

Abstract
Background
The aim of this study was to identify inflammatory bowel disease (IBD) patients’ perspectives regarding everyday life issues.
Methods
From October 2010 till April 2011, 1,181 IBD patients completed an anonymous questionnaire through the internet (827 cases) or at the outpatient clinic of the participating centers (354 cases), aiming to identify: a) the impact of disease on social life, emotional status and work productivity; b) the source of disease information; and c) the level of support from family members and friends.
Results
Fifty-five percent of the patients reported that IBD interferes with their social life, while 65% felt stressed, 60% depressed and 19% tired because of it. Disease information (physician/ internet) was reported only by 31%, while 26% admitted not discussing their therapy with their gastroenterologist. Forty percent felt that the health service they receive is not satisfactory, with 76% desiring more gastroenterologists, 67% more outpatient clinics, 49% more dieticians and 42% more psychologists specialized in IBD. IBD interfered with working capacity in 40% of the participants, while 57% needed time off of work (ranging from 1-20 days per year). One of three patients (32%) has not informed his work environment about the disease; however, 88% had the support of their family and friends for coping with it.
Conclusions
Greek IBD patients claim that health-related social life, emotional status and work productivity are severely affected by their disease, whereas they complain about lack of information regarding the therapy. These unmet demands call for immediate action by healthcare providers and society.
Keywords: Inflammatory bowel disease, quality of life, work productivity, patients’ information on IBD, family support to cope with IBD
Introduction
Crohn’s disease (CD) and ulcerative colitis (UC), collectively known as inflammatory bowel disease (IBD) are chronic conditions characterized by a relapsing-remitting or chronic active disease. Patients with IBD most often deal with unpredictable, unpleasant and potentially embarrassing gastrointestinal symptoms, in addition to treatment-related side effects.
Although medical therapy aims at controlling intestinal inflammation, minimizing symptoms and preventing complications of the disease, awareness has been raised regarding IBD and its treatment impact on patients’ quality of life, as well as their capacity to carry on with a normal social and professional life [1]. Therefore, there is an increasing need to incorporate assessments of patients’ emotional and social well-being into treatment decision making and estimates of health outcome [2,3]. These data will help us determine which aspects of disease management could be improved to meet patients’ demands.
Thus, the objective of this study was to explore patients’ perspectives on how and to what extent IBD impacts their social life, emotional status, and work productivity. Additionally, we sought to explore how patients get disease information and the level of support by family members and friends.
Methods
From October 2010 till April 2011, consecutive, unselected patients with IBD visiting the outpatient clinics of the participating centers were invited to participate in a survey organized by the “Hellenic Foundation of Gastroenterology & Nutrition” in collaboration with the “Ulcerative Colitis & Crohn’s Disease Patients’ Association”. The only eligibility criterion was the age range of 18 to 65 years old. Participants were excluded if they had additional co-morbidities impacting adversely their everyday life (i.e. heart, lung or renal failure) and/or if for any reason they were unable to complete the questionnaire. Extra-intestinal manifestations were not an exclusion criterion.
All participants were asked to complete an anonymous questionnaire, aiming to assess the impact of IBD on certain parameters of their everyday life. Return of a completed questionnaire was taken as consent of the patient to participate in the study.
The questionnaire was formulated by the researchers and was composed of 4 sections. Part A collected data regarding patients’ social life and their disease-related emotional status. Part B explored patients’ knowledge regarding IBD and how they obtained information regarding their disease (latest developments and available treatments). Part C dealt with living at their working environment, relationship with their colleagues and supervisor and work productivity. Finally, part D explored patients’ perceptions with regard to the support they receive from their family and friends. The questionnaire was written in Greek and every effort was made to construct questions based on the Greek way of life. The questionnaire was not previously tested on a pilot study and therefore it has not been validated.
This study was approved by the Institutional Review Board at each participating center.
Statistical analysis
All analyses were conducted using the SPSS 17.0 software (Chicago, IL). Descriptive statistics were used to evaluate the response. The Chi-squared test and the Fisher’s exact test were used when testing the hypothesis regarding categorical variables. In all comparisons a P value <0.05 was regarded as significant.
Results
Overall, 1,264 patients were invited to participate in this survey. Forty-two patients declined participation, citing lack of interest and lack of time, 14 patients were excluded because of co-morbidities, whereas 27 patients did not return the questionnaire. Thus, 1,181 IBD patients were subjected to the final analysis. Of those, 827 completed the questionnaire via internet and 354 at the outpatient clinic of the participating centers. Patients’ and disease characteristics, together with their employment status and level of education are provided in Table 1.
