

Abstract
Pancreatic cystic lesions (PCL) may be incidentally detected in up to 13.5% of patients. These represent a wide variety of lesions including mucinous cysts [intraductal papillary mucinous neoplasms (IPMN) and mucinous cystic neoplasms (MCN)] that have malignant potential. The difficulty in identifying the various PCL and their unpredictable potential for malignant degeneration makes their management cumbersome. The current diagnostic evaluation of PCL often includes EUS-guided fine needle aspiration (EUS-FNA) for cyst fluid analysis. Cyst fluid can be analyzed for tumor markers, cytology, mucins, DNA analysis and amylase. Pancreatic cyst CEA level is considered the most accurate tumor marker for diagnosing mucinous cysts. Approximately 0.2 to 1.0 mL of cyst fluid is required to run the test and a cut-off of 192 ng/ mL can be expected to capture ~75% of mucinous cysts. The presence of a KRAS mutation is very specific for a mucinous cyst but lacks sensitivity. Cytology is especially helpful in diagnosing malignancy typically in the presence of a solid component in the cyst. Newer markers to improve diagnostic accuracy are on the horizon, but clinical studies are awaited.
Keywords: Pancreatic cysts, IPMN, EUS, KRAS
Introduction
Pancreatic cystic lesions (PCL) are being detected with increasing frequency because of the widespread use of cross-sectional imaging. In a recent study, up to 13.5% of patients undergoing magnetic resonance imaging for reasons unrelated to the pancreas were found to have a pancreatic cyst [1].
PCL represent a wide variety of lesions including congenital, inflammatory and neoplastic cysts [2]. The World Health Organization includes intraductal papillary mucinous neoplasms (IPMN), mucinous cystic neoplasms (MCN), solid pseudopapillary neoplasms (SPN) and serous cystic tumors (SCT) in the neoplastic category. IPMN and MCN together are known as mucinous cysts and along with SPN have malignant potential [3-6]. SCT are benign lesions [7], and along with pseudocysts, retention cysts and lymphoepithelial cysts have no malignant potential making surgical resection and surveillance unnecessary [8]. Branch duct IPMN (BD-IPMN), while possessing malignant potential, have been suggested to be indolent compared to their main duct counterpart [6,9-12]. The variety of PCL and their varied potential for malignant degeneration makes their management tedious. Guidelines have been suggested to assist in the management of pancreatic cystic lesions, which include resection and surveillance recommendations [13]. These recommendations rely on an accurate diagnosis of cyst type as well as assessment of the presence or absence of malignancy, which in reality, can be very challenging.
While dramatically increasing the detection of pancreatic cysts, cross sectional imaging has been found to be inaccurate for the diagnosis of pancreatic cystic lesions with an accuracy of around 61% for differentiating between mucinous, nonmucinous, and malignant PCL [14]. Endoscopic ultrasound (EUS) allows for high resolution imaging of the pancreas, however EUS morphology alone has an accuracy of 50-73% for differentiation between mucinous and nonmucinous cysts and suffers from high interobserver variability even amongst experts [15-18].
The current diagnostic evaluation of PCL often includes EUS-guided fine needle aspiration (EUS-FNA) for cyst fluid analysis. Cyst fluid can be analyzed for tumor markers, cytology, mucins (MUCs), DNA analysis, viscosity and chemistries (most commonly amylase). Here, we present a review of the available literature in the utility of cyst fluid analysis in the differentiation of pancreatic cystic lesions.
Tumor markers
Early studies in the 1980s suggested the role of carcinoembryonic antigen (CEA) and carbohydrate antigen (CA) 19-9 in the differentiation of PCL [19,20]. In 1992, Lewandrowski et al in a series of 26 patients, noted that cyst fluid CEA levels were high (>367 ng/mL) in both benign and malignant mucinous cysts, but low (<23 ng/ mL) in pseudocysts and serous cystadenomas (SCA), an indication that CEA can discriminate between mucinous and nonmucinous cysts. In the same study, CA 19-9 and 125 levels were more variable with overlap between mucinous and nonmucinous cysts.
Additional studies followed demonstrating that tumor markers CEA and CA 72-4 were present in high concentrations in the cyst fluid from mucinous cystic neoplasms with various optimal levels and accuracies [21-24]. In 2004, a multicenter prospective study demonstrated that various combinations of morphology, cytology and tumor markers (CEA, CA 72-4, CA 125, CA 19-9 and CA 15-3) did not provide additional diagnostic accuracy [16]. Instead, cyst fluid concentration of CEA alone was found to be more accurate than combination testing. An optimal cutoff value of 192 mg/mL was associated with a diagnostic accuracy of 79% for detection of mucinous cysts.
