

Abstract
An important role of the paediatrician is that of a teacher – every clinician is an educator to patients and their families. This education, however, often occurs under difficult or time-pressured learning conditions. The authors present principles derived from three basic theories of human cognition that may help to guide clinicians’ instruction of parents and patients. Cognitive load theory holds that an individual’s capacity to process information is finite. By controlling information flow rate, decreasing reliance on working memory and removing extraneous cognitive load, learning is improved. Dual code theory suggests that humans have separate cognitive ‘channels’ for text/audio information versus visual information. By constructing educational messages that take advantage of both channels simultaneously, information uptake may be improved. Multimedia theory is based on the notion that there is an optimal blend of media to accomplish a given learning objective. The authors suggest seven practical strategies that clinicians may use to improve patient education.
Keywords: Cognition, Health Education, Multimedia, Teaching materials
Abstract
Le pédiatre occupe un rôle important à titre d’enseignant. En effet, chaque clinicien est un enseignant auprès des patients et de leur famille. Les médecins transmettent souvent cet enseignement dans des conditions d’apprentissage difficiles ou lorsqu’ils sont pressés par le temps. Les auteurs présentent des principes dérivés de trois théories fondamentales de la cognition humaine, qui peuvent contribuer à orienter les directives des cliniciens aux parents et aux patients. Selon la théorie de la charge cognitive, la capacité de traiter l’information est limitée. En contrôlant le débit d’information, en se fiant moins à la mémoire à court terme et en se débarrassant de la charge cognitive parasite, l’apprentissage s’améliore. D’après la théorie du double codage, les humains ont des canaux cognitifs distincts pour assimiler l’information écrite ou auditive et l’information visuelle. En énonçant des messages d’enseignement qui puisent simultanément dans ces deux canaux, on peut améliorer la rétention de l’information. La théorie de l’apprentissage multimédia repose sur la notion qu’il existe une association optimale de médias pour parvenir à un objectif d’apprentissage donné. Les auteurs proposent sept stratégies pratiques que peuvent utiliser les cliniciens pour améliorer l’enseignement aux patients.
CASE PRESENTATION
Case 1
A five-year-old boy presents to the emergency department with a purpuric rash over both lower limbs, which had developed over the preceding 48 h. You diagnose Henoch-Schonlein purpura (HSP), describing the immune-mediated vasculitis that causes it. You warn the parents to watch for testicular swelling and abdominal pain, and to follow-up in a week. They express their understanding and are discharged. The next day, the family doctor calls the emergency department. The family is in her office, confused and distraught.
Case 2
A four-year-old girl presents with dyspnea including tachypnea, moderate retractions and wheezing. She is treated with prednisolone and β-agonist inhalations and, 4 h later, she is ready for discharge home. You explain that this may be asthma and verbally describe the indications for return including increased respiratory rate and retractions between the ribs or subcostally. The parents express their understanding and the girl is discharged. The next day, the child steadily worsens; however, the parents delay returning until she is in extremis.
INTRODUCTION
Effective communication with patients and their caregivers is central to the role of the paediatrician (1,2). In particular, good patient education results in improved outcomes through better compliance, health care utilization and satisfaction (1,3). In the present evidence-based review, we use the cases described above to illustrate how some basic cognitive principles of learning can help all clinicians better inform their patients, particularly in time-pressured settings.
In both of the cases presented above, there was a failure in the physician-patient interaction that led to a misunderstanding. While the importance of good clinical communication skills is appropriately stressed in undergraduate and residency curricula (2), we will concentrate on the educational aspect of the clinician’s interaction with a patient. Cognitive load theory describes the finite limits to human cognition and how we should take them into account as we attempt to deliver information (4). An important step forward has been our understanding of how the brain processes visual and language information in apparently separate systems (dual code theory) (5). Multimedia theory holds that by using juxtapositions of graphics and audio appropriate to the content, we can more efficiently transfer larger amounts of information in a given period of time (6). In each of the following sections, we describe the implications of the theories for clinical practice in the form of seven useful strategies (Table 1).
