

Abstract
Hepatitis C virus (HCV) infection is one of the major causes of hepatocellular carcinoma (HCC). Although predominant in cirrhotic HCV patients, the risk of HCC exists also in case of mere chronic hepatitis C (CHC). Thus the goal of the antiviral therapy is to obtain an early eradication of the HCV infection in order to reduce the risk of hepatocarcinogenesis. We report the case of a 61-year-old Caucasian male with CHC, who developed hemoperitoneum from HCC bleeding after having achieved sustained virological response (SVR). He underwent surgical resection and the histopathological examination showed a moderately-differentiated HCC in a slightly fibrotic liver. The patient has no tumor recurrence and keeps on doing well 18 months after surgery. This report, as many others, proves the existence of a residual risk of hepatocarcinogenesis in spite of obtaining an SVR in the absence of cirrhosis. Therefore, in our opinion, it is of primary importance to understand the underlying mechanisms of hepatocarcinogenesis and the major risk factors for HCC, in order to select those patients who most deserve a follow up. In this regard, we have proposed a different surveillance strategy according to the response to antiviral therapy, hepatic histology and the existence of one or more risk factors for HCC in SVR patients.
Keywords: Hepatitis C virus, hepatocellular carcinoma, sustained virological response
Introduction
Chronic hepatitis C (CHC) is one of the leading causes of hepatocellular carcinoma (HCC) [1-3]. Thus, an early eradication of hepatitis C virus (HCV) infection is a key point in order to stop the progression to cirrhosis and consequently to reduce the risk of developing HCC. Nevertheless, HCC can occur despite obtaining a sustained virological response (SVR) [4-6]. Therefore there is a need to clarify whether it is indicated, in term of cost-effectiveness, to extend the screening for HCC to SVR patients and, eventually, to define the most appropriate follow up method. In this report we describe the unusual clinical case of a non-cirrhotic HCV Italian patient, who developed an hemoperitoneum from HCC bleeding, 13 years after the achievement of SVR.
Case report
A Caucasian 61-year-old man was referred to our Hospital in 1993 due to elevated aspartate aminotransferase (AST) (eight times the upper limit of normal) with a slight increase in the gamma-glutamyl transferase (GGT) and was diagnosed as having CHC. He had no history of alcohol abuse, intravenous drug use, blood transfusions and drug intake. The patient’s medical history was notable for lung silicosis and hypertension without any secondary complication. His body mass index (BMI) was 25.51 kg/m2. He tested positive for HCV antibodies and negative for other causes of liver disease (other viral infections, hepatic autoimmunity, medications, hyperferritinemia, metabolic diseases). In 1993 the assessment of HCV-RNA and genotype by serum polymerase chain reaction (PCR) were not available, so no relative data at the time of the diagnosis exist. Other laboratory findings included a preserved liver function and a normal platelet count (Table 1). Abdominal examination and ultrasonography excluded hepatosplenomegaly and hepatic nodules. The liver biopsy, performed in 1994, showed stage 2 fibrosis with a moderate necro-inflammatory activity (A2 grade) according to the Desmet’s classification [7], and a mild microvescicolar hepatic steatosis.
