

Introduction
Clinically relevant cardiovascular imaging methods to assess response to therapy and prognosis in patients presenting with acute ST segment elevation myocardial infarction (STEMI) are predicated upon their ability to accurately delineate both the area of myocardial infarction and the area of myocardium at risk for infarction secondary to coronary artery occlusion. At‐risk myocardium encompasses both reversible and irreversible myocardial injury and is defined as the portion of myocardium within a coronary artery territory that experiences an acute reduction in blood flow following obstruction of the supplying coronary artery in the absence of collateral flow. Without re‐establishment of myocardial perfusion, necrosis (irreversible injury) ensues as a “wavefront” from subendocardium to subepicardium and progressively involves more at‐risk myocardium over time.1 Thus, in the setting of a non‐reperfused transmural infarct, the area of at‐risk myocardium would be equivalent to the area of infarction in the absence of spontaneous reflow or opening of collaterals secondary to coronary occlusion. In instances of early reperfusion, resulting in only subendocardial myocardial infarction (MI), the region of myocardial salvage (reversible injury) comprises the non‐infarcted myocardium within the region of at‐risk myocardium (Figure 1). Therefore, through accurate delineation of infarcted and at‐risk myocardium, one can theoretically determine the amount of myocardial salvage by taking the difference between the 2 measures. The portion of at‐risk myocardium that will undergo infarction is based on several factors, the most important of which include the duration of coronary occlusion and the rate of propagation of infarction. Variables that affect the propagation rate of infarction may include metabolic factors, such as ischemic preconditioning and the degree of collateral blood flow.
Figure 1.
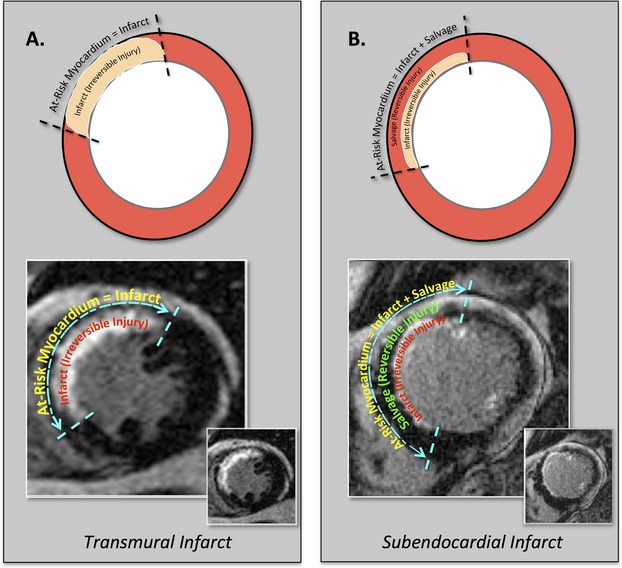
At‐risk myocardium=infarct (irreversible ischemic injury)+ salvage (reversible ischemic injury). Diagram establishing the relationships between at‐risk myocardium, infarct, and salvage in the setting of transmural and subendocardial myocardial infarction in the left anterior descending coronary artery territory.
The treatment of acute MI is predicated upon rapid restoration of myocardial blood flow with percutaneous revascularization techniques and adjunct cardioprotective therapies to minimize the amount of irreversibly injured myocardium and maximize myocardial salvage. In the setting of acute STEMI, patient outcomes are often dictated by final infarct size. While infarct size alone provides an attractive surrogate endpoint to assess the efficacy of drugs used in patients presenting with acute coronary syndromes, additional imaging to quantify the myocardial area at risk would allow for a more comprehensive assessment of therapeutic efficacy. As such, quantifying infarct size alone may be misleading, as similar‐sized infarcts may have smaller or larger associated areas of at‐risk myocardium (Figure 2) and not reflect the true severity of ischemic injury. Thus, it is important to normalize infarct size to the area at risk, as this allows for a more accurate measure of therapeutic success. In this way, incorporating the at‐risk myocardium controls for variations in collateral blood flow and accounts for anatomic variability in perfusion territories within individuals.
Figure 2.
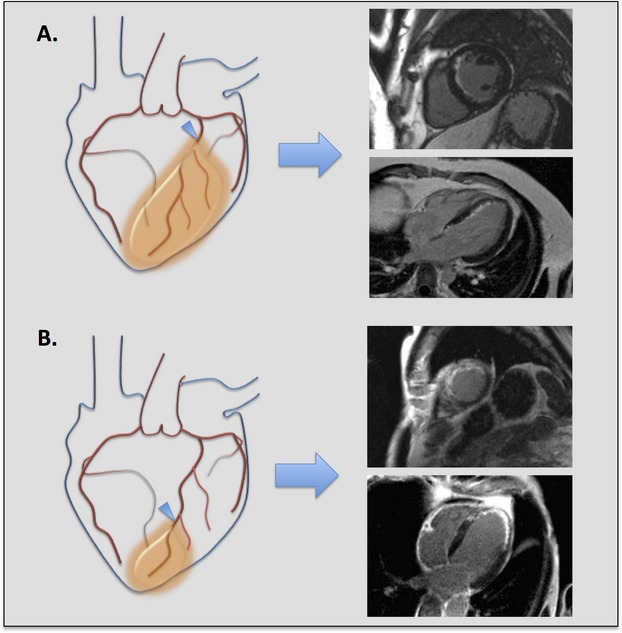
The importance of defining at‐risk myocardium, myocardial infarction, and myocardial salvage in the assessment of therapeutic efficacy for acute coronary syndrome. Two different examples of acute ischemic myocardial injury in the left anterior descending (LAD) coronary artery territory are illustrated. Corresponding delayed‐enhancement cardiac magnetic resonance (DE‐CMR) images in the short axis and 4 chamber orientations are shown for each example. Overall infarct size in each example is similar, but the amount of at‐risk myocardium and severity of ischemic injury differs. A, Proximal LAD occlusion (arrowhead) with large area of at‐risk myocardium (orange shading), subendocardial myocardial infarction, and significant myocardial salvage, suggesting less severe ischemic injury. B, Distal LAD occlusion (arrowhead) with small area of at‐risk myocardium (orange shading), transmural myocardial infarction, and no myocardial salvage, suggesting more severe ischemic injury.
In this contribution, we review contemporary imaging tests, specifically echocardiography, nuclear imaging methods, cardiac magnetic resonance imaging (CMR), and cardiac computed tomography (CT) techniques for the assessment of at‐risk myocardium in the pathophysiological context of myocardial infarction. The rationale for the clinical implementation of these methods over traditional techniques is explored.
Pathophysiology of Myocardial Infarction Secondary to Coronary Occlusion
Through landmark large animal experiments performed in the late 1970s, Reimer and Jennings first elucidated the temporal and anatomical progression of myocardial necrosis secondary to coronary artery occlusion.1 In these canine experiments, coronary occlusion times of <40 minutes with subsequent reperfusion resulted in a subendocardial infarct, in which infarct size was less than the area at risk, while coronary occlusion times of 6 hours or more resulted in a near transmural infarct, which encompassed nearly the entire area at risk.2 Important tenets regarding at‐risk myocardium have been derived from the work of Reimer and Jennings, and thus, form the basis for various cardiovascular imaging techniques used to evaluate at‐risk and infarcted myocardium. In the absence of myocardial perfusion, irreversible injury begins at the subendocardium and extends transmurally as a wavefront to progressively involve more myocardium with increasing coronary artery occlusion time. Additionally, during coronary occlusion, there is no circumferential wavefront of necrosis, as there is no perfusion gradient at the lateral borders of the infarct. The lateral margins of the infarct are, in fact, established as early as 40 minutes after cessation of epicardial coronary blood flow.1 It is important to note, however, that fundamental physiologic and metabolic differences may exist between various species, which may affect the applicability of findings from large animal studies when translated to humans.
From these initial experiments, it has been established that the area of at‐risk myocardium is always greater than or equal to the area of myocardial necrosis. Thus, as the transmural extent of necrosis increases, the region of at‐risk myocardium and the region of myocardial necrosis begin to approach each other in size and will eventually become equivalent in the absence of expeditious reperfusion. Furthermore, the transmural extent of myocardial necrosis is the primary determinant of overall infarct size, which has a significant impact on left ventricular systolic function and overall patient prognosis.3–4 When normalized to the area of at‐risk myocardium, a larger amount of myocardial salvage is indicative of a greater degree of therapeutic success through reperfusion with or wihout other novel cardioprotective strategies.