In a pooled review of 12 studies including the multicenter study noted above, a CEA >800 ng/mL strongly suggested mucinous pathology with a specificity of 98% although sensitivity was poor at only 48% for an overall accuracy of 79% [25]. A CEA<5 had similar performance characteristics (sensitivity 50%, specificity 95%, accuracy 67%) for detection of a SCA or pseudocyst. Also noted was that a CA 19-9 <37 U/mL was strongly indicative of a pseudocyst or SCA with a specificity of 98%. Again, however, sensitivity was poor at only 19% yielding an accuracy of only 46%.
Several studies have been published since with variable ranges of CEA levels for optimal detection of mucinous cysts ranging from 30 ng/mL to 480 ng/mL [7,26-28]. In a more recent single center experience, cyst fluid CEA values for mucinous (benign and malignant) and nonmucinous (inflammatory and serous) cysts were compared in 154 subjects [17]. Forty patients did not have sufficient fluid for CEA analysis. A significant difference was seen between mucinous, serous, and inflammatory cyst types. The calculated optimal CEA cutoff value for distinguishing between a mucinous and nonmucinous cyst was 109.9 ng/mL, with a reported sensitivity and specificity of 81% and 98%, respectively, for an overall accuracy of 86%. No difference in CEA levels were seen between benign mucinous and malignant mucinous cysts.
Benign lymphoepithelial cysts have been found to express high levels of CEA. Although lined by squamous-type epithelium, a recent series found that all resected lymphoepithelial cysts expressed CEA as well as CA19-9 with some exhibiting markedly elevated cyst fluid CEA levels [29].
Currently, pancreatic cyst CEA level is considered the most accurate tumor marker for diagnosing a mucinous PCL. The accuracy may vary among different laboratories and approximately 0.2 to 1.0 mL of cyst fluid is required to run the test. A cut-off of 192 ng/mL is typically referenced as the standard although not insignificant differences can be seen between studies and levels can vary from laboratory to laboratory. At our institution, CEA is the only cyst fluid tumor marker that is routinely used at this time for the diagnostic work-up of a PCL.
Cytology
Cytology typically relies on the detection of: a) MUC-containing cells (in case of IPMN and MCN), b) malignant cells, c) glycogen-rich cuboidal cells (in case of SCT), d) branching papillae with myxoid stroma in the case of a solid pseudopapillary neoplasm (SPN), and e) abundant anucleate squamous cells and debris in lymphoepithelial cysts.
In the absence of an associated solid component, however, pancreatic cyst fluid from mucinous cysts is frequently acellular or paucicellular with resultant low diagnostic yield. In two large, multicenter studies, detection of MUC-containing cells led to a sensitivity of 32-35% and specificity of ~83% for diagnosing MCN and IPMN [16,26]. The reported overall accuracy in the first study was 59%, which was not much better than EUS morphology alone and significantly less than that of cyst fluid CEA level [16]. In a pooled review, overall combined sensitivities of 45% and 48% were seen for the detection of benign mucinous and malignant cysts, respectively [25]. For the detection of SCT, cytology was even poorer with a positive result in only 23/60 or 38% of cases [25].
In a recently published single center study of 141 cysts, cytology was diagnostic in 58% of subjects [17]. Although the cytology findings were highly specific (51/53, 96%), they were insensitive (61/141, 43%), resulting in a low overall accuracy for detection of mucinous lesions at 58%. However, when compared to EUS morphology and CEA for the detection of malignant cysts, cytology was the most accurate with a sensitivity of 38%, specificity of 96% and accuracy of 75%.
Recent studies have shown that the yield of cytology can be increased with the use of a cytobrush passed through a 19 gauge FNA needle [30,31]. When compared to standard EUS-FNA, in cysts larger than 2cm, cytobrushings were significantly more likely to detect MUC-containing cells. Significant complications were seen in 8% (3/39) of patients undergoing cytobrushings, which included bleeding in one and acute pancreatitis in the remainder. This technique has yet to become routine practice.
Mucins
MUCs are heavily glycosylated, high-molecular-weight glycoproteins that are commonly expressed in epithelial cells, which line mucinous cystic neoplasms. These can be detected by special MUC stains (mucicarmine, Alciana blue/PAS) or by the detection of a number of different specific glycoproteins utilizing gene expression.
