

Abstract
Introduction:
Burn injuries are a serious public health problem. In our study we have identified different epidemiological factors based on 10 years of our experience at a burn unit in central India and recommend some strategies to prevent burn injuries.
Materials and Methods:
This is a retrospective analysis (2001-2010) of database from burn unit of S.S. Medical College, Rewa, India.
Results:
2499 patients with burn injury were analysed. 66.8% and 38.2% patients were females and males respectively, with a median age of 25 years. Flame (80.1%) was most common cause, home (96%) was most common place, traditional Indian stove (28.8%), kerosene lamp (26.7%), hot liquid (12.2%) and kerosene stove (10.4%) were common causes. Median Total Body Surface Area (TBSA) burn was 40.0%; females had significantly greater (P < 0.001) burn than males (median 50% vs 26.0%). High mortality (40.3%) seen; female sex (OR 3.22, 95% CI 2.65-3.92); young age (15-29 year) (OR 3.48, 95% CI 2.45-4.94); flame burn (OR 12.9, 95% CI 1.69-98.32); suicidal burn OR 6.82 95%CI 4.44-10.48) and TBSA > 76% (OR 3099, 95%CI 1302-7380) were significant risk factors for death. Median hospital stays was 8 days; shorter hospital stays seen among TBSA burn > 76% (2 days), suicidal intent (4 days), and those who expired (4 days). Septicemia (45.8%) and burn shock (41%) were the major cause for death.
Conclusions:
Cooking and lighting equipments are major cause of burn injury among females and young age group. Equipment modification to improve safety features and public awareness programs are necessary to reduce burn incidents.
Keywords: Burns, epidemiology, female, flame, kitchen, mortality, septicemia, suicidal
INTRODUCTION
Incidence of burn injuries are common in India[1] and is the sixth leading cause of accidental death.[2] Youths and females constitute a significant part of the affected population. A large number of patients suffer from severe burns resulting in increased mortality and morbidity. Despite India's recent socioeconomic growth, management of burn patients and their prognosis remains poor due to the lack of trained professionals and specialized burn centers and enormous cost of medical and surgical management, which is not affordable by most patients.[3,4]
The epidemiological factors of burn injuries vary considerably in different communities and region of the world including India. As very few epidemiological studies are reported from India, the present study was designed to identify the various factors responsible for burn injury treated over a decade in our burn treatment unit and to compare its outcome with various other studies from India and other countries. Further, an effort was made to recommend various preventive measures at the community level to decrease the incident of burn injury.
MATERIALS AND METHODS
This is a retrospective study of burn patients admitted from 1st January 2001 to 31st December 2010 in our hospital. Data was obtained from the medical record section, regarding, (i) Registration: age, sex, residence, occupation, marital status, socioeconomic status, (ii) Chronological: dates of admission and discharge, (iii) Circumstantial: place, intent, cause and source of heat, (iv) Clinical assessment: by using Wallace's “Rule of Nine” in adult and “Lund and Browder” chart in the pediatric age groups and (v) Cause of death: The interrelationships between clinical and epidemiological variables with burn injury were studied. Statistical analyses were performed using the SPSS (Version 16.1) software and following tests were applied: Binominal test, MannWhitney U test, KruskalWallis test, Pearson's Chisquared test (χ2) and P value.
RESULTS
Seasonal variation
Most burn cases were observed in summer (35.5%) and winter (23.9%) with the lowest incidence in the rainy season (19%) [Graph 1].
Graph 1.
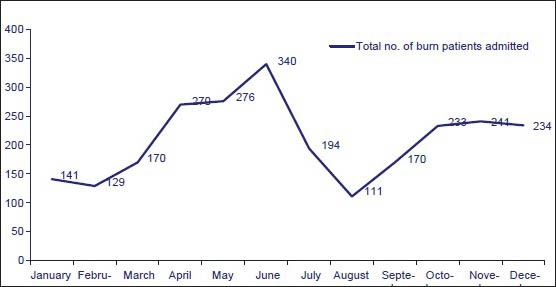
Incidents of burns according to month
Age and sex
Out of total 2,499 burn patients, 1670 (66.8%) are females and 829 (38.2%) are males. Above 6 years of age, significantly (P < 0.001) more females than males reported burn injuries. The median age of patients suffering burn injuries was 25 (mean 26) years, indicating incidence being predominant in young population [Graph 2].
Graph 2.
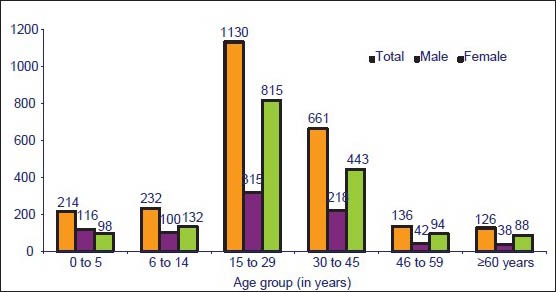
Burns according to age and sex
Residence and place of incident
Most (71.3%) burn patients were from rural areas. Most burns were of domestic origin (96.0%) and kitchen (54.8%) was the most common place of injuries, followed by the living room (41.2%) with very few burn injuries encountered outdoors (4.0%). Females most commonly encountered burn injuries in kitchen (M:F = 1: 2.2) and living room (M:F = 1:1.9) while males predominantly suffered from burn injuries outdoors (M:F =1:0.7).
