

Abstract
Background:
Six-min walk test (6MWT), a simple functional capacity evaluation tool used globally to determine the prognosis and effectiveness of any therapeutic/medical intervention. However, variability in reference equations derived from western population (due to racial and ethnicity variations) hinders from adequate use of 6MWT clinically. Further, there are no valid Indian studies that predict reference values for 6-min walk distance (6MWD) in healthy Indian normal.
Objective:
We aimed for framing individualized reference equations for 6MWT in healthy Indian population.
Materials and Methods:
Anthropometric variables (age, weight, height, and body mass index (BMI)) and 6-min walk in a 30 m corridor were evaluated in 125 subjects (67 females) in a cross-sectional trial.
Results:
6MWD significantly correlated with age (r = -0.29), height (r = 0.393), weight (r = 0.08), and BMI (r = -0.17). The gender specific reference equations for healthy Indian individuals were: (1) Males: 561.022 - (2.507 × age [years]) + (1.505 × weight [kg]) - (0.055 × height [cm]). R2 = 0.288. (2) Indian females: 30.325 - (0.809 × age [years]) - (2.074 × weight [kg]) + (4.235 × height [cm]). R2 = 0.272. Though the equations possess a small coefficient of determination and larger standard error estimate, the former applicability to Indian population is justified.
Conclusion:
These reference equations are probably most appropriate for evaluating the walked capacity of Indian patients with chronic diseases.
KEY WORDS: 6-min walk distance, functional capacity, Indian population, reference value, walk test
INTRODUCTION
Six — min walk test (6 MWT) is the most common clinical and research tool for the evaluation of functional exercise capacity in chronic pulmonary disabled patients.[1,2,3,4,5,6,7,8,9] It reflects the capacity of the individual to perform activities of daily living.[1] Recently, research elucidates that 6MWT accurately estimates maximal oxygen uptake.[2] Demographic, anthropometric, clinical, psychological, and physiological characteristics can affect the test performance in healthy elderly subjects and in patients with cardiopulmonary diseases.[3] The results may be influenced by confounding factors such as clinician's/investigator's encouragement and subject's motivation.[1,5,6,7,8] Accordingly, the 6-min walk distance (6MWD) varies widely, even among healthy subjects.[9] The American Thoracic Society (ATS) recommends that researchers should establish specific reference values for each continental population globally.[3] Recent studies have elaborated 6MWT reference values for various populations.[1,5,6,7,8,9] However, these equations used in western populations may not necessarily be applicable to Indian subjects.[10]
After a detailed literature review, only one Indian cross-sectional study is available demonstrating the reference values of predicted 6 MWD for Indian population.[10] However, heterogeneity and low sample clouds the validity of these equations in Indian clinical arena.[10] There are no valid reference equations for predicting 6MWD in older Indian subjects (25-80 years). In the present study, we assessed 6MWD in a population-based sample of Indian healthy subjects aged 25-80 years and established gender specific reference equations to predict 6MWD. We also compared the 6MWD values measured with the commonly used reference values derived from western population.[1]
MATERIALS AND METHODS
Participants
We studied 125 healthy subjects over 25 years of age. Volunteers were recruited from students, patient's caregivers, and employees of a tertiary care teaching hospital through advertising in hospital notice board. The volunteers were stratified into the following categories, based on age: 25-39 years (a), 40-49 years (b), 50-59 years (c), 60-69 years (d), and 70-79 years (e). All subjects selected for study presented clinical stability, defined as the absence of any acute disease during the 6 weeks preceding the study.[1] Subjects with a current diagnosis of cardiovascular/respiratory disease, those with any health problem that might interfere with the ability to perform physical exercises (e.g., impaired cognition, metabolic, neuromuscular or musculoskeletal diseases or use of walking aids), and those regularly using medications for chronic diseases were excluded from the study. However, former smokers without tobacco-related diseases were included in the study (n = 3).
Total body weight (kg) and body height (cm) were measured according to standard techniques, with the subjects wearing light clothing and no shoes.[1] Measurements were made with a calibrated weighing machine (0.1 kg of precision) and with a fixed wall inch tape (0.5 cm of precision). The body mass index (BMI) was calculated by the standard formula (body mass (kg)/body height (m)2). The risk for cardiovascular events during exercise was assessed using risk stratification chart according to earlier recommendations.[3,11] The study design was approved by the Human Research Ethics Committee of our Hospital, and all subjects gave written informed consent to participate.