Interest in Noninvasively Defining the Myocardial Area at Risk
The goal of therapeutic intervention in the setting of acute MI is to reduce overall mortality and major adverse cardiac events. Given the significant reduction in cardiac morbidity and mortality from current guideline‐based interventional and medical therapy for acute MI, very large numbers of patients with long follow‐up periods are needed to adequately demonstrate improved survival based on the efficacy of a new treatment. Large patient cohorts and lengthy follow‐up periods carry with them a significant burden in terms of cost and time. Thus, there has been great interest in the development of surrogate endpoints for clinical trials, which aim to demonstrate therapeutic efficacy using smaller numbers of enrolled patients. Infarct size is an attractive surrogate endpoint and has been shown to have significant prognostic and management implications when measured by cardiac imaging methods.5–6 However, as discussed earlier, infarct size may not provide a true representation of the severity of ischemic injury. In the setting of acute MI, the ability to differentiate infarcted from at‐risk myocardium by imaging provides a means to derive a myocardial salvage index (percentage of noninfarcted myocardium within the area of at‐risk myocardium) that provides an attractive surrogate endpoint for the assessment of therapeutic efficacy in acute coronary syndromes. In fact, the measurement of myocardial salvage by nuclear and CMR imaging methods has been employed as a surrogate endpoint of therapeutic efficacy in recent clinical trials of acute myocardial infarction.7–9
The ability to apply cardiovascular diagnostic and imaging techniques to the pathophysiology of acute myocardial infarction has garnered significant interest over the last several decades. Clinicians and investigators have used the 12‐lead electrocardiogram as well as invasive coronary angiography to approximate the amount of at‐risk myocardium in the setting of acute coronary occlusion. However, noninvasive imaging techniques that can differentiate regions of reversible and irreversible myocardial injury in vivo offer the potential to provide critical information in assessing the effectiveness of therapies aimed at reducing infarct size and maximizing myocardial salvage. By and large, single‐photon emission computed tomography (SPECT) myocardial perfusion imaging with technetium‐based radiotracers has been the most widely used technique to assess at‐risk myocardium. In addition to perfusion, however, SPECT imaging with radiotracers that evaluate fatty acid and glucose metabolism have more recently been recognized for their potential to retrospectively evaluate the at‐risk myocardium. Myocardial contrast echocardiography (MCE) has also been used in the cardiac catheterization laboratory as a method to assess at‐risk myocardium in the acute phase of MI. Over the last several years, a renewed interest in the evaluation of at‐risk myocardium has been provided by CMR techniques, which aim to retrospectively delineate areas of reversible and irreversible myocardial injury, thus offering the potential to define both myocardial infarction and myocardial salvage within a single imaging session after the time of reperfusion. Capitalizing on principles similar to CMR, cardiac CT techniques are now emerging, which may offer the ability to differentiate myocardial infarction and regions of at‐risk myocardium. At present, however, it is important to understand the pathophysiologic basis and rationale for each of these cardiac imaging methods as a means to noninvasively assess both MI and at‐risk myocardium and objectively recognize their strengths as well as their limitations.
Traditional Methods for Assessing the Myocardial Area at Risk
Electrocardiography
Arguably, the most readily available diagnostic test in cardiovascular medicine for rapidly assessing at‐risk myocardium at the time of acute coronary occlusion and clinical symptoms is the 12‐lead electrocardiogram (ECG). Upon initial patient presentation, the ECG not only provides rationale for prompt triage of patients with STEMI to the cardiac catheterization lab for revascularization, but can also offer information on the presence and location of both at‐risk myocardium and myocardial infarction. Through the use of vectorcardiography, an ECG technique that measures the magnitude and direction of electrical forces of the heart, the ST‐segment vector, or “injury current” vector, can be used to identify patients with a large at‐risk area in the setting of acute STEMI. Depending on the direction and magnitude of the ST vector, one can localize the area of myocardial injury and at‐risk myocardium to a specific coronary artery territory, or infarct‐related artery (IRA). In this way, the ECG provides pathophysiologic information regarding the myocardium during acute ischemic injury without directly imaging the heart. Several methods have been described that attempt to quantify the myocardial area at risk by ECG.10–12 However, ECG scoring methods carry with them significant limitations and largely provide information regarding the presence or absence of at‐risk myocardium in a specific coronary artery territory rather than offering a robust method to accurately delineate infarction and salvage. At present, despite utility in the clinical setting, electrocardiographic methods for defining at‐risk and infarcted myocardium have suboptimal accuracy for assessing response to therapeutic intervention in the clinical setting given significant quantitative limitations.
Coronary Angiography
In the context of STEMI secondary to coronary artery obstruction, semiquantitative estimates of at‐risk myocardium have been derived from scores based on the location of occlusion of the IRA by coronary angiography. Advantages of such techniques include providing the interventional cardiologist with a rapid method to determine the amount of at‐risk myocardium at the time of angiography in order to guide revascularization. The Duke jeopardy score is a simplified angiographic method for estimating at‐risk myocardium based on the location of coronary artery stenoses.13 The BARI score incorporates vessel length and coronary artery luminal size to obtain a myocardial jeopardy index comprised of a ratio of the score associated with the IRA to the summed scores associated with the remainder of the coronary vasculature.14 The APPROACH score divides the left ventricle into regions according to the percentage of myocardium supplied by a coronary artery and is, in part, based on autopsy studies of the left ventricular myocardium.15 Although readily available and clinically useful at the time of revascularization, suboptimal quantitation of both the amount of at‐risk myocardium and infarcted myocardium precludes use of angiographic methods as a surrogate endpoint for the efficacy of adjuvant therapies in large clinical trials. Limitations of traditional electrocardiographic and angiographic methods have provided the impetus for the development of novel cardiac imaging techniques to more accurately quantify the spectrum of infarcted, at‐risk, and salvaged myocardium.
Cardiovascular Imaging Methods for Assessing the Myocardial Area at Risk
Echocardiography
MCE offers the ability to assess at‐risk myocardium by assessing myocardial perfusion through the injection of microbubbles, which provide increased echogenicity of normally perfused myocardium. As microbubble echo contrast is a microvascular tracer, regional absence of blood flow during coronary occlusion with MCE delineates the area of myocardium at risk for necrosis. Subsequently, after reperfusion, the persistent nonperfused region of myocardium has been shown to correlate with the area of MI. Kaul et al first demonstrated the ability of MCE to delineate the area at risk in vivo in a canine model of nonreperfused MI, where they demonstrated an excellent correlation between MCE with intracoronary contrast injection and ex vivo technetium autoradiography.16 Interestingly, they noted that the circumferential extent of the area at risk closely approximated the circumferential extent of the final infarct, regardless of the duration of coronary occlusion. These findings are in agreement with the original ex vivo animal studies of Reimer and Jennings in evaluating the myocardial area at risk. Ito et al were the first to use MCE with intracoronary contrast injection to evaluate myocardial perfusion before and after reperfusion in patients with anterior STEMI. Of note, their studies found evidence of residual perfusion defect immediately after reperfusion (no reflow) in ≈1 quarter of the patients studied.17 Villanueva et al subsequently showed in an animal model that MCE could be used with a vasodilator to assess the area at risk using a right atrial injection of highly concentrated echo contrast.18 This method provided rationale for at‐risk myocardium determination to risk stratify patients in the emergency department setting by using peripheral intravenous access rather than requiring intracoronary access in the cardiac catheterization lab. Further advances with harmonic imaging have allowed for evaluation of myocardial perfusion with small injections of microbubble echo contrast. Lindner et al performed MCE in patients with prior MI and demonstrated good correlation with SPECT perfusion imaging and significant advantages with a continuous infusion of echo contrast compared to bolus injection.19 More recently, molecular echocardiographic techniques have been developed that aim to detect “ischemic memory” through microbubble contrast agents targeted at endothelial leukocyte adhesion molecules. During coronary occlusion, there is overexpression of leukocyte adhesion molecules on the vascular endothelial surface as part of the inflammatory cascade associated with acute MI. Interestingly, these adhesion molecules persist for a period of time after restoration of coronary blood flow and offer the potential to retrospectively image at‐risk myocardium following reperfusion therapy for MI. Villanueva et al used microbubble ultrasound contrast targeted to P‐selectin to evaluate for evidence of recent myocardial ischemia in a murine model of ischemia/reperfusion. Their findings were remarkable for echocardiographic visualization of contrast enhancement in the area of at‐risk myocardium following 15 minutes of ischemia for ≥1 hour after the ischemic insult.20
Despite significant success as a research application, MCE is faced with limitations as a routine clinical method for assessing at‐risk myocardium. Traditional limitations of echocardiography, such as poor acoustic windows in patients with large body habitus, provide challenges for the routine clinical assessment of at‐risk myocardium. Additionally, the ability of a sonographer to consistently acquire conventional 2‐dimensional echo images with comprehensive coverage of the left ventricle is limited in comparison to tomographic imaging techniques, which allow for complete volumetric coverage of the left ventricle. However, with continued refinement 3‐dimensional echocardiographic techniques may obviate these challenges in the future. Given the use of a perfusion agent to assess the area at risk, perfusion imaging must take place prospectively at the time of coronary occlusion and then following reperfusion, similar to SPECT with technetium‐based perfusion tracers. This presents obvious logistic difficulties when attempting to assess at‐risk myocardium at unpredictable times of patient presentation. Molecular echocardiographic techniques offer promise as a means of retrospectively imaging at‐risk myocardium following reperfusion in the setting of acute MI but to date have been limited to animal studies. In summary, current echocardiographic techniques for the assessment of at‐risk myocardium require unique expertise at specialized centers and are not universally available in routine clinical practice.