Cause of burn and equipment
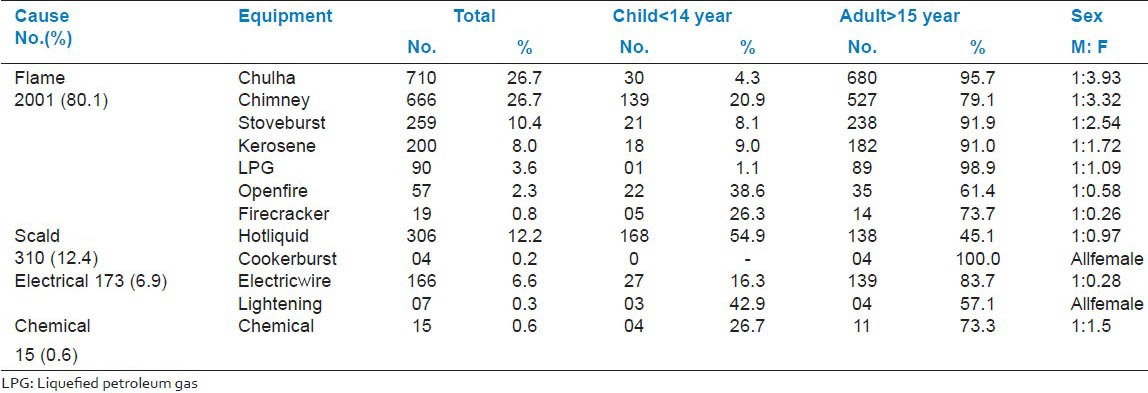
Flame (80.1%) was the most common cause of burn, followed by scald (12.4%), electrical (6.9%) and few cases of chemical burn (0.6%) [Graph 3]. Equipments responsible for flame burns were: floor level cooking arrangements using wood as fuel in Chulha (traditional Indian stove) (28.8%), homemade kerosene bottle lamp chimney (26.7%) and pressurized kerosene stove (10.4%). Scalds (12.4%) were due to contact with hot liquids such as milk, water, oil, vegetable, etc., [Table 1].
Graph 3.
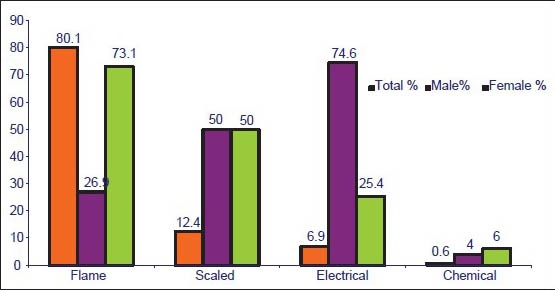
Cause of burn and sex
Table 1.
Causes of burn and equipments responsible
Intent of burn
Accident (93.3%) was the most common intent, followed by suicide (5.8%) and homicide (0.9%). Although females were the majority among all intents, the data did not reach statistical significant (Z = 0.664, 2df, P = 0.718).
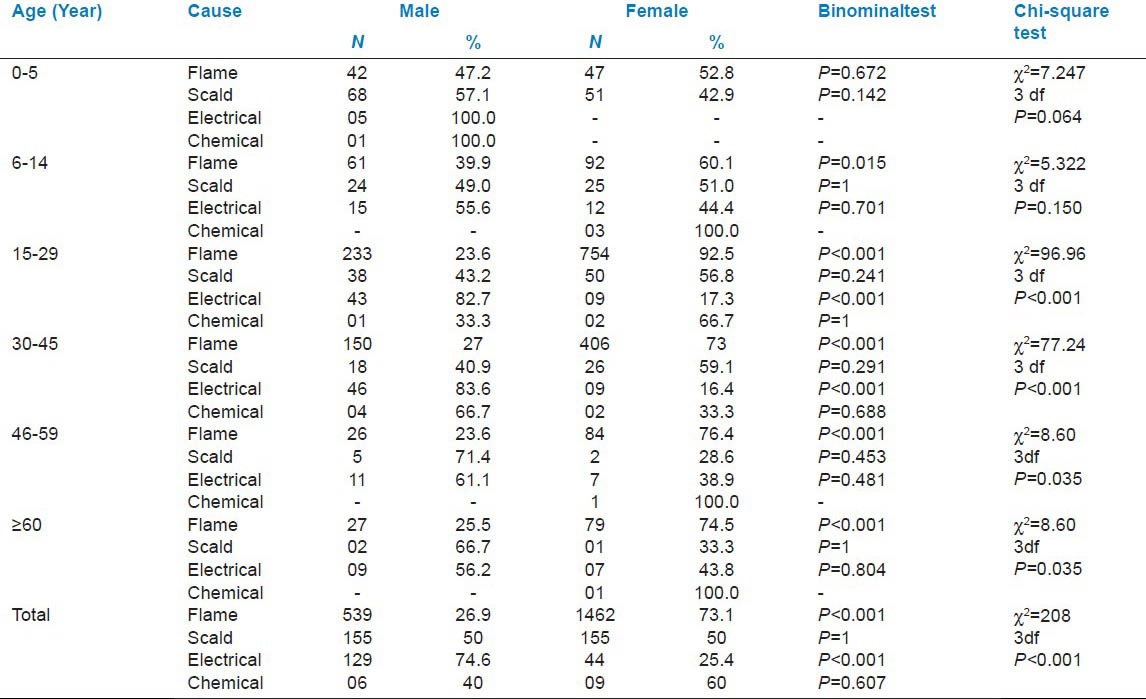
Cause of burn according to age and sex
Amongst children aged 05 years, scalds (55.6%) were most common with no significant sex differences (P = 0.064). Contrary to this, flame injuries were most common (P < 0.001) among the age group over 15 years. Among adults significantly (P < 0.001) more females than males patients suffered flame burn, only electrical burns were significantly more common among males (P < 0.001) [Table 2].