6MWT
6MWT was administered and adhered to the guidelines of American Thoracic Society (ATS) standards.[3] The subjects were given orientation to the test on the day. Each subject was instructed to walk as far as possible during a 6 min period over a 30 m course in an indoor hospital corridor. The course was identified by two traffic cones and the corridor was marked every 3 m according to ATS standards.[3] Instructions and verbal encouragement given to the subjects were standardized.[1] Encouragement was given every minute until subject exhaustion. Reason for stopping the test (either subject or therapist's fatigue perception, breathlessness, hemodynamic instability) was documented. Chest pain, intolerable dyspnea, dizziness, leg cramps, diaphoresis, and fall were additional criteria for immediately stopping the test. Before and after the walk test, the following data were obtained: pulse rate; respiratory rate; blood pressure; and dyspnea/leg effort, using the modified Borg scale. Measured 6MWD values were compared with predicted values from reference equations devised by Enright et al.[4]
Statistical analysis
Statistical analysis was performed using the Statistical Package for Social Sciences (SPSS) 12.01 (SPSS, Chicago, IL, USA). Data were reported as mean ± standard deviation (SD) or as median (interquartile range). The following tests were performed: Pearson or Spearman coefficient to evaluate the correlations between the observed variables and multiple linear regressions were sought among 6 MWD and anthropometric attributes. Residual statistics for goodness of fit and residual plots for normalization and generalization were sought. We compared predicted 6MWD by our Indian predicted equation and western (proposed by Paul Enright) prediction and agreement between both the predicted 6MWD derived was analyzed by Bland-Altman plots.[1]
RESULTS
Of the 125 subjects evaluated, 67 (52.75%) were females. The mean age of the sample was 46 ± 16 years. Mean BMI was within the normal range (23.96 ± 4.35 kg/m2). The prevalence of smoking was 2.4% (n = 3). The mean 6MWD was 495.09 ± 83.85 m (range: 294-691 m). The characteristics of the 125 subjects are summarized in [Table 1].
Table 1.
Characteristics of the subjects (mean±SD)
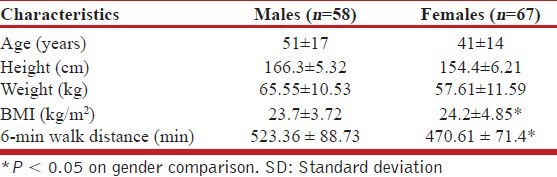
Weight, height, and 6MWD were greater in males than in females (P = 0.00). There was no significant difference between males and females in terms of BMI (P = 0.527).
Bivariate analysis showed that 6MWD correlated significantly (P < 0.05) with age, height, and BMI. In the multiple linear regression analysis, age and anthropometric traits were selected as predictors of 6MWD. The individual equations for both the gender yielded are (by enter method) shown in [Table 2]. The anthropometric traits and age jointly explains 28% of the total variance in 6MWD (the coefficient of determination, R2 = 0.28).
Table 2.
Reference equations for healthy Indian individuals (30-80 years)

The standard error estimate of the equations is projected in [Table 2]. The smaller coefficient of determination (R2) and larger residual SD [Table 2] shows a lesser fit of the Indian prediction equations for generalization. The residual statistics for both the equations are projected in [Table 3]. The average values of predicted and observed residual values predict that still our Indian predicted equations holds better ability in generalization to Indian population rather than other equations.[1] Further the normalization of the population is demonstrated by the low values of standard and studentized residuals [Table 3]. The plot of residuals versus predicted for both male and female equations does not have a systemic appearance as projected in [Figure 1a and b].
Table 3.
Residual statistical analysis of Indian gender specific equations for 6 MWD
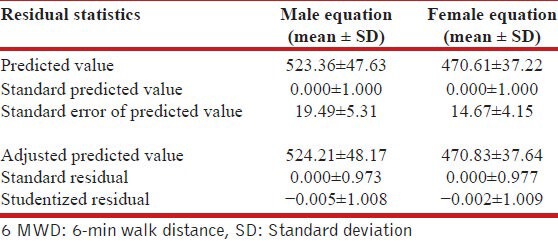
Figure 1.