Nuclear Cardiology
The most widely used technique for directly evaluating at‐risk myocardium has been SPECT imaging with technetium‐99m (99mTc)‐based perfusion tracers administered both prior to and after revascularization of the IRA. 99mTc‐based radiotracers are used extensively in clinical practice for stress myocardial perfusion imaging and allow for high‐quality SPECT images given their distinct higher energy 140 keV photopeak and half‐life of 6 hours. 99mTc‐sestambi and 99mTc‐tetrofosmin are both lipophilic cationic complexes that passively diffuse into mitochondria. The uptake of these agents correlates closely with perfusion and cell viability. Unlike thallium, these agents remain fixed in the myocardium and undergo very minimal redistribution. Given these desirable characteristics, intravenous injection of technetium to assess at‐risk myocardium can take place at the time of coronary occlusion with imaging occurring up to 6 hours later, so as not to delay reperfusion therapy. Combined with an additional injection of technetium and SPECT imaging 1 to 2 weeks after revascularization (Figure 3), these images allow for quantitation of at‐risk myocardium (acute perfusion defect), final infarct size (final perfusion defect), and myocardial salvage (acute perfusion defect‐final perfusion defect). Thus, technetium‐based agents provide a significant and unique advantage when compared to other cardiovascular imaging techniques in that imaging can take place several hours after radioisotope injection. However, the SPECT images acquired remote from injection still represent a snapshot of myocardial perfusion at the time of injection.
Figure 3.
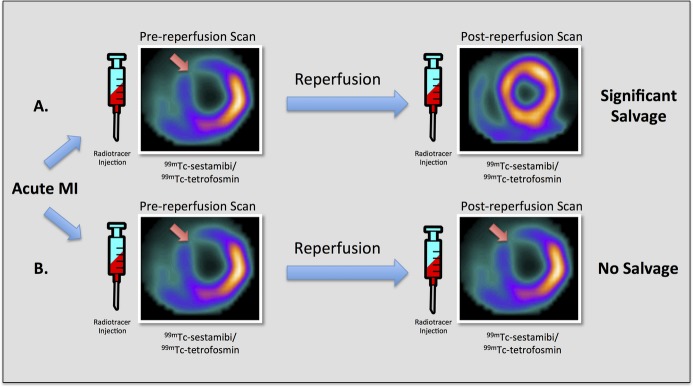
SPECT myocardial perfusion imaging for the assessment of at‐risk myocardium. Diagram depicting conventional technetium‐based SPECT myocardial perfusion imaging with 99mTc‐sestamibi/tetrofosmin for the assessment of myocardial salvage in 2 different hypothetical examples of acute ischemic myocardial injury in the left anterior descending (LAD) coronary artery territory. This technique requires 2 separate examinations with injection of radiotracer and imaging both before and after reperfusion. A, Pre‐reperfusion SPECT imaging reveals an area of decreased counts in the anteroseptum and anterior wall, whereas post‐reperfusion SPECT imaging shows normal myocardial perfusion. These findings suggest significant myocardial salvage in the left anterior descending coronary artery territory. B, Both pre‐reperfusion and postreperfusion SPECT images demonstrate decreased counts in the anteroseptum and anterior wall, suggesting no myocardial salvage in the left anterior descending coronary artery territory. 99mTc indicates technetium‐99m; MI, myocardial infarction; SPECT, single‐photon emission computed tomography.
Animal studies by Sinusas et al provided histopathologic validation that serial 99mTc‐sestambi autoradiography imaging during acute MI can delineate the myocardial area at risk during occlusion and subsequently assess the degree of myocardial salvage following reperfusion.21 Multiple clinical studies have since demonstrated the usefulness of 99mTc‐based tracers to quantify the myocardial area at risk.22–25 However, certain scenarios, including 3‐vessel coronary artery disease causing “balanced ischemia,” or perfusion defects attributed to non‐IRA related coronary artery stenoses may confound interpretation of at‐risk myocardium by perfusion techniques. Additionally, although clinically useful in providing a time‐sensitive depiction of myocardial perfusion at the time of tracer injection, this technique is limited in many ways by the need for 2 separate perfusion studies and the inherent difficulty of radioisotope administration before and after reperfusion. Given the need for prospective imaging at the unforeseeable times of patient presentation, techniques that allow retrospective delineation of the myocardial area at risk, area of infarction, and area of salvage offer significant clinical and research value and applicability.
Retrospective imaging methods are advantageous in that the imaging procedures may take place following reperfusion to assess both at‐risk and infarcted myocardium. Using gated myocardial perfusion imaging with SPECT, Romero‐Farina et al recently evaluated a series of patients with first acute MI by performing 99mTc‐tetrofosmin gated SPECT studies both prior to and then 1 month after infarction followed by revascularization. Through use of a multivariable regression equation, they found that analysis of perfusion and wall motion with a gated SPECT scan performed 1 month after revascularization for acute MI allowed for retrospective determination of at‐risk myocardium, infarcted myocardium, and salvaged myocardium. When compared with traditional nuclear assessment of myocardial salvage with a pre‐ and postreperfusion scan, the novel method provided moderate concordance with acceptable diagnostic power.26 In addition to offering the ability to noninvasively evaluate myocardial perfusion, nuclear imaging with radiolabeled glucose and fatty acid analogues permits characterization of myocardial metabolism in patients with recent myocardial ischemia. SPECT imaging with fatty acid agents, such as β‐methyl‐p‐[123I]‐iodophenyl‐pentadecanoic acid (123I‐BMIPP), theoretically offers the potential to image retrospectively after the time of reperfusion to evaluate the myocardial area at risk. The phenomenon of “ischemic memory” suggests that abnormal fatty acid metabolism persists in a region of at‐risk myocardium for ≤1 week following reperfusion. Thus, theoretically, one could perform nuclear perfusion and metabolic imaging in the early postreperfusion period to assess at‐risk myocardium (Figure 4). Indeed, Kawai et al evaluated 65 consecutive patients with acute MI, in which the patients received an injection of 99mTc‐tetrofosmin both prior to and late after percutaneous revascularization each followed by SPECT imaging, and an injection of 123I‐BMIPP with SPECT imaging performed ≈7 days after acute MI.27 They were able to demonstrate similar defect extent when 123I‐BMIPP performed 1 week after MI was compared with 99mTc‐tetrofosmin prior to revascularization, suggesting that 123I‐BMIPP performed in the subacute phase of MI can retrospectively identify areas of at‐risk myocardium. Although the exact persistence of abnormal fatty acid metabolism measured by 123I‐BMIPP in humans is unknown, there is preclinical data that may be useful in guiding image interpretation. In a rat model of acute ischemia and reperfusion, Higuchi et al showed that in the area at risk, 123I‐BMIPP uptake in comparison to thallium‐201 (201Tl) uptake was higher in the acute phase (20 minutes and day 1), lower in the subacute phase (day 7), and similar in the chronic phase (day 30).28 Results from this study suggest that the time after coronary occlusion significantly affects 123I‐BMIPP uptake in the area of at‐risk myocardium. Despite the promise of SPECT imaging with combined fatty acid and perfusion tracers for the assessment of at‐risk myocardium, these techniques remain limited by their relatively low spatial resolution, attenuation artifact, and radiation exposure. Furthermore, although 123I‐BMIPP has been used clinically in Japan and European countries for evaluating abnormalities in myocardial metabolism, use in the United States thus far has been limited to research studies aimed at early diagnosis of ACS, as the agent has not yet obtained FDA approval for clinical use.29
Figure 4.