MUC staining can be performed on specimens sent for cytology and has the benefit of not requiring any additional cyst fluid. A PPV of 83% for the detection of a mucinous cyst using MUC staining has been reported [32]. Sensitivity, however, was poor with only 12/29 mucinous cysts being detected by staining. A second, relatively small study, noted a sensitivity of mucicarmine staining for detecting MCN at 56% (5/9 lesions) [33]. In a more recent and larger series of patients, 66/121 mucinous cysts were positive for MUC with a reported sensitivity of 80% and specificity of 40% [34]. MUC staining was found to be complementary to cyst CEA levels and cytology and when 1 of 3 was found to be positive, sensitivity and specificity increased to 92% and 52%, respectively, for an overall PPV of 86%.
Staining of gastric contaminants, which may be misinterpreted as cyst fluid epithelial cells is a limitation of MUC staining. Furthermore, MUC staining does not provide any potential information regarding MUC expression. MUCs come in a variety of different categories and aberrant/altered MUC expression has been previously described in pancreatic ductal adenocarcinoma (DAC) and its role in mucinous neoplasms has been evaluated [35].
While MUC1 is not expressed in the normal pancreas, it is aberrantly expressed in DAC [36,37]. It has been noted that MUC1 is also expressed in the invasive components of mucinous cysts that are of DAC or undifferentiated carcinoma type whereas noninvasive MCN lack MUC1 expression and alternatively express MUC2 and MUC5A [36-38]. This information suggests that MUC1 may be a potential indicator of invasiveness while the presence of MUC2 and MUC5A is more suggestive of noninvasive disease. A number of studies have had conflicting results including a series of resected lymphoepithelial cysts all expressing MUC1 [29]. In a recent study, the expression of MUC1 was similar in both neoplastic and nonneoplastic cysts and was also expressed in half of all patients with chronic pancreatitis [39].
DNA
The progression of normal pancreatic duct cells to pancreatic cancer is characterized by the accumulation of genetic mutations, gene silencing, and chromosomal deletions [40]. As such, cyst fluid DNA analysis has been investigated with the aim to differentiate premalignant mucinous pancreatic cysts from nonmucinous cysts, and to detect malignancy in pancreatic cysts.
There has been one prospective, multicenter study of pancreatic cyst DNA analysis [26]. In this study, the presence of a KRAS mutation in cyst fluid was highly specific for a mucinous cyst (96%) but the sensitivity (45%) was low. The elements of DNA analysis associated with malignant cysts included a high DNA amount (optical density ratio >10) and allelic loss amplitude over 82% (suggesting that 82% of the DNA in the fluid was affected by the mutation) with a sensitivity of 70% and a specificity of 85%. The presence of a high amplitude KRAS mutation (i.e. most of the DNA in the fluid was affected by the mutation) followed by allelic loss showed maximum specificity (96%) for malignancy but poor sensitivity. These results were not able to be validated in one small cohort of patients in which consistency in histology, CEA levels, and molecular analysis was seen in approximately 1/3 of the cases [41]. However, an additional study of 35 cysts found that DNA analysis including the components discussed above had a sensitivity and specificity of 83% and 100% for a malignant cyst and 86% and 93% for a benign mucinous cyst [42].
A comparison between CEA and molecular analysis noted poor agreement for diagnosis of mucinous cysts [43]. Only a fraction (19/100) of the included patients, however, had a final histological diagnosis, making the drawing of any conclusions from this data difficult.
We recently completed a long term follow up study of patients who underwent EUS-FNA along with complete DNA analysis [44]. Pancreatic cysts were categorized as “non-indolent” and “indolent” based on surgical pathology and outcome. In a multivariate analysis, pancreatic cyst fluid KRAS mutation was the only component of cyst fluid analysis associated with non-indolent behavior including resection of a mucinous cyst, cyst progression, development of malignancy and death due to pancreatic cancer.
In our practice at the University of Pittsburgh, detection of KRAS mutation is the only molecular marker currently used for the diagnosis of IPMN and MCN. This test can be easily performed at most tertiary hospital laboratories and the amount of cyst fluid necessary for analysis is only a fraction of a milliliter (1-2 drops). This cost of the molecular analysis at our institution is bundled with the cytology interpretation charges. There is also a commercial lab that offers this testing (RedPath Integrated Pathology Inc.).