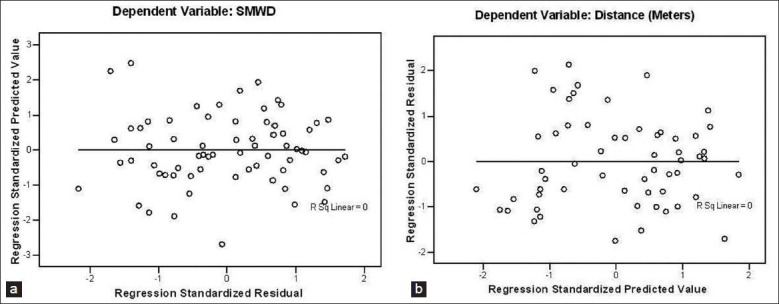
(a) Scatter plot showing the relation between predicted and observed residual 6-min walk distance of male equation (b) Scatter plot showing the relation between predicted and observed residual 6-min walk distance of female equation
When the predicted 6MWD by Indian predicted equations is compared with western predicted equations, there was a low agreement between both the predicted equations. This poor agreement between predicted distances by western equation and our Indian predicted equations is demonstrated by Bland-Altman plot in [Figure 2].
Figure 2.
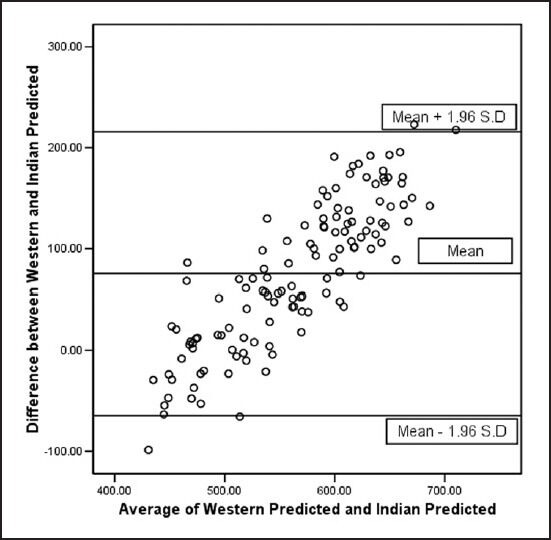
Bland-Altman plot demonstrating agreement between western and Indian equations for predicted maximal 6-min walk distance
DISCUSSION
To our knowledge, the present study is the first larger sample Indian trial to investigate predicted values and potential demographic and anthropometric determinants of 6MWD in the Indian older population and to propose a predictive equation. Further, this study adds to the evidence that the predictive distances derived from western population would not apply for Indian population.[1,10]
Reference equations would permit a more appropriate functional evaluation of Indian patients with chronic pulmonary diseases. The equations derived from other populations commonly overestimated 6MWD in relation to the values obtained for our Indian subjects.[2,10] Since we adhered to the ATS guidelines for the 6MWT, we believe that our derived equations would predict 6MWD precisely in accordance with the predicted equations derived from western population.[3]
Age, height, weight, and BMI significantly influenced the 6MWD of our volunteers. These findings agree with previous studies.[1,2,3,4,5,6,7,8,9] The negative influence of advanced age on the 6MWD might be explained by the gradual reduction in muscle mass, muscle strength, and maximal oxygen uptake that typically occurs with aging.
In our study, the gender difference in the 6MWD may be best explained by the greater absolute muscle strength, muscle mass, and height of men compared to women. This is in agreement with the earlier trials.[1,9] Our finding that height influences 6MWD agrees with the correlations between height and 6MWD reported by earlier literature.[1,2,3,4,5,6,7,8,9] This can be attributed to the greater stride length of taller individuals. Though, literature proposes that 6MWD being shorter in subjects with greater body weight or higher BMI; we found only a weak correlation between BMI, weight, and 6MWD. Previous literature also has proved the nonlinearity of the correlation.[4,9]
In our study, the gender specific reference equations for predicting 6MWD demonstrated a squared correlation coefficient of 0.28, similar to values reported in previous studies, in which it ranged from 0.2 to 0.67.[1] Our Indian predicted equations for 6MWD shows moderate statistical confidence for generalization to our Indian population. This moderate significance may be due to the individual differences in physical activity, musculoskeletal growth, and psychological status.[9,11]
We observed that the equations devised by Enright et al., overestimated 6MWD in relation to the values obtained for our sample.[4] This may be multifactorial such as motivation, timing of the trial, psychological status, encouragement, corridor length, and shape.[11]
There was a poor agreement between western predicted equations and Indian predicted equations for predicted 6MWD. This may be attributed to the racial, cultural differences, ethnic variances, and physical activity. Potential sources of 6MWD variance other than age, gender, or height should be considered. One such source is the psychological status related to exercise capacity in healthy subjects.[1] Other potential sources are differences in earlier functional capacities, peripheral muscle conditioning, and pulmonary function.[3,4,9]
Some potential limitations of our study should be considered. Although subjects were selected consecutively on the basis of inclusion criteria, such a convenience sample might have introduced a bias. In spite of the fact, convenience samples have often been included in studies evaluating reference values for 6MWD.[1,2,3,4,5,6,7,8,9,12] To overcome this limitation, our study should be repeated with larger sample in near future.