Table 1.
Patient characteristics
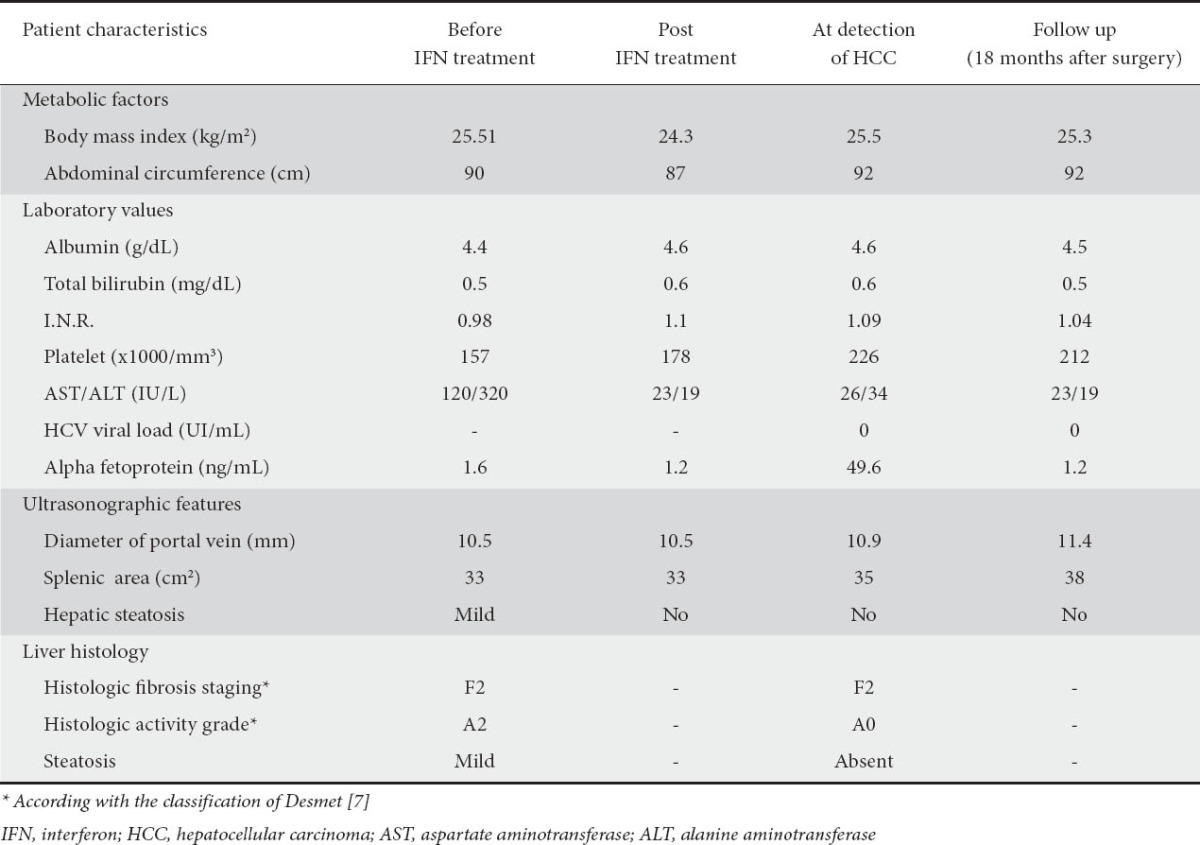
One year later, in January 1994, he was treated with 3MU of interferon-alpha 2a (Roferon) three times a week for 48 weeks, achieving a biochemical and SVR.
From 1996 to 2009 HCV-RNA was undetectable with normal AST/ALT.
In August 2009 the patient was referred to our emergency room for the onset of severe abdominal pain. On abdominal examination, there was distention, rebound and guarding with moderate ascites. The remaining physical examination and vital signs were normal. Laboratory findings showed mild anemia with normal platelet count and a preserved liver function. HCV RNA was undetectable and alpha-fetoprotein was elevated (Table 1).
Contrast-enhanced computed tomography (CT) found a large (8.6 cm) hepatic mass in segment IV, with a vascular pattern typical of HCC, ascites and no evidence of portal vein thrombosis. The subsequent diagnostic paracentesis confirmed the presence of hemoperitoneum.
During his hospital stay, there was a spontaneous stabilization of hemoglobin levels and a progressive pain relief. The gastroscopy was negative for esophageal and gastric varices. Therefore, on 4th November 2009 he underwent a left hepatectomy extending to the fifth hepatic segment. Intraoperatively a plurinodular mass of 7 cm in diameter was found, well demarcated from the remaining liver parenchyma. Histological evaluation revealed a moderately-differentiated HCC (grade G2 according to Edmondson and Steiner) [8], in the absence of vascular invasion; the number of mitosis was less than 1 per 10 high power fields. His liver fibrosis on the resected specimen remained at stage 2.
He was discharged at home on hospital day 24 and has returned to full activity. Three months after surgery the level of alpha-fetoprotein decreased from 49.6 ng/mL pre-resection to 2.4 ng/mL. At the last visit in June 2011 he was well and CT-scan showed no evidence of recurrent tumor.
Discussion
HCC can develop in about 2.5-4.2% of CHC non-cirrhotic SVR patients [4-6,9]. Infact, despite the findings showing a protective role of interferon and SVR, a residual risk of carcinogenesis still remains [2]. For this reason, it becomes of primary importance to identify the factors associated with the development of HCC in sustained responders, in order to be able to detect high-risk patients who need to be monitored closely. The major risk factors for HCC in SVR patients are male sex, advanced age (older than 50-60 years old, according to the studies), advanced histologic stage (>F3 [7]) [2,4-6,9]. Other possible risk factors include: hepatic steatosis [5], a low platelet count [2,9], a high AST level (which reflects a more advanced fibrotic stage) [9], an elevated ALT level at the end of interferon treatment (which probably reflect the persistence of hepatic inflammation, perhaps due to the presence of other underlying risk factors for the development of hepatocellular injury) and an alcohol intake over 27 g/day [2,4]. On the other hand, the type of interferon (alpha 2a/2b, pegylated or not), the type of therapy (mono or combination therapy), previous interferon treatments, HCV genotype and viral load pre-treatment did not influence significantly the rare of hepatocarcinogenesis [2].