Table 1.
Patient and disease characteristics at study entry
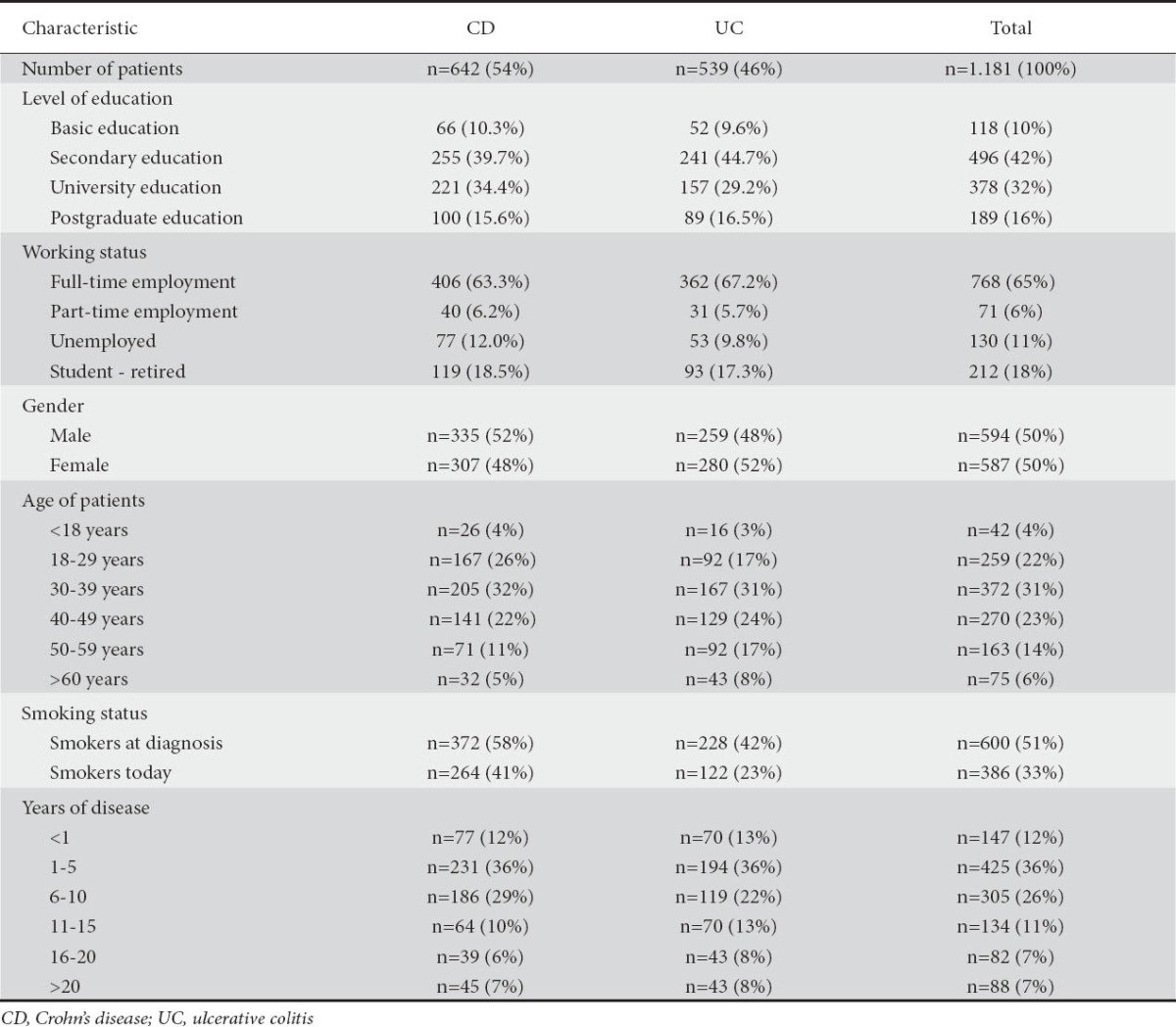
Seventeen percent of the patients reported suffering from other non-socially interfering chronic illnesses, 51% had been smoking before the diagnosis while 33% were still smoking. Of note, 69% reported some kind of abdominal pain during the last 2 weeks, while 77% reported excessive flatulence during the same time period. Thirty-two percent of the patients visited a gastroenterologist as soon as their symptoms appeared and 37% did so within a period of 6 months. At the time of completing the questionnaire, 81% of the patients were in remission and 19% had a flare of their disease.