Viscosity
Mucinous cyst aspirates were reported to be viscous in the early 1990s. In 1993, Lewandrowski and others reported that measurement of the relative viscosity in cyst fluid demonstrated high (> serum viscosity) values in 89% of mucinous tumors and low values (< serum) in all pseudocysts and SCA [45]. In a more recent single center prospective study of 71 patients, mean viscosity was significantly higher in MCN compared to pseudocysts and SCT [28].
The concept of the “string sign” as an indirect and inexpensive measurement of viscosity was introduced in 2009 by Leung et al [27]. Determined by placing a sample of aspirated fluid between the thumb and index finger and measuring the length of stretch prior to disruption, they noted a median string sign of 0 mm in benign cysts and 3.5 mm in mucinous cysts. Furthermore, for every 1mm increase, the risk of a mucinous cyst increased by 116%.
In our experience, viscosity remains a subjective measure and is used along with objective evidence obtained via cyst fluid analysis to differentiate PCL.
Amylase
As an indicator of pancreatic duct communication, cyst fluid amylase levels are commonly used to aid in the differentiation of PCL. High levels are most commonly seen in pseudocysts although are often seen in both MCN and IPMN. In one study, a cutoff value for cyst amylase level of > 479 U/L showed a sensitivity of 73% and a specificity of 90% for distinguishing pseudocysts from cystic neoplasms [33]. A pooled review of 12 studies from 2005, all with histologic diagnosis, found that cysts with amylase <250 U/L were SCA, MCA, or MCAC (sensitivity 44%, specificity 98%) and this cutoff virtually excluded pseudocysts [25].
Used in conjunction with other markers, for cysts with CEA<30 ng/mL (i.e., presumed nonmucinous), a cyst fluid amylase level >8500 U/L detected 91% of pseudocysts, while an amylase <350 U/L captured 85% of SCA [7]. However, a more recent large single-center study, reported no difference in the mean cyst fluid amylase concentration when comparing mucinous and nonmucinous cysts [17].
We find cyst fluid amylase to be of limited utility in the evaluation of PCL in our practice.
Future markers
Recently, GNAS mutations have been implicated in the development of IPMN [46]. Mutations of the GNAS oncogene have previously been shown in other tumors but not in IPMN. Massively parallel sequencing of DNA from cyst fluid and tissue from 19 IPMN for mutations in 169 genes showed that 14 of 19 IPMN carried a KRAS mutation and 6 of 19 IPMN carried a GNAS mutation [47].
An evolving area of interest is the role microRNA (miRNA) may play in the development and progression in IPMN and MCN. MicroRNA are small non-coding RNA (17-25 nucleotides) that regulate gene expression at the post-transcriptional level. Altered expression of most miRNA has been shown in pancreatic cancer. A recent study showed that 10/12 miRNA dysregulated in pancreatic cancer were over-expressed in surgically obtained tissue from 15 non-invasive IPMN (miR-155 and miR-21 had the highest relative fold-change) [48].
Using cytokines as a measurement of antitumor response, a recent evaluation in patients with IPMN found that interleukins IL1 and IL8 concentrations were noted to be significantly higher in those with high grade dysplasia or malignancy compared to those with low or moderate dysplasia [49]. On multivariate analysis, IL1β remained a significant biomarker of high-risk cysts suggesting its usefulness as a potential biomarker.
Clinical application of these exciting new potential biomarkers awaits further study.
Concluding remarks
Pancreatic cyst fluid analysis is an important component of the work up of pancreatic cysts. Properly utilized, it can provide important information that can be used to improve the diagnosis of PCL (Table 1). We currently use cyst fluid cytology, CEA level and KRAS mutation analysis in our clinical practice. Cytology assessment is useful primarily to make a
Table 1.