TABLE 1.
Recommendations for improved patient education
| Recommendation | The clinician could, for example… | Rationale |
|---|---|---|
| 1. When possible, bypass the limits of working memory | …rely less on patient memory for spoken instructions and more on enduring materials such as printed, tailored instructions | Short-term or ‘working’ memory is a bottleneck for information uptake and is easily overwhelmed |
| 2. Let the patient control the information flow rate | …check frequently with the patient for understanding; leave the patient to consider materials at their own pace | The working memory bottleneck is less restrictive when the time available for information uptake is longer |
| 3. Decrease extraneous cognitive load | …eliminate the decorations or excessive details on patient education materials | The brain, under situations of potential overload, must use resources to process both the relevant and the nonrelevant |
| 4. Present information using words AND graphics for maximal uptake | …in addition to spoken words, use pictures of relevant structures or schematics to convey clinical information | Graphics and other visual information bypass the bottleneck for uptake of spoken information resulting in better information transfer per unit time |
| 5. Present the words and graphics at the same time | …attempt to use graphics, visualizations or even gestures that can be synchronized with the spoken message | The ability to make simultaneous connections between the visual and the auditory information in a message improve its uptake |
| 6. Use visual methods to present visual concepts | …use video or animations for dynamic processes instead of spoken words to describe visual phenomena such as dyspnea or rashes | Even if memory constraints are not an issue, matching the content to the format of the educational message results in better learning |
| 7. For maximal effectiveness, it matters how graphics are combined with text | …ensure that all parts of the message are coherent, specifically avoiding redundant or extraneous material (less is more) | Optimal educational uptake occurs when the haptic, aural and visual channels are used in a manner that takes into account the nature of the information to be conveyed |
COGNITIVE LOAD THEORY: TAKE INTO ACCOUNT COGNITIVE LIMITS
Cognitive load theory holds that an individual’s capacity to process information is finite. By taking this into consideration, we can optimize the uptake of new information by patients and their families. The short-term ability of the average human to process (learn) information is finite and limited. This limited initial processor of information is often referred to as an individual’s ‘working memory’ (7). Complexity of information and the rate of presentation will consume working memory to varying degrees, thereby impacting learning. Long-term memory, in contrast, is considerably less restrained; there are multiple examples of remarkable feats of memory that are possible with training, practice and expertise (8). Working memory has famously been described as able to hold on to roughly seven discrete items at one time (9). Finite working memory is believed to be an evolutionary adaptation preventing us from becoming overwhelmed (10).
In a situation in which working memory is being used to its limits, the ‘cognitive load’ of the material to be learned becomes important. Factors that increase mental burden may be either intrinsic to the material (complexity) or extraneous and, thus, distracting from the content focus (nonrelevant material) (4). Furthermore, the degree to which the material is germane or relevant to an individual will also impact learning because there needs to be an active desire to learn the content (11,12). Thus, for educating patients and their families, it is important to keep in mind the finite limits of working memory and the cognitive load of the material (13,14).
1. When possible, bypass the limits of working memory
Working memory can be a ‘bottleneck’ when cognitive load is high. The seven-item limit is an often-used example of the finite bounds of working memory (9). Compare the difficulty of holding a new seven-digit phone number in memory, for even a few minutes, with the success rate of simply writing it down. For patients, we occasionally try to verbally convey complicated new information to patients when they would be much better served with a written handout. The implication for clinicians is that they should, whenever possible, avoid relying on the patient’s memory in favour of written materials (13).
2. Let the patient control the information flow rate
The impact of cognitive load can be alleviated by adjusting the rate of information flow to working memory. Ideally, instructions are given at a rate appropriate to the patient, adjusting based on non-verbal cues and frequent probing for understanding (15,16). In one illustrative example, Mayer and Chandler compared learning by college students regarding how lightning forms. In one study condition, the narrated animated (text and visual) explanation ran continuously for 2.5 min while in the other, the exact same content was broken up into 16 segments with the user controlling the pace using a ‘continue’ button. The latter condition was found to be clearly superior. The implication for clinicians is that, whenever possible, the patient should control the flow rate of new information.