Social life and emotional status
The majority of patients (55%) reported that they had to cancel their participation at a social event because of their disease during the last 2 weeks (Fig. 1). Nine percent of the patients (CD: 11%, UC: 7%) reported that this was a frequent incident (often/all the time). Nineteen percent felt tired either frequently or constantly (CD: 21%, UC: 16%). Sixty percent felt depressed or disappointed because of the disease; this problem was more prevalent in patients with a recent diagnosis of IBD (<5 years). Sixty-five percent reported being stressed because of the disease. Finally, 25% felt anger due to the problems they face and this feeling was more intense in younger and in female patients.
Figure 1.
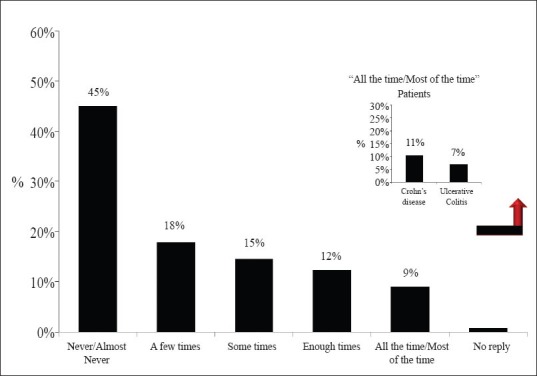
Frequency of cancellation of participation in a social event due to inflammatory bowel disease during the last 2 weeks
Information about the disease
It is of interest that only 31% of our patients reported that they were informed on the latest advances in IBD (from their physician: 30%, through the internet: 16%). Moreover, 26% said that they did not discuss with their gastroenterologist their therapy and did not take part in the decision-making process regarding the treatment options. Almost half of the patients were not happy with the degree of knowledge they have about their disease and the information they received from their doctor. Patients said that they needed more thorough information regarding complications of disease (especially cancer) and treatment-related adverse events (Fig. 2). This was particularly true for patients between the age of 30-39 and for those suffering from CD. Finally, 40% of our patients felt that the health service they receive is not satisfactory, with 76% desiring more gastroenterologists specialized in IBD, 67% more IBD outpatient clinics, 49% more IBD dieticians and 42% more psychologists specialized in IBD (Fig. 3).
Figure 2.
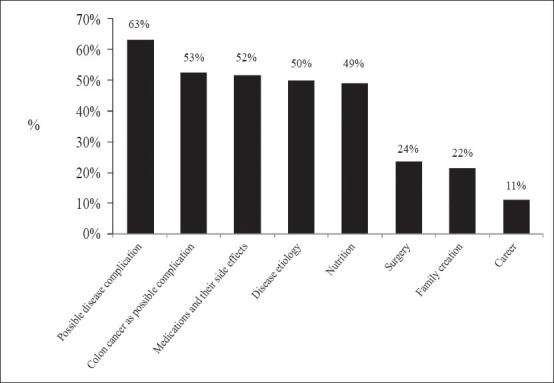
Issues on which inflammatory bowel disease patients need more information
Figure 3.
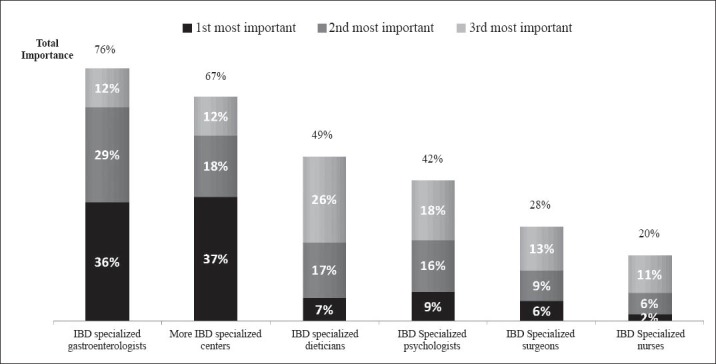
Actions that would improve inflammatory bowel disease patients’ health service Figure 4 Days off of work because of inflammatory bowel disease during the last year for those employed
Effect on work productivity
A considerable percentage of IBD patients reported that the disease did not let them select or enter the university they desired (22%) and precluded them from following the career they would have pursued otherwise (28%). Problems associated with the symptoms of IBD were found to interfere with working capability in 40% of the study patients. The problem was more prevalent in patients between the age groups of 18-29 and 40-49 years old. More than half of the patients (57%) needed to take time off of work, because of problems related to the disease or because of the need to visit the outpatient clinic. The days off of work ranged from 1-20 days per year (Fig. 4). One of three patients (32%) had not informed their boss or colleagues about the disease, either because they felt this was a personal matter (65%) or because of fear of possible negative consequences. From those who had informed their working environment, 30% reported that they did not have the desired support. Finally, only 37% of patients reported that the attending physician was willing to be informed on their ability to work and to offer appropriate support.
