

Abstract
Rising population of diabetic individuals across the world has become a big concern to the society. The persistent hyperglycemia may affect each and every tissue and consequently results in morbidity and eventually mortality in diabetic patients. A direct negative response of diabetes has been observed on oral tissues with few contradictions however, little are known about effect of diabetes on dental implant treatment and the consequent results. Many studies concerned with osteointegration and prognosis of dental implant in diabetic patients have been conducted and published since 1994. These studies have been critically reviewed to understand the impact of diabetes on the success of dental implant and the factors to improve osseointegration and consequently survival of dental implant in diabetic patients. Theoretical literatures and studies in diabetic animals substantiate high failure rate of implants but most of clinical studies indicated statistically insignificant failure of dental implants even in moderately uncontrolled diabetic patients. Success of dental implant in well and fairly controlled diabetic patients with proper treatment planning, prophylactic remedies and adequate postsurgical maintenance appears as good as normal individuals.
Keywords: Dental implant, hyperglycemia, osteointegration
INTRODUCTION
The recent studies in China[1] and India[2] has shown that the number of diabetic individuals has surpassed the estimate of IDF-2009[3] i.e., approximately 285 million people worldwide will have diabetes in 2010 and by 2030, 438 million people of adult population is expected to have diabetes with majority of effected population from China, India and USA.
The comforts like natural dentition, conservative treatment compared to teeth supported FPDs and long term success for the edentulous patients, as well as partially edentulous patients have made dental implants supported prosthetic treatment as an attractive substitute to traditional removable or fixed dental prosthesis besides being costly and lengthy procedures with surgical intervention.[4,5,6] The growing economy of developing nations like china and India has also been playing a key role in popularizing the implant dental treatment. In light of above facts, the dental fraternity may encounter with more number of diabetic patients for dental implant treatments.
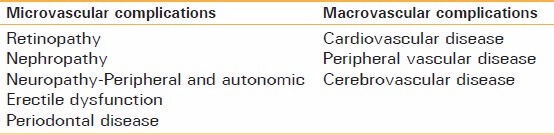
Diabetes mellitus is a chronic disorder of carbohydrate metabolism characterized by hyperglycemia, reflecting distortion in physiological equilibrium in utilization of glucose by tissue, liberation of glucose by liver and production-liberation of pancreatic anterior pituitary and adrenocortical hormone. The debilitating characteristic of diabetes mellitus was known as early as in second century AD, when Areteous named it as diabetes means “a siphon” as he perceived that the condition was characterized by melting down of flesh and limb into urine.[7] Various modern research and discoveries have shown that diabetes mellitus, more or less, affects every tissues of body directly or indirectly through late complications [Table 1].[8] Concerning the effect on oral tissues, Loe.[9] recognized the periodontal disease as sixth major complication of diabetes. Number of studies has proved the adverse effect of chronic hyperglycemia on oral mucosa and with some controversies on alveolar bone.
Table 1.
Late-onset complications of diabetes
This review caters actual scenario to practicing dentists regarding success and failure of dental implant treatment in diabetic individuals observed by various studies. The experience based suggestions and experimental studies about increasing osteointegration and consequently improving success rate of dental implant treatment in diabetic patients have also been discussed.
Effect of diabetes on bone and osteointegration
The persistent hyperglycemia in diabetic individuals, inhibit osteoblastic activity and alters the response of parathyroid hormone that regulates metabolism of Ca and P,[10] decreases collagen formation during callus formation,[11] induces apoptosis in lining cells of bone[12] and increases osteoclastic activity[13,14] due to persistent inflammatory response. It also induces deleterious effect on bone matrix and diminishes growth and accumulation of extracellular matrix.[15] The consequent result is diminished bone formation during healing, which is observed in number of experimental animal studies.[16,17,18,19]
Type -1 diabetes causes decreased bone mineral density, as well as reduced bone formation and higher bone resorption[20] whereas Type -2 diabetes produces normal or greater bone mineral density in some patients.[21] It has been observed that insulin not only reduces the deleterious effect of hyperglycemia by controlling it but also stimulates osteoblastic activity. Hence, bone matrix formation in insulin treated experimental models is similar to control ones.[22]
Most of the studies have been performed in streptozotocin/alloxan induced diabetic experimental models (rat/rabbit) to observe osseointegration of implants. Histo-chemical/histomorphic/planimetric/biomechanical torque/manometric analysis showed that bone volume formed in diabetic animals was similar to non-diabetic animals[23] however, bone implant contact (BIC) in diabetic animals was lesser compared to non-diabetics.[24] The rate of mineral apposition in newly formed bone and bone density around implant was significantly less in uncontrolled diabetic animals.[25] The bone volume and bone density around implant in insulin controlled diabetic animals was observed similar or greater to non-diabetic but BIC was found significantly less[22,26,27,28,29,30](Even in insulin controlled diabetic animals).
Only few case studies for histological observation of dental implant osseointegration in human being have been reported. In one report,[31] an implant was placed and intended to support an overdenture in 65-year-old diabetic women was retrieved after 2 months due to prosthetically unfavorable condition. In histological analysis, no symptoms of implant failure recognized with 80% bone implant contact ratio. A case of diabetes mellitus type-2 having implant failure within 6 months, was reported by Park JB[32] with conclusion that osseointegration was not affected by diabetes mellitus as there was no sign and symptoms of failure before loading.