Typical pancreatic cyst fluid analysis findings
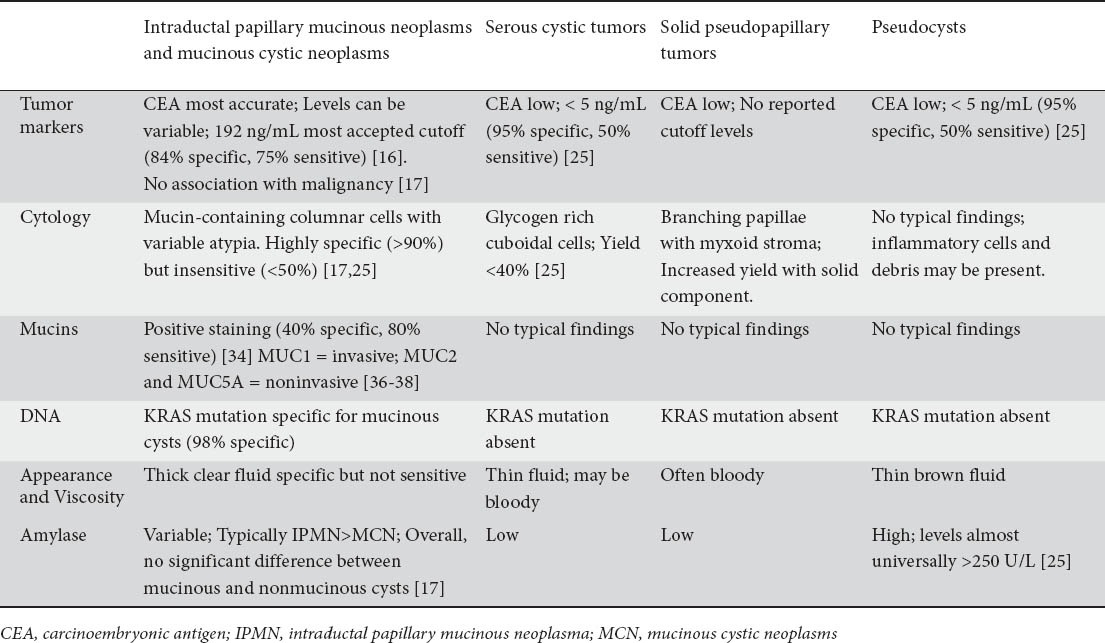
Intraductal papillary mucinous neoplasms Serous cystic tumors Solid pseudopapillary Pseudocysts and mucinous cystic neoplasms tumors diagnosis of malignant cysts especially in the presence of a solid component. If a cyst fluid KRAS mutation is present, we assume the cyst to be mucinous. In the absence of KRAS mutation (due to poor sensitivity ~50%), cyst fluid CEA is the most accurate marker of a mucinous cyst.
Biography
University of Pittsburgh, USA
Footnotes
Conflict of Interest: None
References
- 1.Lee KS, Sekhar A, Rofsky NM, et al. Prevalence of incidental pancreatic cysts in the adult population on MR imaging. Am J Gastroenterol. 2010;105:2079–2084. doi: 10.1038/ajg.2010.122. [DOI] [PubMed] [Google Scholar]
- 2.Brugge WR, Lauwers GY, Sahani D, et al. Cystic neoplasms of the pancreas. N Engl J Med. 2004;351:1218–1226. doi: 10.1056/NEJMra031623. [DOI] [PubMed] [Google Scholar]
- 3.Kobari M, Egawa S, Shibuya K, et al. Intraductal papillary mucinous tumors of the pancreas comprise 2 clinical subtypes: differences in clinical characteristics and surgical management. Arch Surg. 1999;134:1131–1136. doi: 10.1001/archsurg.134.10.1131. [DOI] [PubMed] [Google Scholar]
- 4.Salvia R, Fernandez-del Castillo C, Bassi C, et al. Main-duct intraductal papillary mucinous neoplasms of the pancreas: clinical predictors of malignancy and long-term survival following resection. Ann Surg. 2004;239:678–85. doi: 10.1097/01.sla.0000124386.54496.15. discussion 685-687. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Sohn TA, Yeo CJ, Cameron JL, et al. Intraductal papillary mucinous neoplasms of the pancreas: an updated experience. Ann Surg. 2004;239:788–97. doi: 10.1097/01.sla.0000128306.90650.aa. discussion 797-799. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Sugiyama M, Izumisato Y, Abe N, et al. Predictive factors for malignancy in intraductal papillary-mucinous tumours of the pancreas. Br J Surg. 2003;90:1244–1249. doi: 10.1002/bjs.4265. [DOI] [PubMed] [Google Scholar]
- 7.Snozek CL, Mascarenhas RC, O’Kane DJ. Use of cyst fluid CEA, CA19-9, and amylase for evaluation of pancreatic lesions. Clin Biochem. 2009;42:1585–1588. doi: 10.1016/j.clinbiochem.2009.06.020. [DOI] [PubMed] [Google Scholar]
- 8.Khalid A, Brugge W. ACG practice guidelines for the diagnosis and management of neoplastic pancreatic cysts. Am J Gastroenterol. 2007;102:2339–2349. doi: 10.1111/j.1572-0241.2007.01516.x. [DOI] [PubMed] [Google Scholar]
- 9.Fernandez-del Castillo C, Targarona J, Thayer SP, et al. Incidental pancreatic cysts: clinicopathologic characteristics and comparison with symptomatic patients. Arch Surg. 2003;138:427–433. doi: 10.1001/archsurg.138.4.427. discussion 433-434. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Irie H, Yoshimitsu K, Aibe H, et al. Natural history of pancreatic intraductal papillary mucinous tumor of branch duct type: follow-up study by magnetic resonance cholangiopancreatography. J Comput Assist Tomogr. 2004;28:117–122. doi: 10.1097/00004728-200401000-00020. [DOI] [PubMed] [Google Scholar]
- 11.Pelaez-Luna M, Chari ST, Smyrk TC, et al. Do consensus indications for resection in branch duct intraductal papillary mucinous neoplasm predict malignancy? A study of 147 patients. Am J Gastroenterol. 2007;102:1759–1764. doi: 10.1111/j.1572-0241.2007.01224.x. [DOI] [PubMed] [Google Scholar]