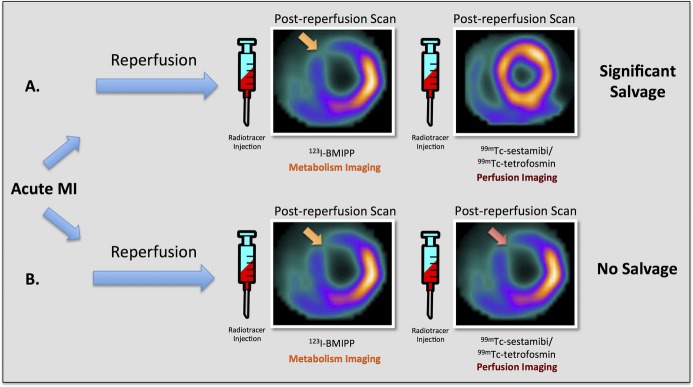
SPECT myocardial metabolism/perfusion imaging for the assessment of at‐risk myocardium. Diagram depicting combined fatty acid SPECT metabolic imaging with 123I‐BMIPP and technetium‐based SPECT perfusion imaging with 99mTc‐sestamibi/tetrofosmin for the assessment of myocardial salvage in 2 different hypothetical examples of acute ischemic myocardial injury in the left anterior descending (LAD) coronary artery territory. This technique requires injections of 2 separate radiotracers (123I‐BMIPP and 99mTc‐sestamibi/tetrofosmin) following reperfusion. A, Post‐reperfusion 123I‐BMIPP SPECT imaging reveals an area of decreased counts in the anteroseptum and anterior wall, whereas post‐reperfusion 99mTc‐sestamibi/tetrofosmin SPECT imaging shows normal myocardial perfusion. These findings suggest significant myocardial salvage in the left anterior descending coronary artery territory. B, Both post‐reperfusion 123I‐BMIPP SPECT metabolic imaging and post‐reperfusion 99mTc‐sestamibi/tetrofosmin perfusion SPECT imaging demonstrate decreased counts in the anteroseptum and anterior wall, suggesting no myocardial salvage in the left anterior descending coronary artery territory. 123I‐BMIPP indicates β‐methyl‐p‐[123I]‐iodophenyl‐pentadecanoic acid; 99mTc, technetium‐99m; MI, myocardial infarction; SPECT, single‐photon emission computed tomography.
Cardiac MRI
As a cardiovascular imaging modality, CMR has the unique ability to provide a comprehensive quantitative assessment of cardiac chamber size, ventricular mass and function, and myocardial tissue characteristics. In the setting of acute MI, CMR has been shown to differentiate among regions of myocardial necrosis, edema, hemorrhage, and microvascular obstruction through the use of various pulse sequences to aid in tissue characterization. As discussed above, multiple diagnostic and imaging methods that attempt to evaluate key pathophysiologic parameters in the setting of acute MI have been studied. However, only CMR, through the use of delayed‐enhancement cardiac MR (DE‐CMR) imaging, has been well validated such that the spatial extent and location of myocardial infarction matched in a 1:1 distribution when compared with histopathology in a large animal model.30 In addition, given its high spatial resolution, DE‐CMR has the ability to identify small subendocardial infarcts often missed by nuclear perfusion techniques, such that the transmural extent of infarction can reliably be assessed.31 In a large, international, multicenter trial, DE‐CMR was shown to be highly sensitive and accurate for detecting acute and chronic MI. In fact, this trial represents the initial and lone multicenter trial designed to study the detection and assessment of MI by a cardiovascular imaging method.32
As DE‐CMR is already widely recognized as the in vivo reference standard to delineate irreversible injury, a clinically robust CMR method to reliably assess at‐risk myocardium would be highly desirable. Whereas technetium‐based nuclear tracers used in SPECT imaging provide a time‐preserved view of myocardial perfusion at the time of tracer injection, which can then be imaged several hours later, CMR techniques using conventional gadolinium‐based contrast agents rely on a first‐pass assessment of myocardial perfusion and, therefore, differ in methods used for the evaluation of myocardial salvage. More than any other noninvasive imaging technique, CMR has garnered great interest and enthusiasm for its potential to retrospectively assess both the area of myocardial infarction and the area of at‐risk myocardium within 1 imaging session several days after the time of reperfusion.
CMR methods that aim to assess the myocardial area at risk have largely focused on 2 main techniques: the circumferential endocardial surface area (ESA) by DE‐CMR; and myocardial edema imaging by pre‐contrast T2‐weighted CMR (T2W‐CMR). Both of these techniques differ in methodology from previously employed SPECT and echo‐based myocardial perfusion techniques. Using these techniques, CMR may potentially overcome logistic difficulties posed by previously used perfusion techniques, which require radiotracer or contrast administration as well as imaging both before and after the time of reperfusion.
Some investigators have used the circumferential extent of infarction as a relatively simple method to measure at‐risk myocardium by defining the transmural projection of the lateral borders of the infarct by DE‐CMR as the myocardial area at risk. The rationale behind this technique is based on the original pathology experiments of Reimer and Jennings, in which they postulate the absence of a circumferential wavefront of perfusion in a coronary artery territory, as there is no perfusion gradient at the lateral borders of the infarct.1 The lateral borders of infarction are established shortly after coronary occlusion and are not appreciably affected by collateral flow. Ortiz‐Perez et al initially demonstrated that the region of at‐risk myocardium can be measured through the use of DE‐CMR images by quantifying the left ventricular (LV) endocardial border of hyperenhancement as a percentage of total LV endocardial surface area.33 Then they evaluated the modified APPROACH and BARI angiographic risk scores by using the ESA of myocardial infarction in patients with transmural infarction on DE‐CMR images to validate these scores. They found that the use of both an angiographic risk score in combination with DE‐CMR provides a method to estimate myocardial salvage. While the ESA‐CMR method has potential in patients with a greater transmural extent of infarction, this technique may not accurately assess at‐risk myocardium in patients presenting early after coronary artery occlusion with little to no myocardial necrosis.
In clinical research and practice today, however, the most prevalent of the 2 CMR techniques to assess myocardial salvage involves measuring myocardial edema, largely through the use of pre‐contrast dark‐blood T2 weighted (T2W) CMR imaging techniques. Myocardial injury results in an increase in myocardial water content, which can be detected by T2W‐CMR as hyperintensity within the edematous zone. The hyperintense region by precontrast T2W‐CMR has been hypothesized by some investigators to represent the myocardial area at risk, and in combination with assessment of infarction by DE‐CMR, is thought to offer a method for the comprehensive quantitative assessment of reversibly and irreversibly injured myocardium within a single cardiac imaging examination.
Several early and important large‐animal studies are often cited as evidence that T2W‐CMR imaging of edema can define at‐risk myocardium after both reperfused and nonreperfused MI.34–36 However, it should be noted that these studies were small and carry limitations. In particular, many of the findings from these studies were based on comparisons to inadequate pathologic reference standards or measured against alternative CMR imaging techniques as an indirect reference standard. Despite significant enthusiasm for T2W‐CMR imaging as a measure of the myocardial area at risk, there is a lack of validation studies, which undeniably demonstrates that the area of hyperintensity by T2W‐CMR imaging matches the spatial extent and location of at‐risk myocardium in a 1:1 distribution when compared with histopathology by microspheres. Although also small and not without their own limitations, other early large‐animal studies of both reperfused and nonreperfused MI suggest that T2W‐CMR may, in fact, identify the area of myocardial infarction rather than the area of at‐risk myocardium.37–39 The conclusions from these studies bring to light that the temporal evolution of MI is highly fluid and complex. In addition to indexing myocardial edema, T2W‐CMR imaging reflects other pathophysiologic processes associated with MI, including inflammation, hemorrhage, and microvascular obstruction. Thus, uncertainty still remains as to what pathophysiology is truly reflected by the area of hyperintensity on T2W‐CMR following STEMI.