Success/failure of dental implants in diabetic patients
Most of the studies[43,44,46,48] observed slightly high percentage of early failure of implants in diabetics compared to late failure. Some reports[45,46,50] indicated increased failure rate within first year of placement of implant. The published retrospective and prospective studies data, retrieved through various sources from 1994 to 2011 [Table 2], indicated that the success rate of dental implants in diabetic patients were in range of 85.5-100% and were comparable to the non-diabetic patients. Most of the studies were of opinion that success rate in well/fairly controlled diabetics was either equal or insignificantly lower than normal individuals. Two studies[36,39], has taken chance to involve uncontrolled diabetic patients for dental implantation and observed encouraging results as early implant success was similar to non-diabetics. However, it is noteworthy that number of patients and implants placed (4 implants in 3 patients) in uncontrolled diabetics was quite low and all the patients selected were free of micro and macro-vascular complications. Only two studies[36,41] reported significantly high failure of implant in diabetic patients even when glucose level was adequately under control. One of these studies retrospectively included early, as well as late failures of implants over the period of 10 years but did not specify the glycemic control over that period. While other study, prospective in nature, observed significantly high early failures with probable reason that placement of multiple adjoining implants in diabetic patients increased the failure rates due to large wound, delayed healing and greater force posed over implants. Inadequate time (study period 90 days only) provided for osseointegration and regaining stability to implant in the study seems to be the cause of observing very high failure in diabetic patients.
Table 2.
Outcome of studies showing survival/success of dental implant in diabetic patients
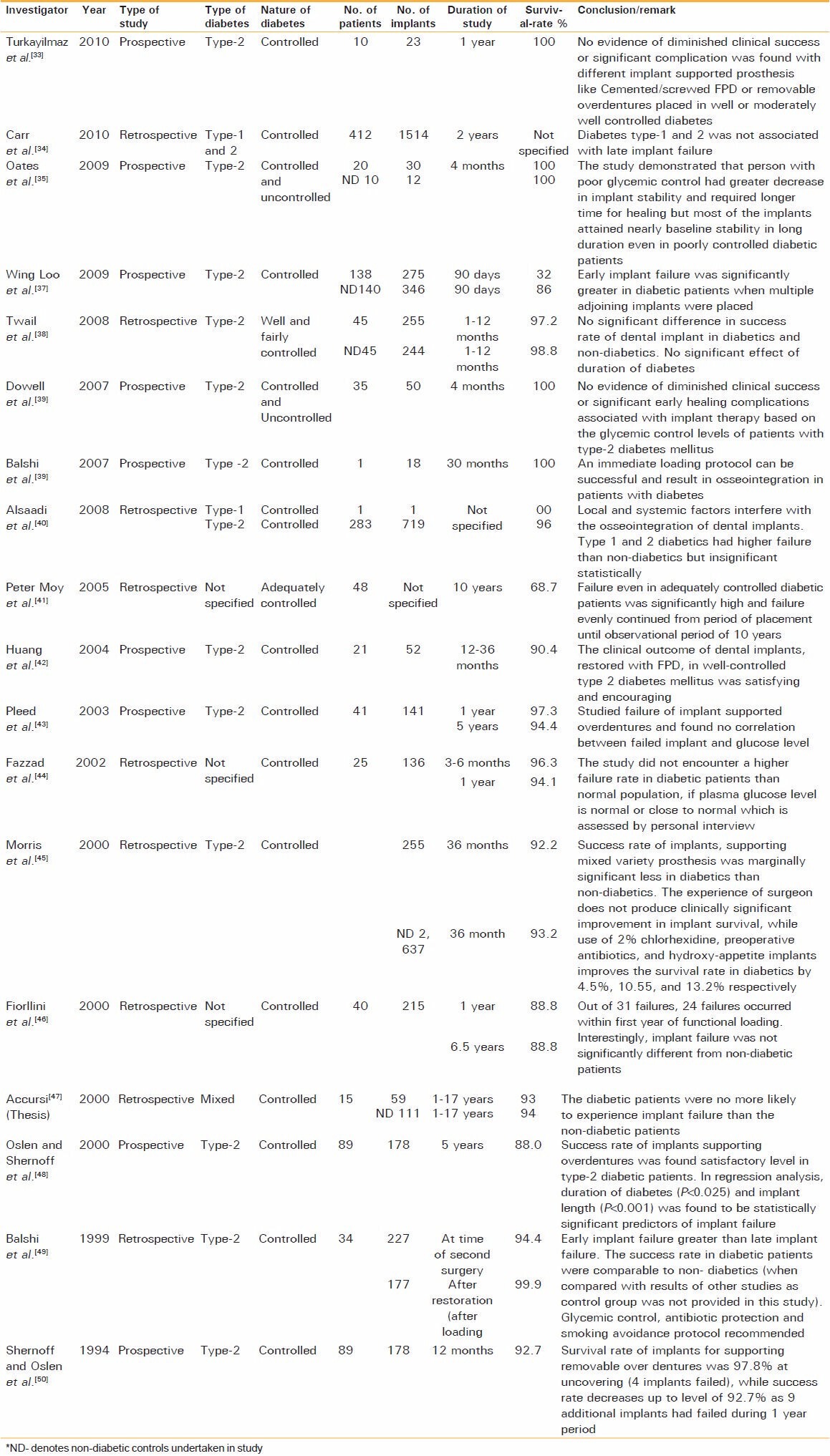
Most of the studies[43,44,46,48] observed slightly high percentage of early failure of implants in diabetics compared to late failure. Some reports[45,46,50] indicated increased failure rate within first year of loading suggesting the risk of implant failure is associated with uncovering of implants and early phase of implant loading. T W Oates observation[35] also supports high early failure in diabetic patients as such patients experienced low implant stability quotient (ISQ) in period of 2-12 weeks and lower the level of glycemic control, higher the amount of ISQ reduction and longer the duration of recovery in ISQ at base level was required. However, most of implants attained base level of stability within 4 months even in uncontrolled diabetic patients, if the patients were refrained with micro- and macro-vascular complications.
