

Abstract
Introduction:
This retrospective study is aimed at the documentation of a more complete view of epidemiological data with particular focus on the characteristics of the surgically and non-surgically treated patients with zygomatic complex fractures.
Materials and Methods:
A total of 133 surgically and 150 non-surgically patients were treated with zygomatic complex fractures in VU University medical center Amsterdam from January 2007 to January 2012 were analyzed. These patient groups were further subdivided into displaced or non-displaced fractures and compared with each other according to age, gender and trauma etiology.
Results:
The mean age of all 286 patients was 42.8 years (standard deviation [SD: ±19.8]). Surgically and non-surgically treated patients differed in presentation with a significantly overall higher age of females, especially within the non-surgically treated patient group with displaced fractures (mean age of 59.5 years, SD: ±27.4). The mean ages of males from the different subgroups were more consistent with the overall mean age. The main causes were traffic accidents, whereas the contribution of falls and assaults depended on age group, gender, treatment management and even fracture displacement.
Conclusions:
This report provides us important epidemiological data of all patients with zygomatic complex fractures. The non-surgically treated patient group contained patients of higher age, more females and a fall-related cause, compared to the surgically treated patient group. The surgically treated patient group showed the same epidemiological characteristics as were demonstrated in previous studies.
Keywords: Epidemiology, fractured zygomatic complex, non-surgical, surgical
INTRODUCTION
Fractures of the zygomatic complex are common after facial trauma and are frequently associated with additional traumatic injury.[1,2,3,4] Early diagnosis of zygomatic complex fractures is essential for optimal treatment and is directly dependent on appropriate initial evaluation, correct injury assessment, and timely initiation of the chosen therapy. Surgical intervention is the treatment of choice for dislocated zygomatic complex fractures, unless patients are medically unfit to undergo surgery if patients refuse surgery, or if patients present with none or minimal functional and/or aesthetic problems.[5,6] In the literature, many of the studies can be found concerning the evaluation of the surgical treatment management of the fractured zygomatic complex.[7,8] Literature concerning the pre-operative assessment of zygomatic complex fractures, in particular the epidemiological differences between the surgically and non-surgically indicated treatment groups, is lacking. To the best of our knowledge, only one study by Back et al. specifically investigated the non-surgically treated patients.[9] However, the study by Back et al. included all facial fractures and therefore did not in particular focus on patients with solely zygomatic complex fractures.[9] The purpose of the present retrospective study was to provide physicians a more complete view of the epidemiological characteristics of the surgically and non-surgically treated patients with zygomatic complex fractures.
MATERIALS AND METHODS
Subjects
A retrospective review was performed from all hospital and out-patient records of 283 patients diagnosed with a fractured zygomatic complex, from January 2007 to January 2012. The eligible patients were identified using the hospital database. Data collection consisted of age, gender, fracture site, fracture displacement, cause of the trauma injury (assault, traffic accident, sport accident, fall or other), date of the trauma, date of the first consultation, and treatment management (surgical or non-surgical). Diagnosis (and the presence of fracture displacement) of all patients was established at the same day of initial assessment by plain radiographic analysis (submentovertex and occipitomental radiographs) and/or computed tomography-scan (CT-scan). Exclusion-criteria were the presence of a Le Fort fracture, or other facial bone fractures that were associated with the (four-sided) fractured zygomatic complex (e.g., isolated lateral orbital rim and/or wall, orbital floor or zygomatic arch), and/or a bilaterally fractured zygomatic complex. Furthermore, patients were excluded if the initial clinical assessment was more than 1 week after the trauma and if radiographical analyses (e.g., plain radiographs or CT-scans) were not available. After data retrieval patients were divided into a group in which patients underwent surgical treatment and a non-surgical treatment group. Furthermore, patients in the non-surgical treatment group were subdivided into groups based on displacement of the fractured zygomatic complex (displacement vs. non-displacement).
Statistics
Nominal data were presented as absolute and relative frequencies, metric data as mean and standard deviation (SD). Comparisons between the groups were done by the Chi-square test for nominal data and the Mann-Whitney U-test for age. P < 0.05 were considered to be significant. All calculations were made using Statistical Package for the Social Sciences (IBM) V 19.0.