Figure 4.
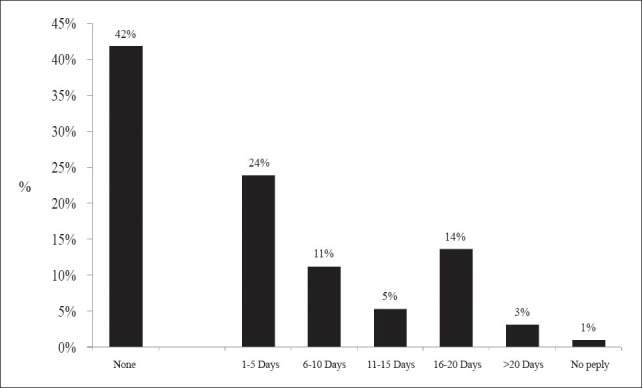
Days off of work because of inflammatory bowel disease during the last year for those employed
Support from family and friends
The vast majority of our patients (88%) reported having overwhelming support from their family and friends, without which they would not be able to cope with the burden of their disease. This was tremendously important for patients younger than 29 years old. However, the desire for support from dieticians and psychologists was expressed by 77% and 71% of our patients respectively.
Discussion
Taking into account the abundance of literature data regarding advances in the pathogenesis, diagnosis and therapy of IBD, it is of interest that only a few studies have so far reported on the impact of the disease on patients’ quality of life. Quality of life assessments have been an integral part of almost all recent large randomized controlled therapeutic trials in the field of IBD [4,5], but they offer a transient estimate of how different therapeutic regimens impact on patients’ lives. On the other hand, studies focusing on quality of life in IBD are difficult to compare due to significant methodological differences. However, a common outcome of these studies is that IBD exerts a huge impact on the psychosocial aspects of a patient’s life [6-9]. In a recent study, 63% of patients reported symptoms of anxiety and depression at some point [10]. Other studies have also demonstrated that rates of depression in IBD patients were three times higher than those in the general population [11]. In accordance with these observations, our results show that a substantial number of patients feel depressed (60%) or even angry (25%) because of their disease, which interferes with social life in more than half of the cases. In addition, 19% feel tired either often or constantly, confirming previous reports that IBD patients experience a high rate of fatigue, usually associated with disease activity, poor sleep quality and perceived stress [12].
Surprisingly, only 31% of our patients report being regularly informed about disease advances and only 30% obtained this information directly from the treating physician. Sixteen percent resort to the internet to get information, although the reliability of the medically-oriented websites visited could not be tested since this was not included in the questionnaire. Even more disappointing is the fact that 26% admit that they do not discuss their therapy with the attending gastroenterologist, whereas 40% feel that the health services they receive are not satisfactory. The major reasons for this condition are the lack of appropriately organized outpatients’ clinics, empowered by specialized personnel (qualified IBD physicians and surgeons, IBD nurses, psychologists, stoma-therapists, dietitians, etc.), limited resources and inappropriate structure and function of outpatient clinics in tertiary hospitals in our country. Therefore, it is not surprising that the patients have emphasized the need for more gastroenterologists, outpatient clinics, dieticians and psychologists specialized in IBD.