- 12.Sohn TA, Yeo CJ, Cameron JL, et al. Intraductal papillary mucinous neoplasms of the pancreas: an increasingly recognized clinicopathologic entity. Ann Surg. 2001;234:313–321. doi: 10.1097/00000658-200109000-00005. discussion 321-322. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Tanaka M, Chari S, Adsay V, et al. International consensus guidelines for management of intraductal papillary mucinous neoplasms and mucinous cystic neoplasms of the pancreas. Pancreatology. 2006;6:17–32. doi: 10.1159/000090023. [DOI] [PubMed] [Google Scholar]
- 14.Fisher WE, Hodges SE, Yagnik V, et al. Accuracy of CT in predicting malignant potential of cystic pancreatic neoplasms. HPB (Oxford) 2008;10:483–490. doi: 10.1080/13651820802291225. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Ahmad NA, Kochman ML, Lewis JD, et al. Can EUS alone differentiate between malignant and benign cystic lesions of the pancreas? Am J Gastroenterol. 2001;96:3295–3300. doi: 10.1111/j.1572-0241.2001.05328.x. [DOI] [PubMed] [Google Scholar]
- 16.Brugge WR, Lewandrowski K, Lee-Lewandrowski E, et al. Diagnosis of pancreatic cystic neoplasms: a report of the cooperative pancreatic cyst study. Gastroenterology. 2004;126:1330–1336. doi: 10.1053/j.gastro.2004.02.013. [DOI] [PubMed] [Google Scholar]
- 17.Cizginer S, Turner B, Bilge AR, et al. Cyst fluid carcinoembryonic antigen is an accurate diagnostic marker of pancreatic mucinous cysts. Pancreas. 2011;40:1024–1028. doi: 10.1097/MPA.0b013e31821bd62f. [DOI] [PubMed] [Google Scholar]
- 18.Frossard JL, Amouyal P, Amouyal G, et al. Performance of endosonography-guided fine needle aspiration and biopsy in the diagnosis of pancreatic cystic lesions. Am J Gastroenterol. 2003;98:1516–1524. doi: 10.1111/j.1572-0241.2003.07530.x. [DOI] [PubMed] [Google Scholar]
- 19.Nishida K, Shiga K, Kato K, et al. Two cases of pancreatic cystadenocarcinoma with elevated CA 19-9 levels in the cystic fluid in comparison with two cases of pancreatic cystadenoma. Hepatogastroenterology. 1989;36:442–445. [PubMed] [Google Scholar]
- 20.Tatsuta M, Iishi H, Ichii M, et al. Values of carcinoembryonic antigen, elastase 1, and carbohydrate antigen determinant in aspirated pancreatic cystic fluid in the diagnosis of cysts of the pancreas. Cancer. 1986;57:1836–1839. doi: 10.1002/1097-0142(19860501)57:9<1836::aid-cncr2820570922>3.0.co;2-d. [DOI] [PubMed] [Google Scholar]
- 21.Hammel P, Levy P, Voitot H, et al. Preoperative cyst fluid analysis is useful for the differential diagnosis of cystic lesions of the pancreas. Gastroenterology. 1995;108:1230–1235. doi: 10.1016/0016-5085(95)90224-4. [DOI] [PubMed] [Google Scholar]
- 22.Hammel P, Voitot H, Vilgrain V, et al. Diagnostic value of CA 72-4 and carcinoembryonic antigen determination in the fluid of pancreatic cystic lesions. Eur J Gastroenterol Hepatol. 1998;10:345–348. doi: 10.1097/00042737-199804000-00012. [DOI] [PubMed] [Google Scholar]
- 23.Sand JA, Hyoty MK, Mattila J, et al. Clinical assessment compared with cyst fluid analysis in the differential diagnosis of cystic lesions in the pancreas. Surgery. 1996;119:275–280. doi: 10.1016/s0039-6060(96)80113-9. [DOI] [PubMed] [Google Scholar]