In addition to the lack of a pathologic reference standard, several limitations exist with the use of conventional dark‐blood T2W‐CMR techniques, including turbo spin echo (TSE) and short tau inversion recovery (STIR), which are among the most common and widely used T2W‐CMR techniques to assess myocardial edema in clinical practice today. Conventional dark‐blood T2W‐CMR often suffers from artifactual signal loss secondary to cardiac motion, which results in poor image homogeneity and can confound interpretation (Figure 5).40 The most widely recognized mechanism of signal loss is thought to be due to misalignment of the dark‐blood preparation with readout, which can occur during arrhythmia, with an ectopic beat, or with significant variation in the cardiac cycle. However, motion affecting the readout itself may also result in additional signal loss. Additionally, regions of slow flow, which occur adjacent to regions of acute myocardial injury, can result in hyperintense signal on conventional dark‐blood T2W‐CMR that may be mistaken for myocardial edema. Furthermore, the increase in T2 signal between normal and edematous but noninfarcted myocardium is small, rendering a low contrast‐to‐noise ratio between abnormal and normal myocardium.41 Thus, routine clinical interpretation of edema versus image artifact can be challenging.
Figure 5.
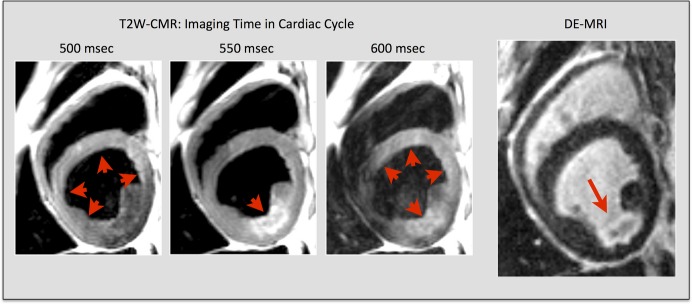
Technical issues with T2‐weighted CMR. Technical limitations with conventional dark‐blood T2W‐CMR. Images taken from a subject with myocardial infarction in the left circumflex coronary artery territory. Red arrowheads indicate areas of myocardium with high signal by T2W‐CMR. The red arrow indicates a subendocardial lateral wall infarct on corresponding DE‐CMR image at the same slice location. Note that the regional myocardial signal intensity varies significantly with small changes in the acquisition time of the cardiac cycle. (Adapted and reprinted, with permission, from reference no. 40.) DE‐CMR indicates delayed‐enhancement cardiac magnetic resonance; MRI, magnetic resonance imaging; T2W‐CMR, T2‐weighted cardiac magnetic resonance.
Newer, bright‐blood T2W‐CMR and T2 mapping techniques, which attempt to reduce such artifacts and improve image quality, have been developed.41–44 However, these techniques are not universally available through all vendors and have yet to be validated against a pathologic reference standard. Technical limitations related to T2 mapping, including misregistration and reduced spatial resolution, may result in partial volume averaging and confound image interpretation. In addition to limitations related to image quality, prognostic studies looking at myocardial salvage have largely been based on conventional dark‐blood T2W‐CMR and have not used these newer techniques. Therefore, the overall prognostic value of these novel techniques has not been studied and remains unknown.
There is prior evidence to confirm that CMR has the ability to accurately differentiate areas of acute from chronic myocardial injury through the use of T2W‐CMR techniques to image myocardial edema.45 This information provides clinical value when one is trying to determine the acuity of myocardial injury in patients with ischemic heart disease. What remains unclear is whether or not the region of myocardial edema in the period surrounding acute myocardial injury secondary to coronary artery occlusion accurately delineates the myocardial area at risk. Differing viewpoints are held and significant controversy exists among various research groups regarding the utility of T2W‐CMR. Several pro/con commentaries have recently been published, which provide a critical and comprehensive analysis of the physiologic and technical aspects of T2W‐CMR with arguments both for and against the widespread use of T2W‐CMR for the assessment of at‐risk myocardium in the setting of acute MI.46–48 Additional study and research is clearly needed, including unequivocal validation studies analogous to those performed to image myocardial infarction with DE‐CMR, in order to provide clarity to this scientific conundrum.
Several groups have attempted to compare the 2 most common CMR techniques for assessing at‐risk myocardium. However, results from prior studies comparing these techniques are, by and large, inconsistent in their findings. In a study of 37 patients with acute reperfused STEMI, Ubachs et al found that ESA provided lower estimates of at‐risk myocardium and correlated poorly when compared to T2W‐CMR as a reference standard, whereas Wright et al found that there was a favorable correlation between the 2 methods in a similar cohort of patients.49–50 More recently, Fuernau et al compared T2W‐CMR and ESA‐CMR to the APPROACH score for the assessment of at‐risk myocardium and found that T2W‐CMR showed a better correlation with the angiographic risk score when compared with the ESA‐CMR method.51 The ESA‐CMR method performed less favorably in cases with little to no evidence of myocardial necrosis. Unfortunately, these studies provide comparative information between different CMR techniques by using CMR measures or angiographic risk scores as indirect reference standards. In an attempt to provide a greater degree of clarity, Versteylen et al evaluated 78 patients with acute STEMI using angiographic (BARI and APPROACH), electrocardiographic (Aldrich), and CMR (T2W‐CMR and ESA‐CMR) methods to quantify at‐risk myocardium.52 They ranked each technique from worst to best according to how well each technique agreed with important and established pathophysiologic concepts derived from original work by Reimer and Jennings. In general, they found that CMR techniques agreed best with these concepts, followed by angiographic methods, and finally, the electrocardiographic method. Between the 2 CMR techniques, the ESA‐CMR method performed better than T2W‐CMR.
Both T2W‐ and ESA‐CMR techniques have attracted significant interest for their potential to noninvasively define the myocardial area at risk, so much so, that these methods have provided the basis for clinical decision‐making as well as surrogate endpoints in the design of large clinical trials to assess at‐risk myocardium and response to therapy in patients with acute MI.9,53–55 However, the rudimentary question of whether or not currently used CMR methods accurately reflect a validated pathologic reference standard for the assessment of at‐risk myocardium remains elusive and without a definitive answer at present. Prior to continued widespread adoption, CMR techniques deserve further careful study to validate their routine clinical use for the assessment of at‐risk myocardium.
Cardiac CT
Cardiac CT is widely recognized for its ability to noninvasively evaluate the coronary arteries given its superior spatial resolution and speed of image acquisition. Some have advocated the use of cardiac CT to assess at‐risk myocardium by defining risk scores similar to those developed for coronary angiography.56 In addition to delineating coronary arterial anatomy, the utility of cardiac CT to noninvasively define myocardial tissue characteristics, including both edematous and infarcted myocardium, has been demonstrated (Figure 6). Several cardiac CT techniques, including imaging of hypoperfusion as assessed by arterial phase cardiac CT and delayed myocardial contrast enhancement CT, have been used to image myocardial infarction. Data regarding CT imaging of myocardial edema in vivo, however, have been sparse. In theory, increased myocardial water content should correspond to reduced attenuation values on non‐contrast enhanced CT. Mahnken et al used a porcine model of acute reperfused myocardial infarction to compare unenhanced, arterial, and late‐phase dual source CT with T2W‐CMR and DE‐CMR.57 Substantial agreement was reported when comparing late‐phase CT and delayed enhancement CMR with TTC staining as well as when comparing unenhanced dual source CT with T2W‐CMR. It should be noted, however, that MI was transmural on all sections in this study, and the utility of the technique in the assessment of smaller subendocardial infarcts is not known.
Figure 6.
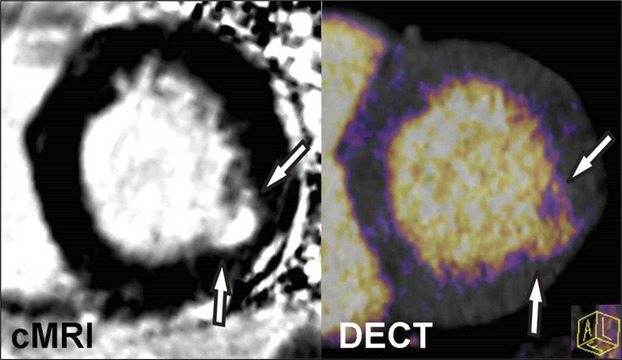
Cardiac magnetic resonance imaging (cMRI) and dual‐energy computed tomography (DECT) imaging of myocardial infarction. Iodine color map reconstructed from a DECT image demonstrates good agreement when compared with delayed‐enhancement cMRI of a subject with prior myocardial infarction of the lateral wall. Similar to cMRI, DECT offers the potential to assess myocardial infarction as well as myocardial salvage through the use of pre‐ and postcontrast techniques.