IBD has a considerable effect on employment behavior of affected persons in their prime working years [13,14]. According to our results, problems associated with the symptoms of IBD interfere with working capability in 40% of patients participating in the study, while more than half need to take time off of work, which ranges from 1 to 20 days per year. This data is in agreement with findings of Boonen et al [15] who reported that IBD has a significant impact on labor force participation, which is higher for CD than for UC and higher in younger and more highly educated patients. IBD-related sick leave rates in their study were 29.1% and 41.1% for UC and CD patients, respectively. The average unemployment rate in a Norwegian cohort was approximately twice higher than in the background population (11.7% versus 4.1%), while IBD-related sick leave rates were 19% and 25% for UC and CD patients, respectively [16]. The higher rate of nonparticipation in the work force, as well as the increased number of days off of work for those who are actually employed, are both major contributors to the indirect costs of illness in IBD patients [17]. In a Swedish study, indirect costs comprised 68% of the total cost (direct plus indirect costs) of IBD to society [18]. The investigators also found that 47% of the indirect costs were related to sickness leave and the remaining 53% were the result of early retirement.
Thirty-two percent of the patients in this study underreport their clinical status to their employers and/or colleagues at work. On the other hand, approximately one third of those who have informed their employers of their disease, claim that they never had the desired level of support. Our results on this parameter are in contrast to the limited data available from previously published studies claiming that IBD patients are not facing significant discrimination at work and most patients seem to disclose IBD to their employers [19-22]. Wyke et al conducted a 6-year prospective study, in which a total of 81% of patients disclosed IBD diagnosis to their employers and 77% stated that their employers had been helpful [23]. These differences may reflect different cultural habits in the working environment between nations and/or different level of fear for job loss in the countries where the studies have been performed.
Finally, our patients quote an overwhelming support from family members and friends, which mirror the strong bonds amongst relatives and close social partners in the Greek society. There is mounting evidence suggesting that a strong social support network in persons with chronic illnesses can facilitate effective coping with stressors, exerts a positive effect on health status and improves the outcome of disease [24,25]. In addition, strong and steady support from family and friends may at least in theory compensate for gaps and pitfalls of a health system that cannot provide the desired support to its patients.
There are several lessons that should be learned from the results of this study. Previous reports have also revealed that physicians frequently underestimate the functional impairment noted in IBD patients [2,3]. In a study by Drossman et al, physicians’ rating about CD severity was poorly correlated with patients’ overall health, since the quality of life scoring was lower in the sociopsychological domain than in the physical domain [26]. The psychological functioning is obviously more difficult to be handled by the physician and therefore it is usually omitted from patient assessment. However, given the importance of functional impairment experienced by our patients, it is obvious that there is an increasing need for gastroenterologists to conceptualize patient health more broadly and incorporate assessments of patient emotional and social well being into treatment decision making.
Our study has several strengths, since the results reported are representative of a large cohort of IBD population in Greece. The study sample is among the largest in the IBD literature, since we had an unusually high response rate to the questionnaire (94.48%), depicting of course the influence which the issues studied had on our patients. It is also of note that 25% of the participants were diagnosed more than 10 years ago, suggesting that responses were provided by patients with a good understanding of their condition. Furthermore, the fact that our study is among the few in the literature to be conducted in southern Europe allowed us to report results that, in some instances, deviate from those already published. Of course our study has several weaknesses as well, since we did not use any validated health related quality of life index to quantify our results; however, our study was not designed to measure exactly this, but rather aimed to give a wider view on IBD patients’ perspectives. Our goal was to use a questionnaire that would be closer to the patients’ “real life” scenario, instead of using a pre-formulated questionnaire designed abroad for patients with different needs and different views to ours. Although it could be argued that, because of this, direct comparison with the results of other studies is difficult, we believe that several conclusions regarding differences in patients’ responses have been noted and are mentioned previously.
In conclusion, the results of this study clearly reinforce the significant impact of IBD on the psychosocial aspects of patients’ lives. Greek IBD patients seek a better organized medical and hospital environment (increased number of IBD outpatient clinics, gastroenterologists, dieticians and psychologists), a tighter relationship with their physician leading to a deeper understanding of their emotional and social status and also the opportunity to receive more disease-related information and a broad educational program for those responsible for human resources in their working environment. IBD patients’ associations and groups in collaboration with IBD specialized medical personnel should stimulate public and/or social authorities to pay more attention and draw action on the above-mentioned unmet needs.
Summary Box.