Duration of diabetes significantly affected the success of dental implant, observed in one study[48] while another did not demonstrate significantly higher late implant failures in diabetic patients even with longer duration. Overall lower success of implant in patients with diabetes of longer duration may be due to higher chance of micro-vascular complications which consequently lead to delayed healing around implants and hence higher early failure.
Few studies,[40] demonstrated significantly higher failure of implant in type-1 diabetic patients than patients with type-2 diabetes (in one study, only one implant placed in a person with diabetes type-1 and it failed i.e., failure rate = 100%, an extremely unlikely true estimate of risk). While one study[34] did not find any significant difference in late failure of dental implant in type-1 and type-2 diabetic patients. Higher failure rate in diabetic type-1 may be due to depletion of insulin in tissues whereas presence of insulin in tissues of type-2 diabetic individuals may reduce deleterious effect of hyperglycemia. There is no study exclusively reported the survival/success of implant in type-1 diabetes however, very few retrospective studies had subject with type-1 and type-2 diabetes but little number of type-1 diabetic subjects.
Immediate loading did not significantly affect the survival of dental implant in diabetic patients provided their plasma glucose level were under normal range.[37,39,44,45] Balshi SF[39] reported 100% survival of 18 implants after 2.5 years after placement followed by immediate loading with screwed retained fixed prosthesis in a 71-year-old diabetic patient. The study suggests that controlled mechanical stimuli over implant can be beneficial for osseointegration and implant survival.
The studies[37,45] observed lower survival of implant in diabetic patients of very old age group but difference was not statically significant. Although, none of the studies had compared success of implant in diabetic females and males but number of studies reported survival as good as in females compared to males in general population. The experience of surgeons and advance surgical process did not significantly affect success of dental implant in diabetics as observed in studies.[38,46]
Measures for improving success of dental implant in diabetics
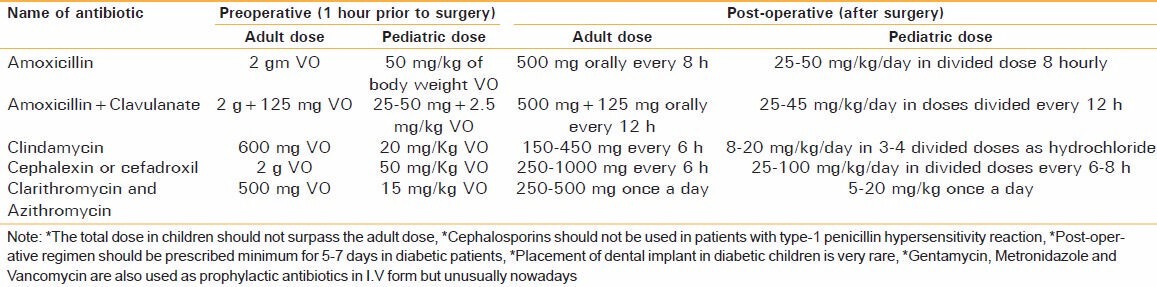
Good glycemic control, preoperative and post-operative, is required to achieve improved osseointegration in diabetics.[51] Prophylactic antibiotics [Table 3] have shown to be effective for success of dental implants in diabetic patients and use of 0. 12% chlorhexidine further improves the success rate.[45,48,49,50,51,52] Certain factors like implant surface characteristics (implant coated with bioactive material) and higher implant length and width has been shown to improve success rate of implant in diabetic patients. Some researcher has found positive results in experimental studies to improve osseointegration and results are yet to be verified in human being. In few studies,[53,54] it was observed that systemic administration of aminoguanidine reduced the deleterious effect of diabetes on osseointregration. Satana et al.[55] used rhFGF2 (recombinant human fibroblast growth factor-2) encapsulated with poly glycosylated poly lactide (PGLA) membrane in calvarial defect of diabetic rat and formation of normal bone level was observed in histomorphic analysis. Wang et al.,[56] in a study based on similar concept, used rrIGF-1(Recombinant rat insulin like growth factor) encapsulated with PGLA around Ti implant inserted in calvaria of diabetic rat. It was found in histomorphic analysis that diabetic rat with rrIGF-1 had higher BIC around the implant compare to rat without rrIGF-1 after 4-8 weeks of surgical placement. A recent hypothesis was made by Bai et al.[57] that adiponectin, an insulin sensitive adipokine may improve osseointregration in diabetic patients by infusing it systemically or using locally as it has shown potent anti-inflammatory properties and increased bone density by enhancing osteoblast and inhibiting osteoclast formation.
