

Abstract
Turmeric is dried rhizome of the perennial herbs curcumalonga. It is called Haldi in Hindi, turmeric in English, ukon in Japanese. It has been used in Asian Medicine since the second millennium BC. It's utility is referred to in the ancient Hindu script the Ayurveda. Pathogenesis of the OLP should be taken in consideration for the treatment point of view. The Cell mediated immunity to secondary antigenic change in oral mucous membrane is thought to play a major role in its pathogenesis modified keratocyte surface antigens are the primary target for cytotoxic cellular response. Curcumin also been shown to have immune modulatory effect involving activation of host macrophages and natural killer cells and modulation of lymphocytes mediated function.
Keywords: Antioxidants, lichenplanus, turmeric
INTRODUCTION
Lichen planus is a relatively common disorder, estimated to effect 0.5% to 2.0%of the general population. It is a chronic inflammatory disease affecting mucosal and cutanous tissue. Oral lichen planus occurs more frequently than the cutanous form and tends to be more resistant to any treatment.
It is believed to result from an abnormal T cell medicated immune response in which basal epithelial cells are recognized as foreign because of the change in the anitgenicity of their cell surface. The cause of this immune mediated basal cell damage is unknown.
It is unknown if lichen planus represents a single disease process or several closely related entities with severe clinical representation.[1]
It is often asymptomatic, the atrophic erosive form can cause symptoms ranging from burning sensation to severe pain, interfering with speaking, eating and swallowing.
Patients with symptoms requires treatment. Plaque and calculus deposits are associated with a significantly with a significantly higher incidence of erythematous and erosive gingival oral lichen planus. Good oral hygiene is essential and can enhance healing .[2]
The psychological profile of the oral lichen planus patients should also be taken in to account. Studies have reported higher level of anxiety, greater depression and increased psychic disorders oral lichen planus.
Various treatment regimens have been designed to improve management of symptomatic oral lichen planus but permanent cure is not yet possible.
The extract of curcumin plant have been a major ingredient of medicine since the time immemorial. It has been attributed a number of medicinal properties in the traditional systems of the medicine. Turmeric and its ingredients curcumin are being studied as chemo preventive agent that inhibits the development of oral cancer, curcumin and essential oil of turmeric have been found to inhibit many diseases processes through their ant inflammatory, antioxidant and anticancer properties. Hence this was under taken to investigate the role of curcumin longa as an alternative means of treatment of the oral lichen planus.
Patients affected by oral lichen planus are often subjected to medical treatment for long periods. The drugs of the choice are immunosuppressive agents. Drugs used locally or systemically, cyclosporine, azathioprine and retinoid.
An immunosuppressive agent affects the severity and progression of oral LP but theatrically they could also trigger malignant transformation.[2]
MATERIAL AND METHODS
A pilot study was conducted in the department of Oral and Mxillofacial surgery. The 10 patients were included in the study, they were clinically diagnosed and histipathologically confirmed as patients of oral lichen planus. The extract of turmeric in the ointment form was made at NBRI, used for local application twice/day for a period of 3 months.
The proposal was duly cleared by institute ethics committee. Informed consent was taken from all the patients before study. Patients exclusion criteria included those presenting with systemic disease, drugs consumption, pregnancy.
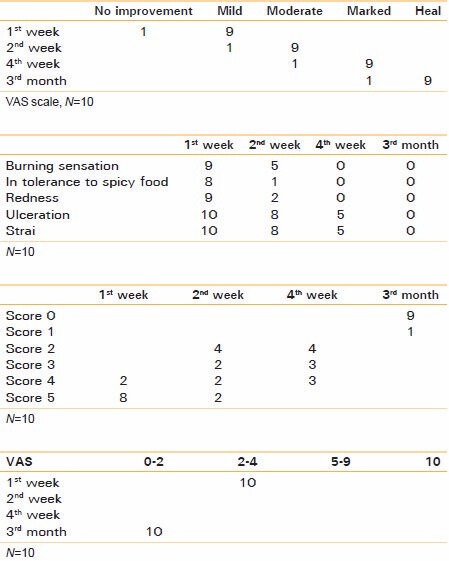
The patients were instructed to report after every 15th day for check up and to collect the ointment. The severity of the clinical sign and symptoms were entered in the set proforma. The data was collected tabulated and analyzed. Significant improvement was observed in the clinical symptoms of the patients. Above all it was well tolerated no adverse reaction was observed.
Response rate was defined based on changes in the appearance score, pain score (VAS) and lesion before and after treatment.
Reduction in sign score thongprasom
Score 5 = white striae with erosive area = 1 cm2
Score 4 = white striae with erosive area < 1 cm2
Score 3 = white striae with erosive area > 1 cm2
Score 2 = white striae with atrophic area < 1 cm2
Score 1 = mild white striae only
Score 0 = no lesion normal mucosa.
PLANT MATERIALS
Fresh rhizome parts of Curcuma longa L. were harvested during flowering in the month of April 2011 from the Banthra- Lucknow).
Extraction
Plant materials were cut and then ground using mill to yield uniform size which was soaked in alcohol (1:10; w/v) for 48 hrs. The extract solution was filtered through filter paper (Whatman No.-1) and alcohol was evaporated using a rotary evaporator at 50°C under reduced pressure to produce crude extract. Crude extracts were kept under low temperature (−4°C) in the refrigerator until use.
Preparation of extract formulation
An appropriate amount of crude extract and glycerin was mixed to prepare extract mixtures in different ratio. And control glycerin
Formulation number MCG (2)-extract: glycerin (75:25).
RESULTS
Improvement in clinical symptoms
DISCUSSION
Steroids have been the drugs of choice in the treatment of lichen planus whether topical or systemic. Their hazards and side effects and contraindications are well known. Non steroidal anti-inflammatory drugs have been also used an alternative to corticosteroid but with less beneficial results in addition to their known side effects [Figures 1–5].[2]
Figure 1.