More recently, Mewton et al compared several techniques for evaluating at‐risk myocardium in a porcine model of acute reperfused MI.58 They performed post‐reperfusion CMR techniques, including ESA‐CMR, dark‐blood T2W‐CMR, and bright‐blood T2W‐CMR, as well as pre‐reperfusion contrast‐enhanced arterial phase CT imaging and compared these techniques with a pathology reference standard. Interestingly, their findings suggested that postreperfusion CMR techniques by and large overestimated the region of at‐risk myocardium when compared to a pathologic reference standard. They found that pre‐reperfusion arterial enhanced CT performed during coronary occlusion exhibited the greatest accuracy when compared to pathology. A pre‐reperfusion CMR perfusion technique during coronary occlusion was not evaluated.
In the setting of acute MI, pre‐reperfusion arterial enhanced CT imaging would obviously delay time to reperfusion and extend door‐to‐balloon time, possibly leading to worse patient outcomes. However, there has been data showing that CT can be performed expeditiously in experienced centers. In a study evaluating the use of CT to differentiate coronary reperfusion during acute MI, Yamashita et al were able to show that CT could be performed in 87 patients with a mean time elapsed before coronary intervention due to cardiac CT scanning of 20±3 minutes.59 Still, many clinicians share the sentiment that any delay in reperfusion is unacceptable and in opposition to current standard of care. With the widespread and increasing availability of CT, including the potential for CT integration into cardiac catheterization laboratories, such strategies may become more feasible in clinical practice, as cardiac CT scanning could be performed rapidly at the time of catheterization.
At present, none of the described cardiac CT techniques are used clinically or have been evaluated as surrogate endpoints in large clinical trials. From a technical standpoint, the pathophysiological basis for myocardial edema representing the myocardial area at risk has not yet been sufficiently validated with histopathology using any postreperfusion imaging modality, including cardiac CT. Thus, postreperfusion edema imaging with cardiac CT faces challenges similar to those described above for cardiac MRI. Recent data suggest that pre‐reperfusion contrast‐enhanced cardiac CT may provide enhanced accuracy for rapidly defining at‐risk myocardium. Although promising, barriers to implementation of pre‐reperfusion cardiac CT in the clinical setting at present are complex and revolve around the quandary of whether time to reperfusion should be delayed in order to assess at‐risk myocardium.
Conclusion
Accurate, reproducible, logistically feasible, and well‐validated cardiovascular imaging methods to assess at‐risk myocardium have been coveted among clinicians and investigators, both for their ability to assist in clinical decision‐making as well as for their ability to assess therapeutic response in the setting of acute MI. Multiple cardiovascular diagnostic and imaging tests have been used to quantify at‐risk myocardium over the last several decades. Although clinically useful, ECG and coronary angiography measures of at‐risk myocardium have by and large been less reliable techniques, as they only indirectly estimate at‐risk myocardium. Contrast echocardiography and nuclear imaging techniques evaluating perfusion gained prominence in the 1990s but have lost momentum given the challenge of prospective imaging at the unforeseen time of patient presentation. More recently, investigators have suggested that nuclear imaging and CMR may offer the potential for retrospective imaging of at‐risk myocardium after the time of reperfusion. However, limitations in radioisotope availability and technical issues related to T2W‐CMR remain as obstacles to routine clinical use. With the ever‐increasing and more instantaneous availability of cardiac CT, pre‐reperfusion arterial phase cardiac CT imaging may offer a way to point‐of‐care assessment of at‐risk myocardium at the time of patient presentation without appreciably delaying time to reperfusion.
In conclusion, there is great promise that cardiovascular imaging methods will offer clinicians and investigators robust methods to identify at‐risk myocardium in vivo in order to guide effective clinical decision‐making and improve therapeutic efficacy for the treatment of acute MI. However, despite a rapidly evolving body of literature, fundamental questions remain unanswered regarding the ability of various cardiovascular imaging techniques to adequately reflect the underlying pathophysiology of acute MI. Therefore, caution should be advised prior to the routine adoption of the latest novel imaging techniques, and the importance of well‐performed validation studies with an established pathologic reference standard should not be understated.
Disclosures
Dr Schoepf is a consultant for and receives research support from Bayer‐Schering, Bracco, General Electric, MEDRAD, and Siemens. The other authors have no conflict of interest to disclose.
References
- 1.Reimer KA, Jennings RB. The “wavefront phenomenon” of myocardial ischemic cell death. II. Transmural progression of necrosis within the framework of ischemic bed size (myocardium at risk) and collateral flow. Lab Invest. 1979; 40:633-644 [PubMed] [Google Scholar]
- 2.Reimer KA, Lowe JE, Rasmussen MM, Jennings RB. The wavefront phenomenon of ischemic cell death. 1. Myocardial infarct size vs duration of coronary occlusion in dogs. Circulation. 1977; 56:786-794 [DOI] [PubMed] [Google Scholar]
- 3.Kim RJ, Wu E, Rafael A, Chen EL, Parker MA, Simonetti O, Klocke FJ, Bonow RO, Judd RM. The use of contrast‐enhanced magnetic resonance imaging to identify reversible myocardial dysfunction. N Engl J Med. 2000; 343:1445-1453 [DOI] [PubMed] [Google Scholar]
- 4.Choi KM, Kim RJ, Gubernikoff G, Vargas JD, Parker M, Judd RM. Transmural extent of acute myocardial infarction predicts long‐term improvement in contractile function. Circulation. 2001; 104:1101-1107 [DOI] [PubMed] [Google Scholar]
- 5.Burns RJ, Gibbons RJ, Yi Q, Roberts RS, Miller TD, Schaer GL, Anderson JL, Yusuf S. The relationships of left ventricular ejection fraction, end‐systolic volume index and infarct size to six‐month mortality after hospital discharge following myocardial infarction treated by thrombolysis. J Am Coll Cardiol. 2002; 39:30-36 [DOI] [PubMed] [Google Scholar]
- 6.Ross AM, Gibbons RJ, Stone GW, Kloner RA, Alexander RW. A randomized, double‐blinded, placebo‐controlled multicenter trial of adenosine as an adjunct to reperfusion in the treatment of acute myocardial infarction (AMISTAD‐II). J Am Coll Cardiol. 2005; 45:1775-1780 [DOI] [PubMed] [Google Scholar]
- 7.Gibbons RJ, Miller TD, Christian TF. Infarct size measured by single photon emission computed tomographic imaging with (99m)Tc‐sestamibi: a measure of the efficacy of therapy in acute myocardial infarction. Circulation. 2000; 101:101-108 [DOI] [PubMed] [Google Scholar]
- 8.Kastrati A, Mehilli J, Dirschinger J, Schricke U, Neverve J, Pache J, Martinoff S, Neumann FJ, Nekolla S, Blasini R, Seyfarth M, Schwaiger M, Schömig A. Myocardial salvage after coronary stenting plus abciximab versus fibrinolysis plus abciximab in patients with acute myocardial infarction: a randomised trial. Lancet. 2002; 359:920-925 [DOI] [PubMed] [Google Scholar]
- 9.Eitel I, Desch S, Fuernau G, Hildebrand L, Gutberlet M, Schuler G, Thiele H. Prognostic significance and determinants of myocardial salvage assessed by cardiovascular magnetic resonance in acute reperfused myocardial infarction. J Am Coll Cardiol. 2010; 55:2470-2479 [DOI] [PubMed] [Google Scholar]