RESULTS
Patient demographics
As you can see in Table 1, the patient demographics are listed The study population consisted of 283 patients of which 133 surgically treated and 150 non-surgically treated. The mean age of the population was 42.8 (SD: ±19.8) years. Subdivided by gender, 201 male (71%) and 82 female (29%) patients were included. There was a significant (P < 0.05) difference in age between male patients (mean age: 40.6 years, SD: ±17) and female patients (mean age: 48.2 years, SD: ±23.6).
Table 1.
Patient demographics
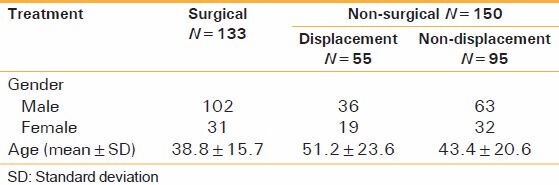
Compared with the surgically treated patients group the patients of the non-surgically treated group were significantly older (P < 0.05). Concerning the non-surgically treated patients group, the 55 patients with a displaced fractured zygomatic complex differed from the 95 patients with a non-displaced zygomatic complex fracture. The mean age of those with displaced zygomatic complex fractures was higher (51.2 years, SD: ±23.6), compared with those with the non-displaced fractures (43.4 years, SD: ±20.6), especially with regard to the female patients (mean age of 59.5 years, SD: ±27.4). The differences were not significant (P = 0.055).
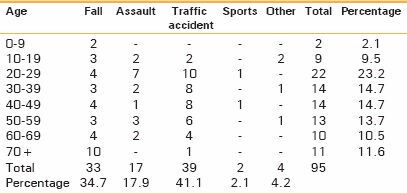
As demonstrated in Table 2, the main cause of zygomatic complex fractures was traffic accidents (43.1%), followed by falls (27.2%) and assaults (20.5%). Sport related accidents and other causes were considered as minor causes.
Table 2.
Cause of injury according to age groups in all patients with a fractured zygomatic complex
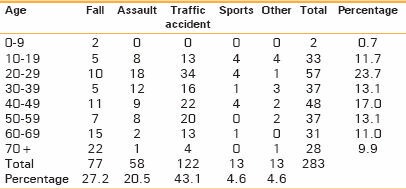
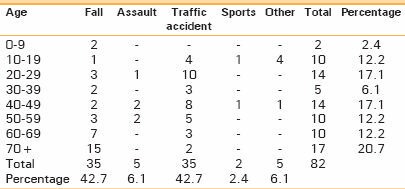
The main causes differed substantially between male and female patients [Tables 2a and b]. In male patients, traffic accidents accounted for 43.3%, followed by assaults (26.4%) and falls (20.9%). In female patients both traffic accidents (42.7%) and falls (42.7%) were the most common causes, whereas assaults were not seen frequently (6.1%). Falls accounted significantly more for the older ages, whereas traffic accidents and assaults accounted for the younger ages (P < 0.000). The male patients were mainly in their 20th year of age, whereas the females were mainly older than 70 years of age.
Table 2a.
Cause of injury according to age for male patients
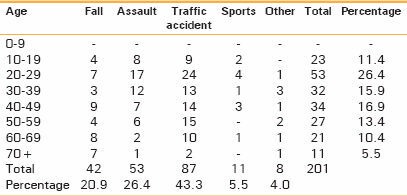
Table 2b.
Cause of injury according to age for female patients
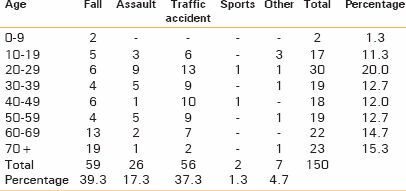
For both groups traffic accidents mainly consisted of bicycle and motorcycle accidents with relative more bicycle accidents for the female patients [Figure 1]. The main cause of injury in the surgically treated patients accounted for almost 50% of traffic accidents, followed by assaults (24.1%) and falls (13.5%) [Table 3a]. In the non-surgically treated patient group falls formed the main cause (39.3%), closely followed by traffic accidents (37.3%). Assault accounted for 17.3% [Table 3b].
Figure 1.
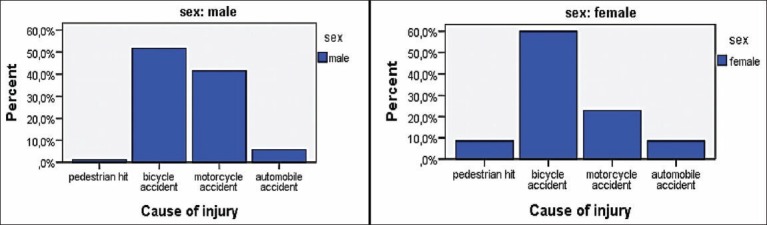
Traffic accidents divided by mode of transport for male and female patients
Table 3a.