Table 3.
Prophylactic antibiotics and their doses
DISCUSSION
Most of the experimental studies have been indicated that the bone matrix formation and bone mineralization was almost equal in controlled diabetic and non-diabetic animals but BIC was lower even in controlled diabetic subjects. Number of studies has proposed and explained mechanism of deleterious effect of diabetes over wound healing and true association (osseointegration) of bone to implant surface [Figures 1 and 2]. However studies,[31,32] performed in humans specifically with diabetes type-2, observed insignificant effect over BIC and consequently good osseointegration of dental implant in controlled diabetic patients. As most of the experimental studies conducted in rats and rabbits, the architectural and compositional difference in bone, higher metabolic rate, very permissive bone healing, faster skeletal changes and bone turnover[58,59] may be the reason for the difference in results of experimental animals and humans. The difference in developing diabetes (alloxan or streptozotocin destruct beta cells of Langerhans consequently induces diabetes) in experimental animals and human being (type-2 diabetes develop due to glucose resistance at cellular level and higher level of glucose in tissue consequently suppress the function of beta cells of Langerhans in long duration) maybe one reason for the difference in BIC. The result of an experimental study in obese diabetic rat strengthens the above explanation, as no difference in BIC was observed in obese diabetic rat than normal one.[60]
Figure 1.
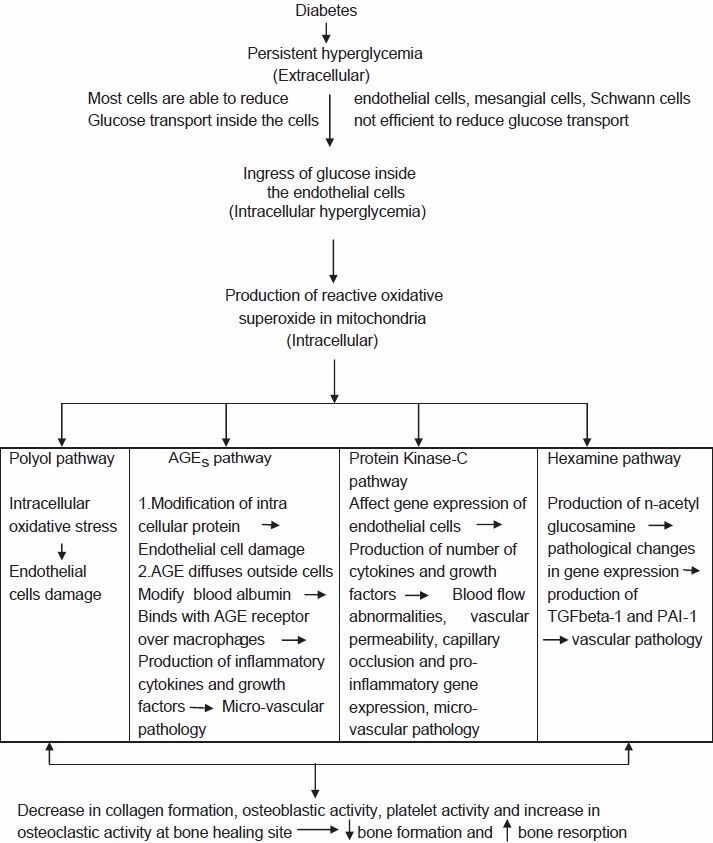
Mechanism of development of diabetic complication
Figure 2.
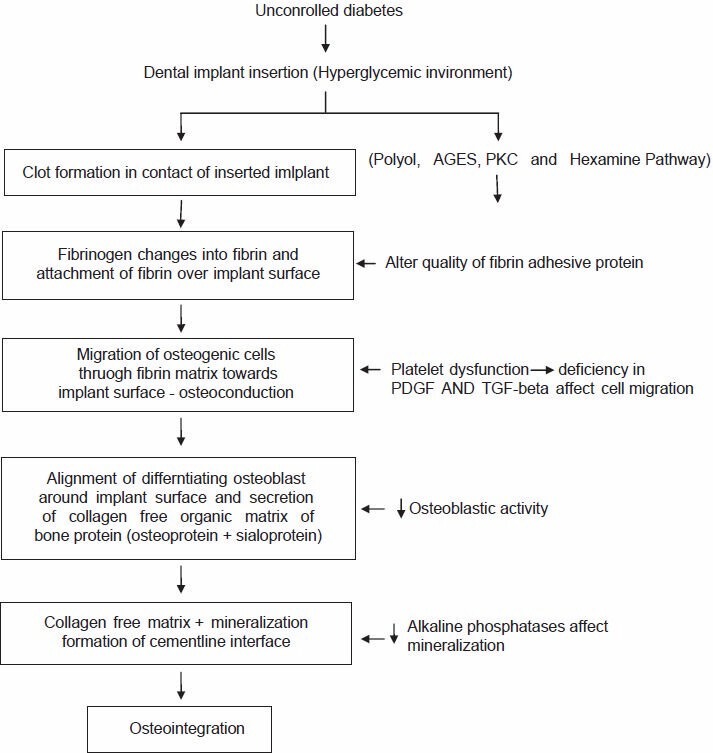
Possible effects of diabetes over mechanism of osteointegration
Most of clinical studies reported success of dental implant in diabetic individual as good as normal peoples. The reason may appear to be the inclusion of controlled diabetics in the almost all studies. The persistent hyperglycemia is responsible for development of micro-vascular complication and consequently the early or late implant failure. Hence the uncontrolled level of diabetes, reflected through measurement of glycated hemoglobin HbAc1 (indicate average glucose level over preceding 2-3 months period,[61] level 6 to 8 shows well controlled, 8.1 to 10 moderately controlled and more than 10 shows poorly controlled diabetes), persistent for longer duration with sign of micro-vascular complication may affect the success of dental implant significantly. However, none of the study included such uncontrolled patients or in other word it can be concluded that none of the surgeon had taken risk to insert dental implant in such human beings.