What is already known:
Patients with inflammatory bowel disease (IBD) most often deal with unpredictable, unpleasant and potentially embarrassing gastrointestinal symptoms, in addition to treatment-related side effects
IBD exerts a huge impact on the psychosocial aspects of patients’ lives
IBD has considerable effect on employment behavior by affecting persons in their prime working years
What the new findings are:
A substantial number of Greek patients feel depressed (60%) or even angry (25%) because of their disease, which interferes with social life in more than half of the cases
Only 31% of our patients report regular information for disease advances and only 30% obtained this information directly from the treating physician
Problems associated with the symptoms of IBD interfere with working capability in 40% of patients, while more than half need to take time off work which ranges from 1 to 20 days per year
Greek patients quote an overwhelming support from family members and friends, which mirror the strong bonds amongst relatives and close social partners in the Greek society
Acknowledgments
The authors thank ABBOTT Laboratories (Hellas) for the support during the study period, as well as for the assistance with the statistical analysis of the results. We also thank our IBD patients for their willingness to share personal issues with us. The following members of the Hellenic Society for the Study of inflammatory bowel disease are thanked for their participation in and contribution to the study: G. Paspatis, K. Triantafyllou, A. Karolidis, I. Koutroubakis, K. Papadakis, D. Karagiannis, Ch. Kalantzis, G. Alexandrakis, M. Mylonaki, J. Triantafylidis, N. Phronas, M. Tzouvala, K. Goumas, I. Katsogridakis, G. Margantinis, K. Papamichail, G. Karamanolis
Biography
Evagelismos General Hospital Athens; Venizelion Hospital, Heraklion, Crete; Attikon Hospital, Athens; University General Hospital of Alexandroupolis; Papanikolaou General Hospital, Thessaloniki; Aghia Olga Hospital, Athens, Greece
Footnotes
Conflict of Interest: None
References
- 1.Westwood N, Travis S. What do patients with inflammatory bowel disease want for their clinical management? Aliment Pharmacol Ther. 2008;27(Suppl 1):1–8. doi: 10.1111/j.1365-2036.2008.03605.x. [DOI] [PubMed] [Google Scholar]
- 2.Stephens R, Hopwood P, Girling D. Randomized trials with quality of life endpoints: are doctors’ ratings of patients’ physical symptoms interchangeable with patients’ self-ratings? Qual Life Res. 1997;6:225–236. doi: 10.1023/a:1026458604826. [DOI] [PubMed] [Google Scholar]
- 3.Calkins D, Rubenstein L, Cleary P, et al. Failure of physicians to recognize functional disability in ambulatory patients. Ann Intern Med. 1991;114:451–454. doi: 10.7326/0003-4819-114-6-451. [DOI] [PubMed] [Google Scholar]
- 4.Colombel J, Sandborn W, Reinisch W, et al. Infliximab, azathioprine, or combination therapy for Crohn's disease. N Engl J Med. 2010;362:1383–95. doi: 10.1056/NEJMoa0904492. [DOI] [PubMed] [Google Scholar]
- 5.Sandborn W, Hanauer S, Rutgeerts P, et al. Adalimumab for maintenance treatment of Crohn's disease: results of the CLASSIC II trial. Gut. 2007;56:1232–1239. doi: 10.1136/gut.2006.106781. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Hoivik M, Moum B, Solberg I, et al. Health-related quality of life in patients with ulcerative colitis after a 10-year disease course: results from the IBSEN study. Inflamm Bowel Dis. 2012;18:1540–1549. doi: 10.1002/ibd.21863. [DOI] [PubMed] [Google Scholar]
- 7.Gray W, Denson L, Baldassano R, Hommel K. Disease activity, behavioral dysfunction and health-related quality of life in adolescents with inflammatory bowel disease. Inflamm Bowel Dis. 2011;17:1581–1586. doi: 10.1002/ibd.21520. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Blondel-Kucharski F, Chircop C, Marquis P, et al. Health related quality of life in Crohn's disease: a prospective longitudinal study in 231 patients. Am J Gastroenterol. 2001;96:2915–2920. doi: 10.1111/j.1572-0241.2001.4681_b.x. [DOI] [PubMed] [Google Scholar]