- 24.Sperti C, Pasquali C, Guolo P, et al. Serum tumor markers and cyst fluid analysis are useful for the diagnosis of pancreatic cystic tumors. Cancer. 1996;78:237–243. doi: 10.1002/(SICI)1097-0142(19960715)78:2<237::AID-CNCR8>3.0.CO;2-I. [DOI] [PubMed] [Google Scholar]
- 25.van der Waaij LA, van Dullemen HM, Porte RJ. Cyst fluid analysis in the differential diagnosis of pancreatic cystic lesions: a pooled analysis. Gastrointest Endosc. 2005;62:383–389. doi: 10.1016/s0016-5107(05)01581-6. [DOI] [PubMed] [Google Scholar]
- 26.Khalid A, Zahid M, Finkelstein SD, et al. Pancreatic cyst fluid DNA analysis in evaluating pancreatic cysts: a report of the PANDA study. Gastrointest Endosc. 2009;69:1095–1102. doi: 10.1016/j.gie.2008.07.033. [DOI] [PubMed] [Google Scholar]
- 27.Leung KK, Ross WA, Evans D, et al. Pancreatic cystic neoplasm: the role of cyst morphology, cyst fluid analysis, and expectant management. Ann Surg Oncol. 2009;16:2818–2824. doi: 10.1245/s10434-009-0502-9. [DOI] [PubMed] [Google Scholar]
- 28.Linder JD, Geenen JE, Catalano MF. Cyst fluid analysis obtained by EUS-guided FNA in the evaluation of discrete cystic neoplasms of the pancreas: a prospective single-center experience. Gastrointest Endosc. 2006;64:697–702. doi: 10.1016/j.gie.2006.01.070. [DOI] [PubMed] [Google Scholar]
- 29.Raval JS, Zeh HJ, Moser AJ, et al. Pancreatic lymphoepithelial cysts express CEA and can contain mucous cells: potential pitfalls in the preoperative diagnosis. Mod Pathol. 2010;23:1467–1476. doi: 10.1038/modpathol.2010.144. [DOI] [PubMed] [Google Scholar]
- 30.Al-Haddad M, Gill KR, Raimondo M, et al. Safety and efficacy of cytology brushings versus standard fine-needle aspiration in evaluating cystic pancreatic lesions: a controlled study. Endoscopy. 2010;42:127–132. doi: 10.1055/s-0029-1215351. [DOI] [PubMed] [Google Scholar]
- 31.Al-Haddad M, Raimondo M, Woodward T, et al. Safety and efficacy of cytology brushings versus standard FNA in evaluating cystic lesions of the pancreas: a pilot study. Gastrointest Endosc. 2007;65:894–898. doi: 10.1016/j.gie.2006.08.047. [DOI] [PubMed] [Google Scholar]
- 32.Walsh RM, Henderson JM, Vogt DP, et al. Prospective preoperative determination of mucinous pancreatic cystic neoplasms. Surgery. 2002;132:628–633. doi: 10.1067/msy.2002.127543. discussion 633-634. [DOI] [PubMed] [Google Scholar]
- 33.Ryu JK, Woo SM, Hwang JH, et al. Cyst fluid analysis for the differential diagnosis of pancreatic cysts. Diagn Cytopathol. 2004;31:100–105. doi: 10.1002/dc.20085. [DOI] [PubMed] [Google Scholar]
- 34.Morris-Stiff G, Lentz G, Chalikonda S, et al. Pancreatic cyst aspiration analysis for cystic neoplasms: mucin or carcinoembryonic antigen--which is better? Surgery. 2010;148:638–644. doi: 10.1016/j.surg.2010.07.023. discussion 644-645. [DOI] [PubMed] [Google Scholar]
- 35.Haab BB, Porter A, Yue T, et al. Glycosylation variants of mucins and CEACAMs as candidate biomarkers for the diagnosis of pancreatic cystic neoplasms. Ann Surg. 2010;251:937–945. doi: 10.1097/SLA.0b013e3181d7738d. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Masaki Y, Oka M, Ogura Y, et al. Sialylated MUC1 mucin expression in normal pancreas, benign pancreatic lesions, and pancreatic ductal adenocarcinoma. Hepatogastroenterology. 1999;46:2240–2245. [PubMed] [Google Scholar]