There are many possible mechanisms of hepatocarcinogenesis in long-term responding patients: the persistence of a liver injury, such as occult infection with HBV or HCV [4-6], the preexistence of microscopic tumor foci, which becomes detectable by diagnostic imaging only after the end of the treatment [9] or the persistence of known risk factors for HCC (alcohol abuse, non alcoholic fatty liver disease and diabetes mellitus) [5,6].
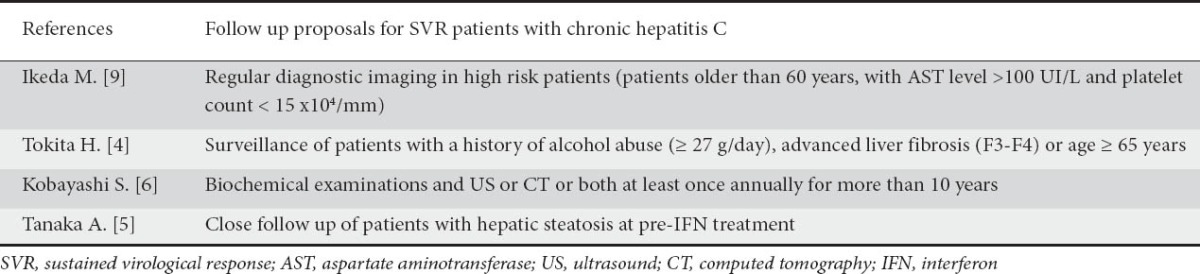
Therefore, in our opinion, a strategy of surveillance should be carried out even in SVR patients, in order to make an early diagnosis and allow them to undergo curative surgical treatment reducing the healthcare costs [6]. Many studies agree in suggesting the need of surveillance in these patients. In Table 2 all these proposals are summarized: some authors, such as Kobayashi et al, suggest an annual radiological and biochemical follow up of all SVR patients [6], while others suggest the surveillance only in high-risk patients (older patients with advanced disease) [4,6,9].
Table 2.
Authors’ follow up proposals
On the other hand, Lok et al, in a prospective analysis of patients included in the HALT-C trial, is doubtful about the cost-effectiveness of a similar follow up, because of the low incidence of HCC in non-cirrhotic patients [10]. Nevertheless, in Kobayashi’s retrospective study, as in many others we have reported before, HCC developed in 3.5% of SVR non-cirrhotic patients [6]; this data, in our opinion, is not of negligible importance and allow us to provide a surveillance also in this group of patients.
In view of the above considerations and based on our clinical experience, we have tried to merge the several suggestions of follow up, in order to propose a shared scheme of surveillance. In our opinion, such strategy should be based on the degree of liver fibrosis, on the response to antiviral treatment and on the presence of risk factors for HCC in SVR patients (Table 3).
Table 3.
Follow up based on the entity of liver fibrosis, on the response to antiviral treatment and on the presence of one or more risk factors for HCC in SVR patients
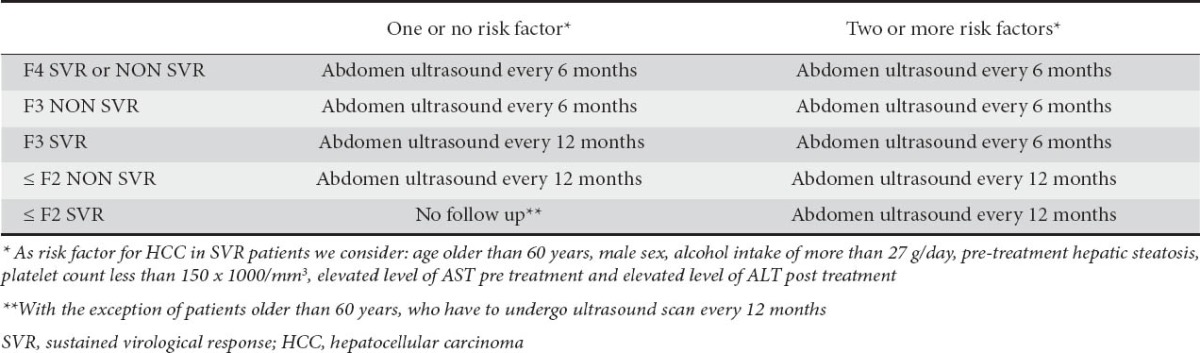
In agreement with the AASLD guidelines [1], all the cirrhotic patients should undergo an ultrasound abdomen every six months. The same for patients with advanced liver fibrosis (F3), SVR or not, with one or more risk factors for HCC. On the other hand, in F3 liver fibrosis SVR patients with one or no risk factors or in patients with mild-moderate liver fibrosis and a risk for HCC (SVR or not) we would propose an annual abdomen ultrasound. In particular, available data suggest that this surveillance strategy will have to be taken in patients over 60 years old, even in the absence of other risk factors. Finally, in mild-moderate liver fibrosis SVR patients with one or no risk factor for HCC, there is no need of surveillance.