3. Decrease extraneous cognitive load
Decreasing extraneous cognitive load enables the learner to use their limited resources to focus on the intrinsic load of the concepts to be learned. To illustrate this, consider an experiment involving learning of cardiovascular physiology by medical students. Butcher (17) randomly assigned 74 subjects to three study conditions: a text-only explanation; text plus a simple drawing; and text plus an anatomical drawing. While both groups with drawing-enhanced explanations performed better than the text-only group, there was an additional, clear advantage for the simple drawing. Their conclusion was that the additional detail on the complete drawing was not germane to the concepts to be learned and, thus, only acted as a barrier, using precious working memory. Stripping educational messages of nonessential elements facilitates learning.
Implications for example cases
In the HSP case, several ideas flow from an understanding of cognitive load theory. The physician could have improved comprehension by giving the parents a printed handout, especially one that included simple schematic representations of vasculitis. Handouts can be read while waiting for test results; this practical strategy enables an individual to control the rate of information flow (16).
DUAL CODE THEORY: USE MULTIPLE SENSES TO IMPROVE INFORMATION TRANSFER
Dual code theory suggests that humans have a separate cognitive ‘channel’ for text/audio information that is distinct from the channel for visual information (5). While the previously described cognitive load theory holds that working memory is a processing bottleneck for learning, dual code theory states that if we take into account how that bottleneck is organized, we can increase the uptake of new information (6,18).
Consider the case of a learner who is watching a narrated PowerPoint (Microsoft Corporation, USA) presentation (Figure 1). As they view the slides, visual information enters their eyes and passes through the optic channels to a symbolic ‘visual sketchpad’ where a pixel-by-pixel pictorial model is formed within working memory (19). At the same time, the presenter’s spoken words enter the ears and, through the working memory auditory system, are processed on a ‘phonological loop’, a type of cognitive audio tape, that continuously spools as words enter (19,20). The important thing about these two separate working memory systems is that their capacities for processing information are independent of one another (11). Thus, these systems can be conceived of as two separate highways going in the same direction. In situations involving cognitive overload, it helps to use both pathways maximally (11).
Figure 1).
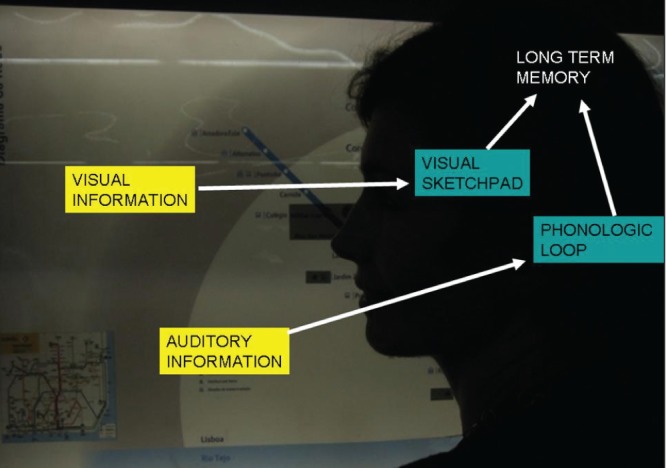
Dual code theory. Representation of dual code theory showing distinct areas of working memory for auditory (text) information and visual information. Using both routes to present information results in increased uptake in situations of potential cognitive overload
Once both the visual and auditory information register in the visual sketchpad and phonological loop of the working memory, respectively, it is integrated to create accessible knowledge in long-term memory (7). This process is aided by congruence between the visual and auditory material (21). Thus, PowerPoint slides that have text describing one topic while the narration involves a different topic results in suboptimal learning.
