.41657.x. [DOI] [PubMed] [Google Scholar]
- 8.Vakil N, van Zanten SV, Kahrilas P, et al. Global Consensus Group The Montreal definition and classification of gastroesophageal reflux disease: a global evidence-based consensus. Am J Gastroenterol. 2006;101:1900–1920. doi: 10.1111/j.1572-0241.2006.00630.x. [DOI] [PubMed] [Google Scholar]
- 9.Lundella LR, Dentb J, Bennettc JR, et al. Endoscopic assessment of oesophagitis: clinical and functional correlates and further validation of the Los Angeles classification. Gut. 1999;45:172–180. doi: 10.1136/gut.45.2.172. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Bredenoord AJ, Weusten BL, Timmer R, et al. Minimum sample frequency for multichannel intraluminal impedance measurement for the oesophagus. Neurogastroenterol Motil. 2004;16:713–719. doi: 10.1111/j.1365-2982.2004.00575.x. [DOI] [PubMed] [Google Scholar]
- 11.Lam HG, Breumelhof R, Roelofs JM, et al. What is the optimal time window in symptom analysis of 24-hour esophageal pressure and pH data? Dig Dis Sci. 1994;39:402–409. doi: 10.1007/BF02090215. [DOI] [PubMed] [Google Scholar]
- 12.Bredenoord AJ, Weusten BL, Smout AJ. Symptom association analysis in ambulatory gastro-oesophageal reflux monitoring. Gut. 2005;54:1810–1817. doi: 10.1136/gut.2005.072629. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Mousavi S, Tosi J, Eskandarian R, et al. Role of clinical presentation in diagnosing reflux-related non-cardiac chest pain. J Gastroenterol Hepatol. 2007;22:218–221. doi: 10.1111/j.1440-1746.2006.04416.x. [DOI] [PubMed] [Google Scholar]
- 14.Kim JH, Rhee PL, Park EH, Son HJ, Kim JJ, Rhee JC. Clinical usefulness of subgrouping of patients with non-cardiac chest pain according to characteristic symptoms in Korea. Gastroenterol Hepatol. 2007;22:320–325. doi: 10.1111/j.1440-1746.2006.04264.x. [DOI] [PubMed] [Google Scholar]
- 15.Wong WM, Lai KC, Lau CP, et al. Upper gastrointestinal evaluation of Chinese patients with non-cardiac chest pain. Aliment Pharmacol Ther. 2002;16:465–471. doi: 10.1046/j.1365-2036.2002.01217.x. [DOI] [PubMed] [Google Scholar]
- 16.Dickman R, Mattek N, Holub J, et al. Prevalence of upper gastrointestinal tract findings in patients with non-cardiac chest pain versus those with gastroesophageal reflux disease (GERD)- related symptoms: results from a national endoscopic database. Am J Gastroenterol. 2007;102:1173–1179. doi: 10.1111/j.1572-0241.2007.01117.x. [DOI] [PubMed] [Google Scholar]
- 17.Sifrim D, Castell D, Dent J, et al. Gastroesophageal reflux monitoring: review and consensus report on detection and definitions of acid, non-acid, and gas reflux. Gut. 2004;53:1024–1031. doi: 10.1136/gut.2003.033290. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Karamanolis G, Kotsalidis G, Triantafyllou K, et al. Yield of combined impedance-pH monitoring for refractory reflux symptoms in clinical practice. J Neurogastroenterol Motil. 2011;17:158–163. doi: 10.5056/jnm.2011.17.2.158. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Karamanolis G, Tutuian R. Role of non-acid in patients with non-erosive reflux disease. Ann Gastroenterol. 2013;26:100–103. [PMC free article] [PubMed] [Google Scholar]