We are aware that, at present, this strategy of follow up cannot be extended to clinical practice, but prospectively designed studies are needed to elucidate this field.
Biography
Santa Maria Nuova Hospital in Reggio Emilia, Italy
Footnotes
Conflict of Interest: None
References
- 1.Bruix J, Sherman M. Management of hepatocellular carcinoma: An Update. Hepatology. 2011;53:1020–1022. doi: 10.1002/hep.24199. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Yoshida H, Shiratori Y, Moriyama M, Arakawa Y, Ide T, Sata M, Inoue O, et al. Interferon therapy reduces the risk for hepatocellular carcinoma: national surveillance program of cirrhotic and noncirrhotic patients with chronic hepatitis C in Japan. IHIT Study Group. Inhibition of Hepatocarcinogenesis by Interferon Therapy. Ann Intern Med. 1999;131:174–181. doi: 10.7326/0003-4819-131-3-199908030-00003. [DOI] [PubMed] [Google Scholar]
- 3.Vezali E, Agheno A, Lampertico P, Colombo M. Does interferon therapy prevent hepatocellular carcinoma in patients with chronic viral hepatitis? Clin Res Hepatol Gastroenterol. 2011;35:455–464. doi: 10.1016/j.clinre.2011.02.008. [DOI] [PubMed] [Google Scholar]
- 4.Tokita H, Fukui H, Tanaka A, et al. Risk factors for the development of hepatocellular carcinoma among patients with chronic hepatitis C who achieved a sustained virological response to interferon therapy. J Gastroenterol Hepatol. 2005;20:752–758. doi: 10.1111/j.1440-1746.2005.03800.x. [DOI] [PubMed] [Google Scholar]
- 5.Tanaka A, Uegaki S, Kurihara H, et al. Hepatic steatosis as a possible risk factor for the development of hepatocellular carcinoma after eradication of hepatitis C virus with antiviral therapy in patients with chronic hepatitis C. World J Gastroenterol. 2007;13:5180–5187. doi: 10.3748/wjg.v13.i39.5180. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Kobayashi S, Takeda T, Enomoto M, et al. Development of hepatocellular carcinoma in patients with chronic hepatitis C who had a sustained virological response to interferon therapy: a multicenter, retrospective cohort study of 1124 patients. Liver Int. 2007;27:186–191. doi: 10.1111/j.1478-3231.2006.01406.x. [DOI] [PubMed] [Google Scholar]
- 7.Desmet VJ, Gerber M, Hoofnagle JH, Manns M, Scheuer PJ. Classification of chronic hepatitis: diagnosis, grading and staging. Hepatology. 1994;19:1513–1520. [PubMed] [Google Scholar]
- 8.Edmondson HA, Steiner PE. Primary carcinoma of the liver: a study of 100 cases among 48,900 necropsies. Cancer. 1954;7:462–503. doi: 10.1002/1097-0142(195405)7:3<462::aid-cncr2820070308>3.0.co;2-e. [DOI] [PubMed] [Google Scholar]
- 9.Ikeda M, Fujiyama S, Tanaka M, et al. Risk factors for development of hepatocellular carcinoma in patients with chronic hepatitis C after sustained response to interferon. J Gastroenterol. 2005;40:148–156. doi: 10.1007/s00535-004-1519-2. [DOI] [PubMed] [Google Scholar]
- 10.Lok AS, Everhart JE, Wright EC, et al. For the HALT-C Trial Group. Maintenance peginterferon therapy and other factors associated with hepatocellular carcinoma in patients with advanced hepatitis C. Gastroenterology. 2011;140:840–849. doi: 10.1053/j.gastro.2010.11.050. [DOI] [PMC free article] [PubMed] [Google Scholar]