4. Present information using words AND graphics for maximal uptake
A large number of empirical studies document the superiority of combining words with graphics for presenting information over using either method alone (12,21,22). In one example of many, Brewer et al (23) demonstrated the power of graphics in a controlled trial comparing auditory jury instructions with auditory and visual instructions. The control group included 90 untrained adults while the comparison ‘expert’ group included 90 senior law students. The amount of learning was assessed using recall and recognition tests, and a transfer test using a novel scenario. When the jury instructions were given via the auditory route alone, the law students were clearly superior to the untrained adults; however, the difference was not observed when the same instructions were given with added animations and flow charts. This situation of giving instructions to untrained adults is analogous to the situation of discharge patient instructions. The implication is that explanatory graphics, such as sketches, images and video, can greatly augment words (22,24).
5. Present the words and graphics simultaneously
In an experiment that supports the dual code theory, Mayer and Anderson (18) presented college students information regarding how a piston works using standardized spoken words and graphics (6). They randomly assigned the students to receive the words either before the graphics or concurrently with the graphics. Although the group who received the words concurrent with graphics were allowed 50% less time with the material, they generated 50% more solutions to test problems than did the group who received the words before graphics. Their conclusion was that presenting the information concurrently not only takes advantage of the dual pathway but also allows representational connections to be made between the two forms. This, in turn, improves the uptake of the information into long-term memory and, thus, leads to the improved performance in this group.
Implications for example cases
The implication of dual code theory for clinicians is that it is helpful to have graphics prepared at the time of verbal instruction to enable parents and patients to develop accurate mental models. Even gestures have been shown to aid comprehension (25). For case 1, pictures or animations of intussusception can ‘flesh out’ verbal explanations. In case 2, anatomical representations of bronchioles may show how inhaled corticosteroids work differently from bronchodilators, thus improving the parents’ judgment regarding which to use when.
MULTIMEDIA THEORY: FIND JUST THE RIGHT BLEND OF MEDIA
While cognitive load theory and dual code theory describe the constraints on human processing, multimedia theory holds that there is an optimal blend of media (text, visual, aural and tactile) to accomplish a given learning objective.
Multimedia theory states that even when cognitive limits are not an issue (ie, when given unlimited time), people still learn more thoroughly from the thoughtful use of multiple combined media than from a single medium (6). The theory implies use of the appropriate media for a given concept. For example, using words or the aural channel to teach a visual concept is, at best, inefficient and, at worst, ineffective (26).
6. Use visual methods to present visual concepts
The appearance of rashes, the colour of bile, the process of intussusception, the signs of toxicity – are all concepts difficult to grasp without a visual aid. However, too often, suboptimally engineered systems leave a time-pressured clinician attempting to convey these visual concepts using only spoken words, thus ignoring the multimedia principle (6,21). Consider the asthma example: signs such as “retraction, sucking in between the ribs, distress, prolonged expiration” are extremely difficult to convey using spoken words, especially when compared with the ease with which they can be demonstrated on an appropriate video. Having a precompiled collection of visual materials to aid in explanations will be rewarded with increased patient understanding (26).
7. For maximal effectiveness, it matters how graphics are combined with text
Certain methods of combining text with graphics are better than others. While the term ‘multimedia’ can be used to indiscriminately label any computer presentation of material using two or more types of media, the multimedia theory describes particularly effective ways in which graphics can be combined with text (6). Numerous studies have shown that decorative clipart that does not integrate with the text is deleterious to learning (22). Only judicious use of animation is helpful (22,18). Redundant material harms rather than enhances educational effectiveness (21,22,27) Designs that ‘split attention’, such as having video in one pane and text in another, often impair learning (6).
Implications for example cases
The implication of multimedia theory is that, when designing patient educational materials, words and graphics should integrate to efficiently deliver the message. Verbal descriptions of ‘vasculitis’ for the HSP case or ‘bronchospasm’ can be misinterpreted by patients in any number of ways, whereas presenting the new terms in conjunction with well-honed visual representations results in more precise, reproducible understanding.