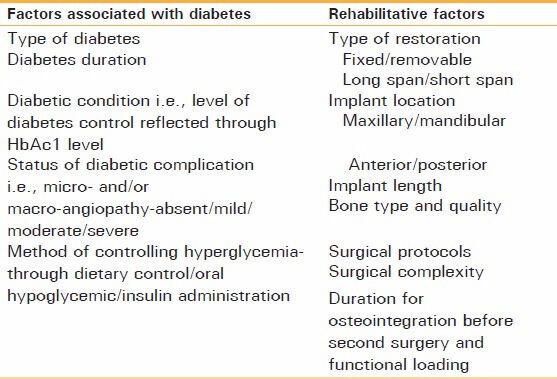
Even the fairly or moderately controlled diabetes persisting for very longer duration (more than 10 years) may produce complications and diminish the health of tissues. The compromised condition along with some unfavorable restorative factors may bargain the success of dental implants. Therefore, numerous factors associated with rehabilitation and diabetes itself, more or less, affect the survival of dental implant in diabetic subjects[62] [Table 4]. Cautious consideration of the mentioned factors during rehabilitation improves the success and hence the survival of dental implants in diabetic individuals.
Table 4.
Probable factors affecting survival of dental implants
CONCLUSION
The survival of dental implant in well/fairly controlled diabetic patients appears as good as in general population. Use of prophylactic antibiotic, longer duration of post surgical antibiotic course, chlorhexidine mouth rinse, bioactive material coated implants and implant with higher width and length seems to further improve the survival of implant in diabetic individuals. Systemic administration of some insulin sensitive adipokine and use of local growth factors have been found to improve osseointegration in diabetic experimental animals but yet to be verified in human beings. However, it is advisable to delay the placement of implant in poorly controlled diabetics till the control of diabetes. Longer duration prospective clinical studies with greater number of diabetic individuals and non-diabetic controls are still required to develop better understanding of impact of diabetes over dental implant success.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- 1.Yang W, Lu J, Wang J, Jia W, Ji L, Xiao J, et al. Prevalence of diabetes among men and women in China. N Engl J Med. 2010;362:1090–101. doi: 10.1056/NEJMoa0908292. [DOI] [PubMed] [Google Scholar]
- 2.Vaz NC, Ferreira AM, Kulkarni MS, Vaz FS. Prevalence of diabetes mellitus in a rural population of Goa, India. Natl Med J India. 2011;24:16–8. [PubMed] [Google Scholar]
- 3.IDF Diabetes Atlas. International Diabetes Federation. 4th ed. Quebec, Canada: Released at Montreal; 2009. [PubMed] [Google Scholar]
- 4.Machtei EE, Frankenthal S, Blumenfeld I, Gutmacher Z, Horwitz J. Dental implants for immediate fixed Restoration of partially edentulous patients: A 1-year Prospective pilot clinical trial in periodontally susceptible Patients. J Periodontol. 2007;78:1188–94. doi: 10.1902/jop.2007.060418. [DOI] [PubMed] [Google Scholar]
- 5.Levin L, Sadet P, Grossmann Y. A retrospective evaluation of 1,387 single-tooth implants: 6-year Follow-up. J Periodontol. 2006;77:2080–3. doi: 10.1902/jop.2006.060220. [DOI] [PubMed] [Google Scholar]
- 6.Levin L, Nitzan D, Schwartz-Arad D. Success of dental Implants placed in intraoral block bone grafts. J Periodontol. 2007;78:18–21. doi: 10.1902/jop.2007.060238. [DOI] [PubMed] [Google Scholar]
- 7.Heath H, 3rd, Lambert PW, Service FJ, Arnaud SB. Calcium homeostasis and diabetes mellitus. J Clin Endocrinol Metab. 1979;49:462–6. doi: 10.1210/jcem-49-3-462. [DOI] [PubMed] [Google Scholar]
- 8.Mellado Valero A, FerrerGarcía JC, Herrera Ballester A, Labaig Rueda C. Effects of diabetes on the osseointegration of dental implants. Med Oral Patol Oral Cir Bucal. 2007;12:E38–43. [PubMed] [Google Scholar]
- 9.Loe H. Periodontal disease: Sixth complication of diabetes mellitus. Diabetes Care. 1993;16:329–34. [PubMed] [Google Scholar]
- 10.Santana RB, Xu L, Babakhanlou C, Amar S, Graves DT. A role for advanced glycation end products in diminished bone healing in type 1 Diabetes. Diabetes. 2003;52:150–210. doi: 10.2337/diabetes.52.6.1502. [DOI] [PubMed] [Google Scholar]
- 11.Gooch HL, Hale JE, Fujioka H, Balian G, Hurwitz SR. Alterations of cartilage and collagen expression during fracture healing in experimental diabetes. Connect Tissue Res. 2000;41:81–5. doi: 10.3109/03008200009067660. [DOI] [PubMed] [Google Scholar]