- 37.Yonezawa S, Taira M, Osako M, et al. MUC-1 mucin expression in invasive areas of intraductal papillary mucinous tumors of the pancreas. Pathol Int. 1998;48:319–322. doi: 10.1111/j.1440-1827.1998.tb03913.x. [DOI] [PubMed] [Google Scholar]
- 38.Luttges J, Feyerabend B, Buchelt T, et al. The mucin profile of noninvasive and invasive mucinous cystic neoplasms of the pancreas. Am J Surg Pathol. 2002;26:466–471. doi: 10.1097/00000478-200204000-00008. [DOI] [PubMed] [Google Scholar]
- 39.Carrara S, Cangi MG, Arcidiacono PG, et al. Mucin expression pattern in pancreatic diseases: findings from EUS-guided fine-needle aspiration biopsies. Am J Gastroenterol. 2011;106:1359–1363. doi: 10.1038/ajg.2011.22. [DOI] [PubMed] [Google Scholar]
- 40.Khalid A, McGrath KM, Zahid M, et al. The role of pancreatic cyst fluid molecular analysis in predicting cyst pathology. Clin Gastroenterol Hepatol. 2005;3:967–973. doi: 10.1016/s1542-3565(05)00409-x. [DOI] [PubMed] [Google Scholar]
- 41.Sreenarasimhaiah J, Lara LF, Jazrawi SF, et al. A comparative analysis of pancreas cyst fluid CEA and histology with DNA mutational analysis in the detection of mucin producing or malignant cysts. JOP. 2009;10:163–168. [PubMed] [Google Scholar]
- 42.Shen J, Brugge WR, Dimaio CJ, et al. Molecular analysis of pancreatic cyst fluid: a comparative analysis with current practice of diagnosis. Cancer. 2009;117:217–227. doi: 10.1002/cncy.20027. [DOI] [PubMed] [Google Scholar]
- 43.Sawhney MS, Devarajan S, O’Farrel P, et al. Comparison of carcinoembryonic antigen and molecular analysis in pancreatic cyst fluid. Gastrointest Endosc. 2009;69:1106–1110. doi: 10.1016/j.gie.2008.08.015. [DOI] [PubMed] [Google Scholar]
- 44.Rockacy MJ, Zahid M, McGrath KM, Khalid A. Long term follow-up and outcome of patients with pancreatic cysts following cyst EUS-FNA and DNA analysis. Gastrointest Endosc. 2011;73:AB153. [Google Scholar]
- 45.Lewandrowski KB, Southern JF, Pins MR, et al. Cyst fluid analysis in the differential diagnosis of pancreatic cysts. A comparison of pseudocysts, serous cystadenomas, mucinous cystic neoplasms, and mucinous cystadenocarcinoma. Ann Surg. 1993;217:41–47. doi: 10.1097/00000658-199301000-00008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Furukawa T, Kuboki Y, Tanji E, et al. Whole-exome sequencing uncovers frequent GNAS mutations in intraductal papillary mucinous neoplasms of the pancreas. Sci Rep. 2011;1:161. doi: 10.1038/srep00161. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Wu J, Matthaei H, Maitra A, et al. Recurrent GNAS mutations define an unexpected pathway for pancreatic cyst development. Sci Transl Med. 2011;3:92ra66. doi: 10.1126/scitranslmed.3002543. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Habbe N, Koorstra JB, Mendell JT, et al. MicroRNA miR-155 is a biomarker of early pancreatic neoplasia. Cancer Biol Ther. 2009;8:340–346. doi: 10.4161/cbt.8.4.7338. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Maker AV, Katabi N, Qin LX, et al. Cyst fluid interleukin-1beta (IL1beta) levels predict the risk of carcinoma in intraductal papillary mucinous neoplasms of the pancreas. Clin Cancer Res. 2011;17:1502–1508. doi: 10.1158/1078-0432.CCR-10-1561. [DOI] [PMC free article] [PubMed] [Google Scholar]