DISCUSSION
We have described the main principles of cognitive overload, dual code theory and multimedia theory. As we have documented, these fundamental attributes of human cognition are well established in the cognition literature. Careful instructional design of the discharge patient educational encounter, taking these principles into account, may be more effective than the informal approaches that dominate at present (13,16).
In the clinical literature, there are multiple articles documenting specific clinical conditions for which patient education is an effective therapeutic intervention (eg, asthma) or for which a unique window of opportunity exists (eg, alcohol abuse counselling after a motor vehicle collision) (1,3,16,28). This type of diagnosis-specific approach to patient education may be limited by case specificity. We have illustrated a more general approach that can be applied across cases.
Wei and Camargo (3) proposed eight criteria for evaluating an emergency department-based patient education program. These include ensuring that patient-education efforts take into account the ‘logistical constraints’ of the setting and are tailored to patients as well as their caregivers. Their highly sensible criteria, however, do not directly provide the practitioner with a conceptual framework for how a clinician can overcome the limitations in the moment. The cognitive theories presented here may be the basis for an adaptive, individualized approach to the problems posed by high cognitive load on the patient discharge educational interaction.
Fortunately, the increasing availability of Internet resources in the clinical environment makes it simpler than ever to use graphic media according to the principles we have outlined. Consider again the patient with HSP. We have found it very helpful to perform a Google (Google, USA) image search with the parent or patient watching, using the eponym as a search term. Looking at visual explanations of mechanisms, such as that for vasculitis, may help to enhance understanding and improve decision making by parents. Patients may find it reassuring to view pictures of others with a similar rash. Showing the appearance of more severe forms can also help in anticipatory guidance.
This can be accomplished in a brief session at the computer. A further benefit is the modelling, by the clinician, of effective heath information-seeking behaviour.
In the present selective review, we have not addressed some substantive patient education issues, such as culture, literacy, language and health access, all of which could contribute to or moderate the factors we have discussed.
CONCLUSIONS
Cognitive load theory holds that humans’ capacity to process information is finite. Dual code theory suggests that humans have a separate cognitive ‘channel’ for text/audio information that is distinct from the channel for visual information. Multimedia theory holds that there is an optimal blend of media to accomplish a given learning objective. These three theories have key implications for how patient education can be optimally structured.
Acknowledgments
The authors thank the members of the NYU Program for Medical Innovations and Research who reviewed early versions of this manuscript.
REFERENCES
- 1.Yin HS, Forbis SG, Dreyer BP. Health literacy and pediatric health. Curr Probl Pediatr Adoles Health Care. 2007;37:258–86. doi: 10.1016/j.cppeds.2007.04.002. [DOI] [PubMed] [Google Scholar]
- 2.Teutsch C. Patient-doctor communication. Med Clin North Am. 2003;87:1115–45. doi: 10.1016/s0025-7125(03)00066-x. [DOI] [PubMed] [Google Scholar]
- 3.Wei H, Camargo C. Patient Education in the Emergency Department. Acad Emerg Med. 2000;7:710–17. doi: 10.1111/j.1553-2712.2000.tb02052.x. [DOI] [PubMed] [Google Scholar]
- 4.Chandler P, Sweller J. Cognitive Load Theory and the Format of Instruction. Cogn Instr. 1991;8:293–332. [Google Scholar]