Pre treatment lesion
Figure 5.

Pre treatment showing lesion
Figure 2.

After 4 week treatment
Figure 3.

After 3 months treatment
Figure 4.

Case 2 after 1 month treatment
Turmeric is the dried rhizome of the perennial herbs Curcuma longa. It is called Haldi in Hindi, turmeric in English, ukon in Japanese. It has been used in Asian Medicine since the second millennium BC. It's utility is referred to in the ancient Hindu script the Ayurveda.
In addition to its aromatic stimulants and coloring properties in the diet, turmeric is mixed with other natural compound such as slaked lime and has been used topically as a treatment for wounds, inflammation and tumour.[3] Curcuma species contains turmerin, essential oil 9turmerons, atlantones are zingiberene and curcuminioids including curcumin 1,7-bis (4_ hydroxy - 3-methoxyphenyl)-16,-heptadiene3-5dion) curcumanoids can be defined as phenolic compound derived from the roots of curcuma species (zingiberaceae) curcumin (deferuloy methane is a low molecular weight polyphenol first chemically characterized in 1910 that is generally regarded as most active constituent and comprises 2-8%of most turmeric preparation. Curcumin is a bis α-β unsaturated β diketone. Its ability to inhibit induction of Cox 2 gene expression has been demonstrated in the colon and oral epithelial cells in vitro. Curcumin also affect carcinogenesis process associated with the growth and dissemination of established malignancy. Angionesis is a now regarded as critical to the transition of premalignant lesion in a hyperproliferative state to malignant phenotype this facilitating tumour growth and metastasis.
Expression of angiogenic growth factors co relates with the prognosis of lung and other cancers. Inhibition of angionesis by growth factor production integral to the formation of veessels, has also been affected by curcumin in nonmalignant and malignant cells. Curcumin also been shown to have immunomodulatory effect involving activation of host macrophages and natural killer cells and modulation of lymphocytes mediated function.
Curcumin has shown growth inhibitory effect in vitro in cancer cells line derived from human prostate, large intestine, brain and leukemia.
Pathogenesis of the OLP should be taken in consideration for the treatment point of view. The Cell mediated immunity to secondary antigenic change in oral mucous membrane is thought to play a major role in its pathogenesis modified keratocyte surface antigens are the primary target for cytotoxic cellular response. Where the most cells and antigen presenting langerhance cells seems to be the key cellular element s in the lesion progress.
The T cells kill the target cell either by synthesis and extracellular release of cytotoxic protein as perforin and granzymes producing pores in the target cells membrane and so kill cells by osmotic lysis or by stimulating the target cell through mechanism that are not well understood to undergo apoptosis after killing the activated T cells disengage from its target but remain active and can kill again .[4]
Curcumin exhibits anti-inflammatory, antiviral antibacterial, antioxidants and nematocidal activities. It has been shown to suppress tumour initiation, promotion and metastasis. It also inhibit the growth and proliferation of head and neck squamous cell carcinoma. By modulating the constitutive activation of NF-Kb signaling arresting the cells in the G1S phase of cell cycle and activation of upstream and down stream caspases .[5]
CONCLUSIONS
OLP is a chronic condition affecting of the Indian population. Steroids have been the drugs of choice in the treatment of lichen planus whether topical or systemic. Their hazards and side effects and contraindications are well known . We tried to find out herbal modalities for oral lichen planus with no or minimal side effects.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- 1.Edwards PC, Kelsch R. Oral lichen planus: Clinical presentation and management. J Can Assoc. 2002;68:494–9. [PubMed] [Google Scholar]
- 2.Lodi G, Scully C, Carrozzo M, Griffiths M, Sugerman PB, Thongprasom K. Current controversies in oral lichen planus: Report of an international consensus meeting. Part 2. Clinical management and malignant transformation. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2005;100:164–78. doi: 10.1016/j.tripleo.2004.06.076. [DOI] [PubMed] [Google Scholar]
- 3.Sharma RA, Gescher AJ, Steward WP. Curcumin: The story so far. Eur J Cancer. 2005;41:1955–68. doi: 10.1016/j.ejca.2005.05.009. [DOI] [PubMed] [Google Scholar]
- 4.Jajarm HH, Falaki F, Mahdavi O. A comparative pilot study of low intensity laser versus topical corticosteroids in the treatment of erosive-atrophic oral lichen planus. Photomed Laser Surg. 2011;29:421–5. doi: 10.1089/pho.2010.2876. [DOI] [PubMed] [Google Scholar]
- 5.Sharma C, Kaur J, Shishodia S, Aggarwal BB, Ralhan R. Curcumin down regulates smokeless tobacco-induced NF-kappaB activation and COX-2 expression in human oral premalignant and cancer cells. Toxicology. 2006;228:1–15. doi: 10.1016/j.tox.2006.07.027. [DOI] [PubMed] [Google Scholar]