- 10.Aldrich HR, Wagner NB, Boswick J, Corsa AT, Jones MG, Grande P, Lee KL, Wagner GS. Use of initial ST‐segment deviation for prediction of final electrocardiographic size of acute myocardial infarcts. Am J Cardiol. 1988; 61:749-753 [DOI] [PubMed] [Google Scholar]
- 11.Wilkins ML, Maynard C, Annex BH, Clemmensen P, Elias WJ, Gibson RS, Lee KL, Pryor AD, Selker H, Turner J, Weaver WD, Anderson ST, Wagner GS. Admission prediction of expected final myocardial infarct size using weighted ST‐segment, Q wave, and T wave measurements. J Electrocardiol. 1997; 30:1-7 [DOI] [PubMed] [Google Scholar]
- 12.Christian TF, Gibbons RJ, Clements IP, Berger PB, Selvester RH, Wagner GS. Estimates of myocardium at risk and collateral flow in acute myocardial infarction using electrocardiographic indexes with comparison to radionuclide and angiographic measures. J Am Coll Cardiol. 1995; 26:388-393 [DOI] [PubMed] [Google Scholar]
- 13.Dash H, Johnson RA, Dinsmore RE, Harthorne JW. Cardiomyopathic syndrome due to coronary artery disease. I: relation to angiographic extent of coronary disease and to remote myocardial infarction. Br Heart J. 1977; 39:733-739 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Alderman EL, Stadius M. The angiographic definitions of the Bypass Angioplasty Revascularization Investigation. Coron Artery Dis. 1992; 3:1189-1208 [Google Scholar]
- 15.Graham MM, Faris PD, Ghali WA, Galbraith PD, Norris CM, Badry JT, Mitchell LB, Curtis MJ, Knudtson ML. Validation of three myocardial jeopardy scores in a population‐based cardiac catheterization cohort. Am Heart J. 2001; 142:254-261 [DOI] [PubMed] [Google Scholar]
- 16.Kaul S, Pandian NG, Okada RD, Pohost GM, Weyman AE. Contrast echocardiography in acute myocardial ischemia: I. In vivo determination of total left ventricular “area at risk”. J Am Coll Cardiol. 1984; 4:1272-1282 [DOI] [PubMed] [Google Scholar]
- 17.Ito H, Tomooka T, Sakai N, Yu H, Higashino Y, Fujii K, Masuyama T, Kitabatake A, Minamino T. Lack of myocardial perfusion immediately after successful thrombolysis. A predictor of poor recovery of left ventricular function in anterior myocardial infarction. Circulation. 1992; 85:1699-1705 [DOI] [PubMed] [Google Scholar]
- 18.Villanueva FS, Glasheen WP, Sklenar J, Kaul S. Assessment of risk area during coronary occlusion and infarct size after reperfusion with myocardial contrast echocardiography using left and right atrial injections of contrast. Circulation. 1993; 88:596-604 [DOI] [PubMed] [Google Scholar]
- 19.Lindner JR, Villanueva FS, Dent JM, Wei K, Sklenar J, Kaul S. Assessment of resting perfusion with myocardial contrast echocardiography: theoretical and practical considerations. Am Heart J. 2000; 139:231-240 [PubMed] [Google Scholar]
- 20.Villanueva FS, Lu E, Bowry S, Kilic S, Tom E, Wang J, Gretton J, Pacella JJ, Wagner WR. Myocardial ischemic memory imaging with molecular echocardiography. Circulation. 2007; 115:345-352 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Sinusas AJ, Trautman KA, Bergin JD, Watson DD, Ruiz M, Smith WH, Beller GA. Quantification of area at risk during coronary occlusion and degree of myocardial salvage after reperfusion with technetium‐99m methoxyisobutyl isonitrile. Circulation. 1990; 82:1424-1437 [DOI] [PubMed] [Google Scholar]
- 22.Gibbons RJ, Verani MS, Behrenbeck T, Pellikka PA, O'Connor MK, Mahmarian JJ, Chesebro JH, Wackers FJ. Feasibility of tomographic 99mTc‐hexakis‐2‐methoxy‐2‐methylpropyl‐isonitrile imaging for the assessment of myocardial area at risk and the effect of treatment in acute myocardial infarction. Circulation. 1989; 80:1277-1286 [DOI] [PubMed] [Google Scholar]
- 23.Behrenbeck T, Pellikka PA, Huber KC, Bresnahan JF, Gersh BJ, Gibbons RJ. Primary angioplasty in myocardial infarction: assessment of improved myocardial perfusion with technetium‐99m isonitrile. J Am Coll Cardiol. 1991; 17:365-372 [DOI] [PubMed] [Google Scholar]
- 24.Santoro GM, Bisi G, Sciagrà R, Leoncini M, Fazzini PF, Meldolesi U. Single photon emission computed tomography with technetium‐99m hexakis 2‐methoxyisobutyl isonitrile in acute myocardial infarction before and after thrombolytic treatment: assessment of salvaged myocardium and prediction of late functional recovery. J Am Coll Cardiol. 1990; 15:301-314 [DOI] [PubMed] [Google Scholar]
- 25.Gibbons RJ, Christian TF, Hopfenspirger M, Hodge DO, Bailey KR. Myocardium at risk and infarct size after thrombolytic therapy for acute myocardial infarction: implications for the design of randomized trials of acute intervention. J Am Coll Cardiol. 1994; 24:616-623 [DOI] [PubMed] [Google Scholar]
- 26.Romero‐Farina G, Aguade‐Bruix S, Candell‐Riera J, Pizzi MN, Pineda V, Figueras J, Cuberas G, De Leon G, Castell‐Conesa J, Garcia‐Dorado D. Acute myocardial infarction: estimation of at‐risk and salvaged myocardium at myocardial perfusion SPECT 1 month after infarction. Radiology. 2013; 269:577-584 [DOI] [PubMed] [Google Scholar]
- 27.Kawai Y, Tsukamoto E, Nozaki Y, Kishino K, Kohya T, Tamaki N. Use of 123I‐BMIPP single‐photon emission tomography to estimate areas at risk following successful revascularization in patients with acute myocardial infarction. Eur J Nucl Med. 1998; 25:1390-1395 [DOI] [PubMed] [Google Scholar]
- 28.Higuchi T, Taki J, Nakajima K, Kinuya S, Namura M, Tonami N. Time course of discordant BMIPP and thallium uptake after ischemia and reperfusion in a rat model. J Nucl Med. 2005; 46:172-175 [PubMed] [Google Scholar]
- 29.Kontos MC, Dilsizian V, Weiland F, DePuey G, Mahmarian JJ, Iskandrian AE, Bateman TM, Heller GV, Ananthasubramaniam K, Li Y, Goldman JL, Armor T, Kacena KA, LaFrance ND, Garcia EV, Babich JW, Udelson JE. Iodofiltic acid I 123 (BMIPP) fatty acid imaging improves initial diagnosis in emergency department patients with suspected acute coronary syndromes: a multicenter trial. J Am Coll Cardiol. 2010; 56:290-299 [DOI] [PubMed] [Google Scholar]
- 30.Kim RJ, Fieno DS, Parrish TB, Harris K, Chen EL, Simonetti O, Bundy J, Finn JP, Klocke FJ, Judd RM. Relationship of MRI delayed contrast enhancement to irreversible injury, infarct age, and contractile function. Circulation. 1999; 100:1992-2002 [DOI] [PubMed] [Google Scholar]
- 31.Wagner A, Mahrholdt H, Holly TA, Elliott MD, Regenfus M, Parker M, Klocke FJ, Bonow RO, Kim RJ, Judd RM. Contrast‐enhanced MRI and routine single photon emission computed tomography (SPECT) perfusion imaging for detection of subendocardial myocardial infarcts: an imaging study. Lancet. 2003; 361:374-379 [DOI] [PubMed] [Google Scholar]
- 32.Kim RJ, Albert TSE, Wible JH, Elliott MD, Allen JC, Lee JC, Parker M, Napoli A, Judd RM. Performance of delayed‐enhancement magnetic resonance imaging with gadoversetamide contrast for the detection and assessment of myocardial infarction: an international, multicenter, double‐blinded, randomized trial. Circulation. 2008; 117:629-637 [DOI] [PubMed] [Google Scholar]
- 33.Ortiz‐Pérez JT, Meyers SN, Lee DC, Kansal P, Klocke FJ, Holly TA, Davidson CJ, Bonow RO, Wu E. Angiographic estimates of myocardium at risk during acute myocardial infarction: validation study using cardiac magnetic resonance imaging. Eur Heart J. 2007; 28:1750-1758 [DOI] [PubMed] [Google Scholar]
- 34.García‐Dorado D, Oliveras J, Gili J, Sanz E, Pérez‐Villa F, Barrabés J, Carreras MJ, Solares J, Soler‐Soler J. Analysis of myocardial oedema by magnetic resonance imaging early after coronary artery occlusion with or without reperfusion. Cardiovasc Res. 1993; 27:1462-1469 [DOI] [PubMed] [Google Scholar]