- 9.Muller K, Prosser R, Bampton R, Mountifield R, Andrews J. Female gender and surgery impair relationships, body image and sexuality in inflammatory bowel disease: patient perceptions. Inflamm Bowel Dis. 2010;16:657–663. doi: 10.1002/ibd.21090. [DOI] [PubMed] [Google Scholar]
- 10.Magro F, Portela F, Lago P, et al. Inflammatory bowel disease: a patient's and caregiver's perspective. Dig Dis Sci. 2009;54:2671–2679. doi: 10.1007/s10620-008-0658-3. [DOI] [PubMed] [Google Scholar]
- 11.Fuller-Thomson E, Sulman J. Depression and inflammatory bowel disease: findings from two nationally representative Canadian surveys. Inflamm Bowel Dis. 2006;12:697–707. doi: 10.1097/00054725-200608000-00005. [DOI] [PubMed] [Google Scholar]
- 12.Graff L, Vincent N, Walker J, et al. A population based study of fatigue and sleep difficulties in inflammatory bowel disease. Inflamm Bowel Dis. 2011;17:1882–1889. doi: 10.1002/ibd.21580. [DOI] [PubMed] [Google Scholar]
- 13.Marri S, Buchman A. The education and employment status of patients with inflammatory bowel diseases. Inflamm Bowel Dis. 2005;11:171–177. doi: 10.1097/00054725-200502000-00011. [DOI] [PubMed] [Google Scholar]
- 14.Rogala L, Miller N, Graff L, et al. Population-based controlled study of social support, self-perceived stress and work issues and access to health care in inflammatory bowel disease. Inflamm Bowel Dis. 2008;14:526–535. doi: 10.1002/ibd.20353. [DOI] [PubMed] [Google Scholar]
- 15.Boonen A, Dagnelie P, Feleus A, et al. The impact of inflammatory bowel disease on labor force participation: results of a population sampled case-control study. Inflamm Bowel Dis. 2002;8:382–389. doi: 10.1097/00054725-200211000-00002. [DOI] [PubMed] [Google Scholar]
- 16.Bernklev T, Jahnsen J, Henriksen M, et al. Relationship between sick leave, unemployment, disability and health related quality of life in patients with inflammatory bowel disease. Inflamm Bowel Dis. 2006;12:402–412. doi: 10.1097/01.MIB.0000218762.61217.4a. [DOI] [PubMed] [Google Scholar]
- 17.Longobardi T, Jacobs P, Bernstein C. Work losses related to inflammatory bowel disease in the United States: Results from the national health interview survey. Am J Gastroenterol. 2003;98:1064–1072. doi: 10.1111/j.1572-0241.2003.07285.x. [DOI] [PubMed] [Google Scholar]
- 18.Blomqvist P, Ekbom A. Inflammatory bowel diseases: health care and costs in Sweden in 1994. Scand J Gastroenterol. 1997;32:1134–1139. doi: 10.3109/00365529709002993. [DOI] [PubMed] [Google Scholar]
- 19.Mayberry M, Probert C, Srivastava E, et al. Perceived discrimination in education and employment by people with Crohn's disease: a case control study of educational achievement and employment. Gut. 1992;33:312–314. doi: 10.1136/gut.33.3.312. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Bonnevie O. A socio-economic study of patients with ulcerative colitis. Scand J Gastroenterol. 1967;2:129–136. doi: 10.3109/00365526709180058. [DOI] [PubMed] [Google Scholar]
- 21.Hay J, Hay A. Inflammatory bowel disease: cost of illness. J Clin Gastroenterol. 1992;14:309–317. doi: 10.1097/00004836-199206000-00009. [DOI] [PubMed] [Google Scholar]
- 22.Moody G, Probert C, Jayanthi V, et al. The attitude of employers to people with IBD. Soc Sci Med. 1992;34:459–460. doi: 10.1016/0277-9536(92)90306-b. [DOI] [PubMed] [Google Scholar]
- 23.Wyke R, Edwards F, Allan R. Employment problems and prospects of patients with inflammatory bowel disease. Gut. 1988;29:1229–1235. doi: 10.1136/gut.29.9.1229. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Broadhead W, Kaplan B, James S. The epidemiologic evidence for a relationship between social support and health. Am J Epidemiol. 1983;117:521–537. doi: 10.1093/oxfordjournals.aje.a113575. [DOI] [PubMed] [Google Scholar]
- 25.Mookadem F, Arthur H. Social support and its relationship to morbidity and mortality after acute myocardial infarction. Arch Intern Med. 2004;164:1514–1518. doi: 10.1001/archinte.164.14.1514. [DOI] [PubMed] [Google Scholar]
- 26.Drossman D, Patrick D, Mitchell C, et al. Health related quality of life in inflammatory bowel disease – functional status and patients worries and concerns. Dig Dis Sci. 1989;34:1379–1386. doi: 10.1007/BF01538073. [DOI] [PubMed] [Google Scholar]