- 12.He H, Liu R, Desta T, Leone C, Gerstenfeld LC, Graves DT. Diabetes causes decrease osteoclastogenesis, reduced bone formation and enhanced apoptosis of osteoblastic cells in bacteria stimulated bone loss. Endocrinology. 2004;145:447–52. doi: 10.1210/en.2003-1239. [DOI] [PubMed] [Google Scholar]
- 13.Liu R, Bal HS, Desta T, Behl Y, Graves DT. Tumor necrosis factor alpha mediates enhanced apoptosis of matrix-producing cells and impairs diabetic healing. Am J Pathol. 2006;168:757–64. doi: 10.2353/ajpath.2006.050907. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Kayal RA, Tsatsas D, Bauer MA, Allen B, Al-Sebaei MO, Kakar S, et al. Diminished bone formation during diabetic fracture healing is related to the premature resorption of cartilages associated with increased osteoclast activity. J Bone Miner Res. 2007;22:560–3. doi: 10.1359/jbmr.070115. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Weiss RE, Gora A, Nimni ME. Abnormalities in the biosynthesis of cartilage and bone proteoglycans in experimental diabetes. Diabetes. 1981;30:670–7. doi: 10.2337/diab.30.8.670. [DOI] [PubMed] [Google Scholar]
- 16.Nyomba BL, Verhaegue J, Tomaste M, Lissens W, Bouillon RB. Bone mineral homeostasis in spontaneously diabetic BB rats. Abnormal vitamin D metabolism and impaired active intestinal calcium absortion. Endocrinology. 1989;124:565–72. doi: 10.1210/endo-124-2-565. [DOI] [PubMed] [Google Scholar]
- 17.Beam HA, Parsons JR, Lin SS. The effects of blood glucose control upon fracture healing in the BB Wistar rat with diabetes mellitus. J Orthop Res. 2002;20:1210–6. doi: 10.1016/S0736-0266(02)00066-9. [DOI] [PubMed] [Google Scholar]
- 18.Gebauer GP, Lin SS, Beam HA, Vieira P, Parsons JR. Low-intensity pulsed Ultrasound increases the fracture callus strength in diabetic BB Wistar rats but does not affect cellular proliferation. J Orthop Res. 2002;20:587–92. doi: 10.1016/S0736-0266(01)00136-X. [DOI] [PubMed] [Google Scholar]
- 19.Lu H, Kraut D, Gerstenfeld LC, Graves DT. Diabetes interferes with the bone formation by affecting the expression of transcription factors that regulate osteoblast differentiation. Endocrinology. 2003;144:346–52. doi: 10.1210/en.2002-220072. [DOI] [PubMed] [Google Scholar]
- 20.Levin M, Boisseau V, Avioli L. Effects of diabetes mellitus on bone mass in juvenile and adult onset-diabetes. N Engl J Med. 1976;294:241–5. doi: 10.1056/NEJM197601292940502. [DOI] [PubMed] [Google Scholar]
- 21.Krakauer J, McKenna M, Burderer N, Rao D, Whitehouse F, Parfitt A. Bone loss and bone turnover in diabetes. Diabetes. 1995;44:775–82. doi: 10.2337/diab.44.7.775. [DOI] [PubMed] [Google Scholar]
- 22.Locatto ME, Abranzon H, Caferra D, Fernández MC, Alloatti R, Puche RC. Growth and development of bone mass in untreated alloxan diabetic rats. Effects of collagen glycosilation and parathyroid activity on bone turnover. Bone Miner. 1993;23:129–44. doi: 10.1016/s0169-6009(08)80049-9. [DOI] [PubMed] [Google Scholar]
- 23.McCracken MS, Aponte-Wesson R, Chavali R, Lemons JE. Bone associated with implants in diabetic and insulin-treated rats. Clin Oral Implants Res. 2006;17:495–500. doi: 10.1111/j.1600-0501.2006.01266.x. [DOI] [PubMed] [Google Scholar]
- 24.Nevins ML, Karimbux NY, Weber HP, Giannobile WV, Fiorellini JP. Wound healing in endosseous implants in experimental diabetes. Int J Oral Maxillofac Implants. 1998;13:620–9. [PubMed] [Google Scholar]
- 25.Hasegawa H, Ozawa S. Type 2 diabetes impairs implant osseointegration capacity in rats. Int J Oral Maxillofac Implants. 2008;23:237–46. [PubMed] [Google Scholar]
- 26.Shyng YC, Devlin H, Ou KL. Bone formation around immediately placed oral implants in diabetic rats. Int J Prosthodont. 2006;19:513–24. [PubMed] [Google Scholar]
- 27.Siqueira JT, Cavalher-Machado SC, Arana-Chavez VE, Sannomiya P. Bone formation around titanium implants in the rat tibia: Role of insulin. Implant Dent. 2003;12:242–51. doi: 10.1097/01.id.0000074440.04609.4f. [DOI] [PubMed] [Google Scholar]