CONCLUSION
We conclude that 6MWD presents substantial variability in Indian healthy subjects aged 25-80 years. However, an important part of the variability was adequately predicted by demographic and anthropometric attributes. We observed that equations devised for western population overestimated the 6MWD measured in Indian subjects. Our study resulted in gender specific reference equations for the prediction of 6MWD in healthy Indian subjects. We conclude that our equations may facilitate the assessment of Indian patients with the chronic pulmonary diseases that affect their functional capacity.
ACKNOWLEDGMENT
We thank Ms. Saranya, postgraduate student, PSG College of Physiotherapy, Peelamedu, Coimbatore for being a part in acquaintance of 6-min walk test data and recruitment of volunteers.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Iwama AM, Andrade GN, Shima P, Tanni SE, Godoy I, Dourado VZ. The six-minute walk test and body weight-walk distance product in healthy Brazilian subjects. Braz J Med Biol Res. 2009;42:1080–5. doi: 10.1590/s0100-879x2009005000032. [DOI] [PubMed] [Google Scholar]
- 2.Ross RM, Murthy JN, Wollak ID, Jackson AS. The six minute walk test accurately estimates mean peak oxygen uptake. BMC Pulm Med. 2010;10:31. doi: 10.1186/1471-2466-10-31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. ATS statement: Guidelines for the six-minute walk test. Am J Respir Crit Care Med. 2002;166:111–7. doi: 10.1164/ajrccm.166.1.at1102. [DOI] [PubMed] [Google Scholar]
- 4.Enright PL, McBurnie MA, Bittner V, Tracy RP, McNamara R, Arnold A, et al. Cardiovascular health study. The 6-min walk test: A quick measure of functional status in elderly adults. Chest. 2003;123:387–98. doi: 10.1378/chest.123.2.387. [DOI] [PubMed] [Google Scholar]
- 5.Camarri B, Eastwood PR, Cecins NM, Thompson PJ, Jenkins S. Six minute walk distance in healthy subjects aged 55-75 years. Respir Med. 2006;100:658–65. doi: 10.1016/j.rmed.2005.08.003. [DOI] [PubMed] [Google Scholar]
- 6.Chetta A, Zanini A, Pisi G, Aiello M, Tzani P, Neri M, et al. Reference values for the 6-min walk test in healthy subjects 20-50 years old. Respir Med. 2006;100:1573–8. doi: 10.1016/j.rmed.2006.01.001. [DOI] [PubMed] [Google Scholar]
- 7.Poh H, Eastwood PR, Cecins NM, Ho KT, Jenkins SC. Six-minute walk distance in healthy Singaporean adults cannot be predicted using reference equations derived from Caucasian populations. Respirology. 2006;11:211–6. doi: 10.1111/j.1440-1843.2006.00820.x. [DOI] [PubMed] [Google Scholar]
- 8.Troosters T, Gosselink R, Decramer M. Six minute walking distance in healthy elderly subjects. Eur Respir J. 1999;14:270–4. doi: 10.1034/j.1399-3003.1999.14b06.x. [DOI] [PubMed] [Google Scholar]
- 9.Casanova C, Celli BR, Barria P, Casas A, Cote C, de Torres JP, et al. The 6-min walk distance in healthy subjects: Reference standards from seven countries. Eur Respir J. 2011;37:150–6. doi: 10.1183/09031936.00194909. [DOI] [PubMed] [Google Scholar]
- 10.Sivaranjini S, Vanamail P, Eason J. Six minute walk test in people with tuberculosis sequelae. Cardiopulm Phys Ther J. 2010;21:5–10. [PMC free article] [PubMed] [Google Scholar]
- 11.Meyer FJ, Borst MM, Buschmann HC, Ewert R, Friedmann-Bette B, Ochmann U, et al. Exercise testing in respiratory medicine. Pneumologie. 2013;67:16–34. doi: 10.1055/s-0032-1325901. [DOI] [PubMed] [Google Scholar]
- 12.Kervio G, Carre F, Ville NS. Reliability and intensity of the six-minute walk test in healthy elderly subjects. Med Sci Sports Exerc. 2003;35:169–74. doi: 10.1097/00005768-200301000-00025. [DOI] [PubMed] [Google Scholar]