- 5.Paivio A. Dual coding theory: Retrospect and current status. Can J Psychol. 1991;45:255–87. [Google Scholar]
- 6.Mayer RE. Multimedia Learning. Cambridge, England: Cambridge University Press; 2009. p. 318. [Google Scholar]
- 7.Baddeley G, Hitch AD. Working Memory. Psychol Learning Motivation. 1974;8:47–89. [Google Scholar]
- 8.Ericsson KA, Lehmann AC. Expert and exceptional performance: evidence of maximal adaptation to task constraints. Ann Rev Psychol. 1996;47:273–305. doi: 10.1146/annurev.psych.47.1.273. [DOI] [PubMed] [Google Scholar]
- 9.Miller GA. The magical number seven, plus or minus two. Psychol Rev. 1956;63:81–97. [PubMed] [Google Scholar]
- 10.Sweller J. Evolution of human cognitive architecture. Psychol Learning Motivation. 2003;43:215–66. [Google Scholar]
- 11.Merriënboer JJG, Sweller J. Cognitive load theory and complex learning: Recent developments and future directions. Educ Psychol Rev. 2005;17:147–77. [Google Scholar]
- 12.Kalyuga S, Sweller J. Measuring knowledge to optimize cognitive load factors during instruction. J Educ Psychol. 2004;96:558–68. [Google Scholar]
- 13.Wilson EAH, Wolf MS. Working memory and the design of health materials: A cognitive factors perspective. Patient Educ Couns. 2009;74:318–22. doi: 10.1016/j.pec.2008.11.005. [DOI] [PubMed] [Google Scholar]
- 14.van Merriënboer JJG, Sweller J. Cognitive load theory in health professional education: Design principles and strategies. Med Educ. 2010;44:85–93. doi: 10.1111/j.1365-2923.2009.03498.x. [DOI] [PubMed] [Google Scholar]
- 15.Alberti TL, Nannini A, Associate F. Patient comprehension of discharge instructions from the emergency department: A literature review. J Am Acad Nurse Pract. 2012;00:1–9. doi: 10.1111/j.1745-7599.2012.00767.x. [DOI] [PubMed] [Google Scholar]
- 16.Szpiro KA, Harrison MB, Van Den Kerkhof EG, Lougheed MD. Patient education in the emergency department. Adv Emerg Nurs J. 2008;30:34–49. [Google Scholar]
- 17.Butcher KR. Learning from text with diagrams: Promoting mental model development and inference generation. J Educ Psychol. 2006;98:182–97. [Google Scholar]
- 18.Mayer RE, Anderson RB. Animations need narrations: An experimental test of a dual-coding hypothesis. J Educ Psychol. 1991;83:484–90. [Google Scholar]
- 19.Baddeley A. The episodic buffer: A new component of working memory? Trends in cognitive sciences. 2000;4:417–23. doi: 10.1016/s1364-6613(00)01538-2. [DOI] [PubMed] [Google Scholar]
- 20.Mayer RE. Multimedia learning. Psychol Learn Motiv. 2002;41:85–139. [Google Scholar]
- 21.Mayer RE, Moreno R. Nine ways to reduce cognitive load in multimedia learning. Educ Psychol. 2003;38:43–52. [Google Scholar]
- 22.Clark RC, Mayer RE. e-learning and the Science of Instruction: Proven guidelines for consumers and designers of multimedia learning. 2nd edn. San Francisco: Wiley & Sons; 2007. [Google Scholar]
- 23.Brewer N, Harvey S, Semmler C. Improving comprehension of jury instructions with audio-visual presentation. Appl Cogn Psychol. 2004;18:765–76. [Google Scholar]
- 24.Pinsky LE, Wipf JE. Innovations in education and clinical practice: A picture is worth a thousand words: Practical use of videotape in teaching. J Gen Intern Med. 2000;15:805–10. doi: 10.1046/j.1525-1497.2000.05129.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Kendon A. Do gestures communicate? A review. Res Language Soc Interact. 1994;27:175–200. [Google Scholar]
- 26.Marcus N, Cooper M, Sweller J. Understanding instructions. J Educ Psychol. 1996;88:49–63. [Google Scholar]
- 27.Grunwald T, Corsbie-Massay C. Guidelines for cognitively efficient multimedia learning tools: Educational strategies, cognitive load, and interface design. Acad Med. 2006;81:213–23. doi: 10.1097/00001888-200603000-00003. [DOI] [PubMed] [Google Scholar]
- 28.Delgado M, Gindle A, Pallin D, Camargo CA. Multicenter study of preferences for health education in the emergency department. Acad Emerg Med. 2010;17:652–8. doi: 10.1111/j.1553-2712.2010.00764.x. [DOI] [PubMed] [Google Scholar]