- 35.Aletras AH, Tilak GS, Natanzon A, Hsu L‐Y, Gonzalez FM, Hoyt RF, Arai AE. Retrospective determination of the area at risk for reperfused acute myocardial infarction with T2‐weighted cardiac magnetic resonance imaging: histopathological and displacement encoding with stimulated echoes (DENSE) functional validations. Circulation. 2006; 113:1865-1870 [DOI] [PubMed] [Google Scholar]
- 36.Tilak GS, Hsu L, Hoyt RF, Arai AE, Aletras AH. In vivo T2‐weighted magnetic resonance imaging can accurately determine the ischemic area at risk for 2‐day‐old nonreperfused myocardial infarction. Invest Radiol. 2008; 43:7-15 [DOI] [PubMed] [Google Scholar]
- 37.Ryan T, Tarver RD, Duerk JL, Sawada SG, Hollenkamp NC. Distinguishing viable from infarcted myocardium after experimental ischemia and reperfusion by using nuclear magnetic resonance imaging. J Am Coll Cardiol. 1990; 15:1355-1364 [DOI] [PubMed] [Google Scholar]
- 38.Johnston DL, Brady TJ, Ratner AV, Rosen BR, Newell JB, Pohost GM, Okada RD. Assessment of myocardial ischemia with proton magnetic resonance: effects of a three hour coronary occlusion with and without reperfusion. Circulation. 1985; 71:595-601 [DOI] [PubMed] [Google Scholar]
- 39.Miller DD, Johnston DL, Dragotakes D, Newell JB, Aretz T, Kantor HL, Brady TJ, Okada RD. Effect of hyperosmotic mannitol on magnetic resonance relaxation parameters in reperfused canine myocardial infarction. Magn Reson Imaging. 1989; 7:79-88 [DOI] [PubMed] [Google Scholar]
- 40.Wince WB, Kim RJ. Molecular imaging: T2‐weighted CMR of the area at risk—a risky business? Nat Rev Cardiol. 2010; 7:547-549 [DOI] [PubMed] [Google Scholar]
- 41.Kellman P, Aletras AH, Mancini C, McVeigh ER, Arai AE. T2‐prepared SSFP improves diagnostic confidence in edema imaging in acute myocardial infarction compared to turbo spin echo. Magn Reson Med. 2007; 57:891-897 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Aletras AH, Kellman P, Derbyshire JA, Arai AE. ACUT2E TSE‐SSFP: a hybrid method for T2‐weighted imaging of edema in the heart. Magn Reson Med. 2008; 59:229-235 [DOI] [PubMed] [Google Scholar]
- 43.Giri S, Chung Y‐C, Merchant A, Mihai G, Rajagopalan S, Raman SV, Simonetti OP. T2 quantification for improved detection of myocardial edema. J Cardiovasc Magn Reson. 2009; 11:56. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Verhaert D, Thavendiranathan P, Giri S, Mihai G, Rajagopalan S, Simonetti OP, Raman SV. Direct T2 quantification of myocardial edema in acute ischemic injury. JACC Cardiovasc Imaging. 2011; 4:269-278 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Abdel‐Aty H, Zagrosek A, Schulz‐Menger J, Taylor AJ, Messroghli D, Kumar A, Gross M, Dietz R, Friedrich MG. Delayed enhancement and T2‐weighted cardiovascular magnetic resonance imaging differentiate acute from chronic myocardial infarction. Circulation. 2004; 109:2411-2416 [DOI] [PubMed] [Google Scholar]
- 46.Friedrich MG, Kim HW, Kim RJ. T2‐weighted imaging to assess post‐infarct myocardium at risk. JACC Cardiovasc Imaging. 2011; 4:1014-1021 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Arai AE, Leung S, Kellman P. Controversies in cardiovascular MR imaging: reasons why imaging myocardial T2 has clinical and pathophysiologic value in acute myocardial infarction. Radiology. 2012; 265:23-32 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Croisille P, Kim HW, Kim RJ. Controversies in cardiovascular MR imaging: T2‐weighted imaging should not be used to delineate the area at risk in ischemic myocardial injury. Radiology. 2012; 265:12-22 [DOI] [PubMed] [Google Scholar]
- 49.Ubachs JFA, Engblom H, Erlinge D, Jovinge S, Hedström E, Carlsson M, Arheden H. Cardiovascular magnetic resonance of the myocardium at risk in acute reperfused myocardial infarction: comparison of T2‐weighted imaging versus the circumferential endocardial extent of late gadolinium enhancement with transmural projection. J Cardiovasc Magn Reson. 2010; 12:18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Wright J, Adriaenssens T, Dymarkowski S, Desmet W, Bogaert J. Quantification of myocardial area at risk with T2‐weighted CMR: comparison with contrast‐enhanced CMR and coronary angiography. JACC Cardiovasc Imaging. 2009; 2:825-831 [DOI] [PubMed] [Google Scholar]
- 51.Fuernau G, Eitel I, Franke V, Hildebrandt L, Meissner J, de Waha S, Lurz P, Gutberlet M, Desch S, Schuler G, Thiele H. Myocardium at risk in ST‐segment elevation myocardial infarction comparison of T2‐weighted edema imaging with the MR‐assessed endocardial surface area and validation against angiographic scoring. JACC Cardiovasc Imaging. 2011; 4:967-976 [DOI] [PubMed] [Google Scholar]
- 52.Versteylen MO, Bekkers SCAM, Smulders MW, Winkens B, Mihl C, Winkens MHM, Leiner T, Waltenberger JL, Kim RJ, Gorgels APM. Performance of angiographic, electrocardiographic and MRI methods to assess the area at risk in acute myocardial infarction. Heart. 2012; 98:109-115 [DOI] [PubMed] [Google Scholar]
- 53.Larose E, Rodés‐Cabau J, Pibarot P, Rinfret S, Proulx G, Nguyen CM, Déry JP, Gleeton O, Roy L, Noël B, Barbeau G, Rouleau J, Boudreault JR, Amyot M, De Larochellière R, Bertrand OF. Predicting late myocardial recovery and outcomes in the early hours of ST‐segment elevation myocardial infarction traditional measures compared with microvascular obstruction, salvaged myocardium, and necrosis characteristics by cardiovascular magnetic resonance. J Am Coll Cardiol. 2010; 55:2459-2469 [DOI] [PubMed] [Google Scholar]
- 54.Thiele H, Hildebrand L, Schirdewahn C, Eitel I, Adams V, Fuernau G, Erbs S, Linke A, Diederich K‐W, Nowak M, Desch S, Gutberlet M, Schuler G. Impact of high‐dose N‐acetylcysteine versus placebo on contrast‐induced nephropathy and myocardial reperfusion injury in unselected patients with ST‐segment elevation myocardial infarction undergoing primary percutaneous coronary intervention. The LIPSIA‐N‐ACC (Prospective, Single‐Blind, Placebo‐Controlled, Randomized Leipzig Immediate PercutaneouS Coronary Intervention Acute Myocardial Infarction N‐ACC) Trial. J Am Coll Cardiol. 2010; 55:2201-2209 [DOI] [PubMed] [Google Scholar]
- 55.Lønborg J, Kelbaek H, Vejlstrup N, Jørgensen E, Helqvist S, Saunamäki K, Clemmensen P, Holmvang L, Treiman M, Jensen JS, Engstrøm T. Cardioprotective effects of ischemic postconditioning in patients treated with primary percutaneous coronary intervention, evaluated by magnetic resonance. Circ Cardiovasc Interv. 2010; 3:34-41 [DOI] [PubMed] [Google Scholar]
- 56.Chiou K‐R, Peng N‐J, Hsiao S‐H, Huang Y‐L, Cheng C‐C, Pan H‐B, Wu M‐T. CT of coronary heart disease: Part 2, Dual‐phase MDCT evaluates late symptom recurrence in ST‐segment elevation myocardial infarction patients after revascularization. AJR Am J Roentgenol. 2012; 198:548-562 [DOI] [PubMed] [Google Scholar]
- 57.Mahnken AH, Bruners P, Bornikoel CM, Krämer N, Guenther RW. Assessment of myocardial edema by computed tomography in myocardial infarction. JACC Cardiovasc Imaging. 2009; 2:1167-1174 [DOI] [PubMed] [Google Scholar]
- 58.Mewton N, Rapacchi S, Augeul L, Ferrera R, Loufouat J, Boussel L, Micolich A, Rioufol G, Revel D, Ovize M, Croisille P. Determination of the myocardial area at risk with pre‐ versus post‐reperfusion imaging techniques in the pig model. Basic Res Cardiol. 2011; 106:1247-1257 [DOI] [PubMed] [Google Scholar]
- 59.Yamashita M, Lee S, Hamasaki S, Nishimoto T, Kajiya T, Toyonaga K, Arima R, Toda H, Ohba I, Otsuji Y, Tei C. Noninvasive evaluation of coronary reperfusion by CT angiography in patients with STEMI. JACC Cardiovasc Imaging. 2011; 4:141-149 [DOI] [PubMed] [Google Scholar]