- 28.de Morais JA, Trindade-Suedam IK, Pepato MT, Marcantonio E, Jr, Wenzel A, Scaf G. Effect of diabetes mellitus and insulin therapy on bone density around osseointegrated dental implants: A digital subtraction radiography study in rats. Clin Oral Implants Res. 2009;20:796–801. doi: 10.1111/j.1600-0501.2009.01716.x. [DOI] [PubMed] [Google Scholar]
- 29.Kwon PT, Rahman SS, Kim DM, Kopman JA, Karimbux NY, Fiorellini JP. Maintenance of osseointegration utilizing insulin therapy in a diabetic rat model. J Periodontol. 2005;76:621–6. doi: 10.1902/jop.2005.76.4.621. [DOI] [PubMed] [Google Scholar]
- 30.Fiorellini JP, Nevins ML, Norkin A, Weber HP, Karimbux NY. The effect of insulin therapy on osseointegration in a diabetic rat model. Clin Oral Implants Res. 1999;10:362–9. doi: 10.1111/j.1600-0501.1999.tb00011.x. [DOI] [PubMed] [Google Scholar]
- 31.Bugea C, Luongo R, Di Iorio D, Cocchetto R, Celletti R. Bone contact around osseointegrated implants: Histologic analysis of a dual-acid-etched surface implant in a diabetic patient. Int J Periodontics Restorative Dent. 2008;28:145–51. [PubMed] [Google Scholar]
- 32.Park JB. Bone healing at a failed implant site in a type II diabetic patient: Clinical and histologic evaluations: A case report. J Oral Implantol. 2007;33:28–32. doi: 10.1563/0-826.1. [DOI] [PubMed] [Google Scholar]
- 33.Turkyilmaz I. One-year clinical outcome of dental implants placed in patients with type-2 diabetes mellitus: A case. Implant Dent. 2010;19:323–9. doi: 10.1097/ID.0b013e3181e40366. [DOI] [PubMed] [Google Scholar]
- 34.Carr AB. Implant location and radiotherapy are the only factors linked to 2-year implant failure. J Evid Based Dent Pract. 2010;10:49–51. doi: 10.1016/j.jebdp.2009.11.025. [DOI] [PubMed] [Google Scholar]
- 35.Oates TW, Dowell S, Robinson M, McMahan CA. Glycemic control and implant stabilization in type 2 diabetes mellitus. J Dent Res. 2009;88:367–71. doi: 10.1177/0022034509334203. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Loo WT, Jin LJ, Cheung MN, Wang M. The impact of diabetes on the success of dental implants and periodontal healing. Afr J Biotechnol. 2009;8:5122–7. [Google Scholar]
- 37.Tawil G, Younan R, Azar P, Sleilati G. Conventional and advanced implant treatment in the type II diabetic patient: Surgical protocol and long-term clinical results. Int J Oral Maxillofac Implants. 2008;23:744–53. [PubMed] [Google Scholar]
- 38.Dowell S, Oates TW, Robinson M. Implant success in people with type- 2 diabetes mellitus with varying glycemic control. J Am Dent Assoc. 2007;138:355–61. doi: 10.14219/jada.archive.2007.0168. [DOI] [PubMed] [Google Scholar]
- 39.Balshi SF, Wolfinger GJ, Balshi TJ. An examination of immediately loaded dental implant stability in the diabetic patient using resonance frequency analysis (RFA) Quintessence Int. 2007;38:271–9. [PubMed] [Google Scholar]
- 40.Alsaadi G, Quirynen M, Komárek A, van Steenberghe D. Impact of local and systemic factors onthe incidence of oral implant failures, up to abutment connection. J Clin Periodontol. 2007;34:610–7. doi: 10.1111/j.1600-051X.2007.01077.x. [DOI] [PubMed] [Google Scholar]
- 41.Moy PK, Mediana D, Shetty V, Aghloo TL. Dental implant failure rates and associated factors. Int J Oral Maxillofac Implants. 2005;20:569–77. [PubMed] [Google Scholar]
- 42.Huang JS, Zhou L, Song GB. Dental implants in patients with Type 2 diabetes mellitus: A clinicalstudy. Shanghai Kou Qiang Yi Xue. 2004;13:441–3. [PubMed] [Google Scholar]
- 43.Peled M, Ardekian L, Tagger-Green N. Dental implants in patients with type 2 diabetes mellitus: A clinical study. Implant Dent. 2003;12:116–22. doi: 10.1097/01.id.0000058307.79029.b1. [DOI] [PubMed] [Google Scholar]
- 44.Farzad P, Andersson L, Nyberg J. Dental implant treatment in diabetic patients. Implant Dent. 2002;11:262–7. doi: 10.1097/00008505-200207000-00011. [DOI] [PubMed] [Google Scholar]