Cause of injury for surgically treated patients
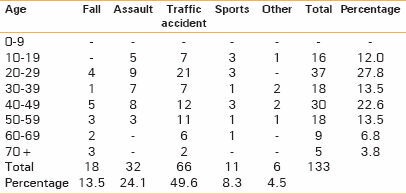
Table 3b.
Cause of injury for non-surgically treated patients
Non-surgically treated patients divided into displaced and non-displaced fractures
The relative share of male patients was almost equally divided between the displaced fracture group (65.5%) and the non-displaced fractures (66.3%). The main causes differed between both groups within the non-surgically treated group. Displaced zygomatic complex fractures were mainly caused by falls [Table 4a], whereas non-displaced fractures were mostly caused by traffic accidents, followed by falls [Table 4b]. Assaults were almost equally divided between both groups.
Table 4a.
Causes of injury for the displaced fractures in the non-surgically treated patients group
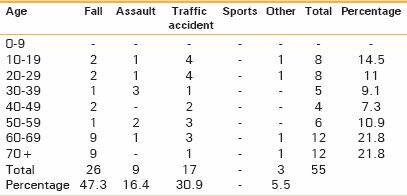
Table 4b.
Causes of injury for the non-displaced fractures in the non-surgically treated patients group
DISCUSSION
This retrospective study aimed at the documentation of a more complete view of epidemiological data, as well as analysis of the differences between the surgically and non-surgically treated patients with zygomatic complex fractures.
The mean age of all 286 patients was 42.8 years (SD: ±19.8). Surgically treated and non-surgically treated patients differed substantially in presentation and, in particular, the females of the non-surgically treated group. As expected, the non-surgically treated patients had a higher mean age (46.2 years, SD: ±22.0), especially within the group of fracture displacement. This latter group almost consisted of symptomatic patients and will mainly consist of patients with treatment refusal or patients that are medically unfit. Strikingly, only female patients of the non-surgically treated patients group and not of the surgically treated patients group were much older (mean age of 52.3 years, SD: ±26.3) and especially for those within the displaced fractures (mean age of 59.5 years, SD: ±27.4). The age of our surgically treated patients group had similar results with other publications, in which predominance of younger patients, aged between 21 and 30 years and, moreover, no large differences in age between male and female patients were reported.[2,3,4] We found an overall higher mean age and this was due to our non-surgically treated patients that consisted of an old aged female population. As in line with other previous studies the sex distribution was markedly higher for males than for females with a ratio of 2.4:1 of all patients.[1,2,3,4]
In our study, the main causes in all patients were mainly attributed to traffic accidents, assaults and falls. In many other studies, traffic accidents and assaults were main causes,[1,2,3,4,10] which was in accordance with our surgically treated population but not with the non-surgically treated population. Fall (40%) was the main cause in the non-surgically treated patients group and in particular in those with displaced zygomatic complex fractures (47%), followed by traffic accidents. This is not in accordance with Back et al., who reported a high incidence of assaults (46%), followed by falls (20%) in their non-surgically treated patients.[9] However, the study of Back et al. included all facial fractures and was conducted in Australia with a lower mean age of 38 years. Our higher incidence of falls is partially due to old aged (above 50 years) female patients who have a higher risk on and are more prone to falls[11] and have other living and/or social habits. Assaults happen much more in young male adults, as in accordance with our surgically treated population. Additional explanation for our higher incidence of falls might be due to our governmental safety measurements that could have decreased traffic (car) accidents[10] and citizen safety (less alcohol abuse, assaults) in our country.
This study was a retrospective analysis, which means that it was automatically subject to measurements and registration styles by physicians and might therefore have a subjective bias. Another shortcoming of our study is, whether our epidemiological data is representative for whole Amsterdam as there are four other hospitals treating patients with trauma injury. However, to our knowledge this is the first report for The Netherlands, which includes the non-surgically treated patients group.
There are several differences between the non-surgically treated and the surgically treated patients, and even within the non-surgically treated patients group, based on the presence of fracture displacement. From an epidemiological point of view neglecting, this non-surgically treated group in studies and solely describing the surgically treated patients can be considered a data gap and may be also an explanation for the large variability of incidence and etiology between different countries.[1,2,4,8,10] Standardized and comparable studies including non-surgically treated patients and more specifically comparing the non-surgical group with the surgical group are therefore highly required.
CONCLUSION
This retrospective analysis provides us important data for a detailed view of all patients with zygomatic complex fractures and shows several epidemiological differences between the surgically and non-surgically treated patient groups and even differences within the latter group. The surgically treated group mainly consisted of young male adults and the assault-related cause highly contributed, as in accordance with previous studies. On the contrary, the non-surgically treated group had a high proportion of elderly female patients, especially for the group with displaced zygomatic complex fractures. Furthermore, there was a high amount of fall-related causes. Epidemiological studies should be based on surgically as well as non-surgically treated patient groups and will help us to provide the importance of the differences between these groups and perhaps future plans for injury prevention.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- 1.Covington DS, Wainwright DJ, Teichgraeber JF, Parks DH. Changing patterns in the epidemiology and treatment of zygoma fractures: 10-year review. J Trauma. 1994;37:243–8. doi: 10.1097/00005373-199408000-00016. [DOI] [PubMed] [Google Scholar]
- 2.Gassner R, Tuli T, Hächl O, Rudisch A, Ulmer H. Cranio-maxillofacial trauma: A 10 year review of 9,543 cases with 21,067 injuries. J Craniomaxillofac Surg. 2003;31:51–61. doi: 10.1016/s1010-5182(02)00168-3. [DOI] [PubMed] [Google Scholar]
- 3.Trivellato PF, Arnez MF, Sverzut CE, Trivellato AE. A retrospective study of zygomatico-orbital complex and/or zygomatic arch fractures over a 71-month period. Dent Traumatol. 2011;27:135–42. doi: 10.1111/j.1600-9657.2010.00971.x. [DOI] [PubMed] [Google Scholar]
- 4.van den Bergh B, Karagozoglu KH, Heymans MW, Forouzanfar T. Aetiology and incidence of maxillofacial trauma in Amsterdam: A retrospective analysis of 579 patients. J Craniomaxillofac Surg. 2012;40:e165–9. doi: 10.1016/j.jcms.2011.08.006. [DOI] [PubMed] [Google Scholar]
- 5.Evans BG, Evans GR. MOC-PSSM CME article: Zygomatic fractures. Plast Reconstr Surg. 2008;121:1–11. doi: 10.1097/01.prs.0000294655.16607.ea. [DOI] [PubMed] [Google Scholar]
- 6.Kelley P, Hopper R, Gruss J. Evaluation and treatment of zygomatic fractures. Plast Reconstr Surg. 2007;120:5S–15. doi: 10.1097/01.prs.0000260720.73370.d7. [DOI] [PubMed] [Google Scholar]
- 7.Carr RM, Mathog RH. Early and delayed repair of orbitozygomatic complex fractures. J Oral Maxillofac Surg. 1997;55:253–8. doi: 10.1016/s0278-2391(97)90537-1. [DOI] [PubMed] [Google Scholar]
- 8.Zingg M, Laedrach K, Chen J, Chowdhury K, Vuillemin T, Sutter F, et al. Classification and treatment of zygomatic fractures: A review of 1,025 cases. J Oral Maxillofac Surg. 1992;50:778–90. doi: 10.1016/0278-2391(92)90266-3. [DOI] [PubMed] [Google Scholar]
- 9.Back CP, McLean NR, Anderson PJ, David DJ. The conservative management of facial fractures: Indications and outcomes. J Plast Reconstr Aesthet Surg. 2007;60:146–51. doi: 10.1016/j.bjps.2006.01.032. [DOI] [PubMed] [Google Scholar]
- 10.van Beek GJ, Merkx CA. Changes in the pattern of fractures of the maxillofacial skeleton. Int J Oral Maxillofac Surg. 1999;28:424–8. doi: 10.1034/j.1399-0020.1999.280605.x. [DOI] [PubMed] [Google Scholar]
- 11.Iida S, Hassfeld S, Reuther T, Schweigert HG, Haag C, Klein J, et al. Maxillofacial fractures resulting from falls. J Craniomaxillofac Surg. 2003;31:278–83. doi: 10.1016/s1010-5182(03)00069-6. [DOI] [PubMed] [Google Scholar]