- 45.Morris HF, Ochi S, Winkler S. Implant survival in patients with type 2 diabetes: Placement to 36 months. Ann Periodontol. 2000;5:157–63. doi: 10.1902/annals.2000.5.1.157. [DOI] [PubMed] [Google Scholar]
- 46.Fiorellini JP, Chen PK, Nevins M, Nevins ML. A retrospective study of dental implants in diabetic patients. Int J Periodontics Restorative Dent. 2000;20:366–73. [PubMed] [Google Scholar]
- 47.Accursi GE. Treatment outcomes with osseointegrated Branemark implants in diabetic patients: A retrospective study [thesis] Toronto (ON): University of Toronto; 2000. [Google Scholar]
- 48.Olson JW, Shernoff AF, Tarlow JL, Colwell JA. Dental endosseous implant assessments in a type 2 diabetic population: A prospective study. Int J Oral Maxillofac Implants. 2000;15:811–8. [PubMed] [Google Scholar]
- 49.Balshi TJ, Wolfinger GJ. Dental implants in the diabetic patient: A retrospective study. Implant Dent. 1999;8:355–9. doi: 10.1097/00008505-199904000-00005. [DOI] [PubMed] [Google Scholar]
- 50.Shernoff AF, Colwell JA, Bingham SF. Implants for type II diabetic patients: Interim report. VA Implants in Diabetes Study Group. Implant Dent. 1994;3:183–5. doi: 10.1097/00008505-199409000-00009. [DOI] [PubMed] [Google Scholar]
- 51.Ciancio SG, Lauciello F, Shibly O, Vitello M, Mather M. The effect of an antiseptic mouthrinse on implant maintenance: Plaque and peri-implant gingival tissues. J Periodontol. 1995;66:962–5. doi: 10.1902/jop.1995.66.11.962. [DOI] [PubMed] [Google Scholar]
- 52.Porras R, Anderson GB, Caffesse R, Narendran S, Trejo PM. Clinical response to 2 different therapeutic regimens to treat peri-implant mucositis. J Periodontol. 2002;73:1118–25. doi: 10.1902/jop.2002.73.10.1118. [DOI] [PubMed] [Google Scholar]
- 53.Guimarães RP, de Oliveira PA, Oliveira AM. Effects of induced diabetes and the administration of aminoguanidine in the biomechanical retention of implants: A study in rats. J Periodontal Res. 2011;46:691–6. doi: 10.1111/j.1600-0765.2011.01391.x. [DOI] [PubMed] [Google Scholar]
- 54.Kopman JA, Kim DM, Rahman SS, Arandia JA, Karimbux NY, Fiorellini JP. Modulating the effects of diabetes on osseointegration with aminoguanidine and doxycycline. J Periodontol. 2005;76:614–20. doi: 10.1902/jop.2005.76.4.614. [DOI] [PubMed] [Google Scholar]
- 55.Santana RB, Trackman PC. Controlled release of fibroblast growth factor 2 stimulates bone healing in an animal model of diabetes mellitus. Int J Oral Maxillofac Implants. 2006;21:711–8. [PubMed] [Google Scholar]
- 56.Wang F, Song YL, Li CX, Li DH, Zhang HP, Ma AJ, et al. Sustained release of insulin-like growth factor-1 from poly (lactide-co-glycolide) microspheres improves osseo-integration of dental implants in type 2 diabetic rats. Eur J Pharmacol. 2010;640:226–32. doi: 10.1016/j.ejphar.2010.04.024. [DOI] [PubMed] [Google Scholar]
- 57.Bai Y, Yin G, Luo E. Adiponectin may improve osseointegration of dental implants in T2D Patients. Med Hypotheses. 2011;77:192–4. doi: 10.1016/j.mehy.2011.04.008. [DOI] [PubMed] [Google Scholar]
- 58.Pearce AI, Richards RG, Milz S, Schneider E, Pearce SG. Animal models for implant biomaterial research in bone: A review. Eur Cell Mater. 2007;13:1–10. doi: 10.22203/ecm.v013a01. [DOI] [PubMed] [Google Scholar]
- 59.Nunamaker DM. Experimental models of fracture repair. Clin Orthop Relat Res. 1998;355:56–65. doi: 10.1097/00003086-199810001-00007. [DOI] [PubMed] [Google Scholar]
- 60.Casap N, Nimri S, Ziv E, Sela J, Samuni Y. Type 2 diabetes has minimal effect on osseointegration of titanium implants in Psammomysobesus. Clin Oral Implants Res. 2008;19:458–64. doi: 10.1111/j.1600-0501.2007.01495.x. [DOI] [PubMed] [Google Scholar]
- 61.Derr R, Garrett E, Stacy GA, Saudek CD. Is HbA (1c) affected by glycemic instability? Diabetes Care. 2003;26:2728–33. doi: 10.2337/diacare.26.10.2728. [DOI] [PubMed] [Google Scholar]
- 62.Michaeli E, Weinberg I, Nahlieli O. Dental implant in diabetic patients: Systemic and rehabilitative consideration. Quintessence Int. 2009;40:639–45. [PubMed] [Google Scholar]