Table 2.
Cause of burn and age
Clinical assessment of the burn wound
In our study, total body surface area (TBSA) burn ranged from 1% to 100% (median 40%, mean 47.5%). 1319 (52.7%) patients had < 40% TBSA burn while 1180 (47.3%) patients had > 41% TBSA burn. Significantly (Z = 250.6, 9df, P < 0.001) more female cases than males were observed with TBSA > 10% [Graph 4].
Graph 4.
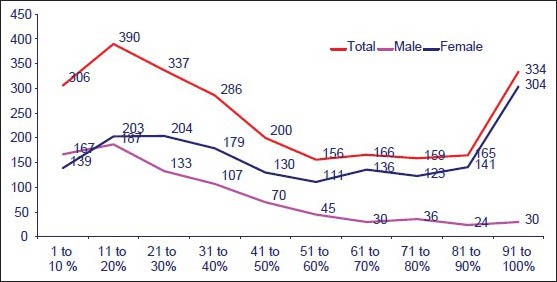
Total body surface area (TBSA) burn and sex
Distribution of burn patients based on TBSA
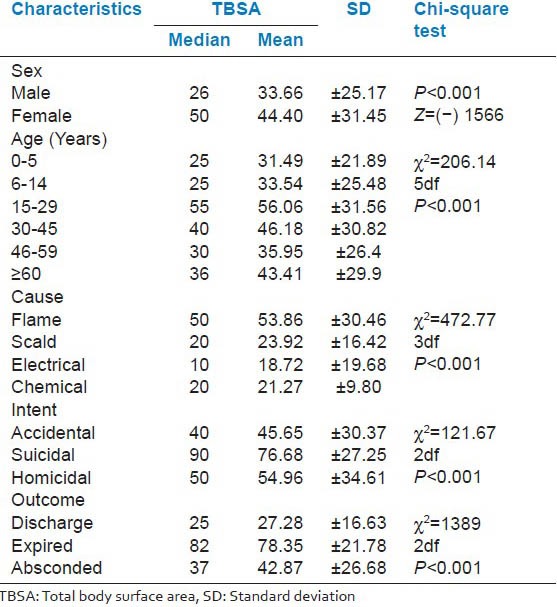
Significant statistical differences in median TBSA burn between different characteristics were observed. Females (median 50%, SD ± 31.45); age 1529 year (median 55%, SD ± 31.56); flame burn (median 50%, SD ± 30.46%), suicidal intent (median 90%, SD ± 27.25%) and among who succumbed to burn injury (median 82%, SD ± 21.78%) had severe burn injury [Table 3].
Table 3.
Burn characteristics according to TBSA
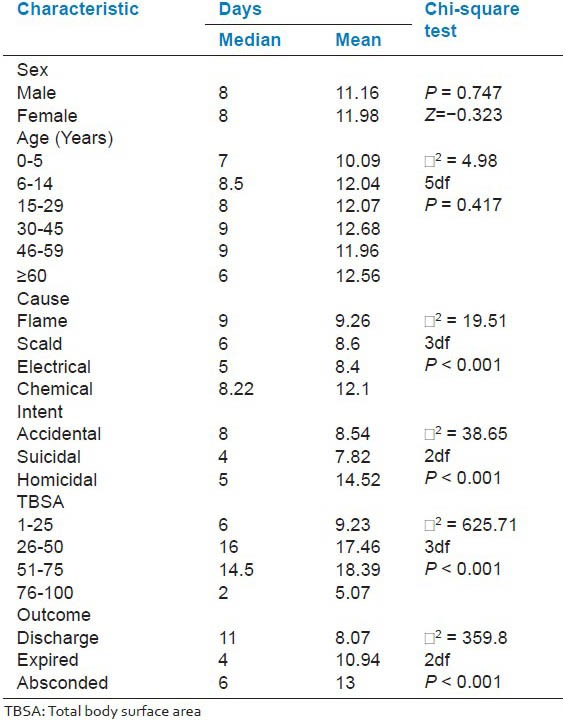
Hospital stays
Hospital stay ranged from few hours to 182 days (median 8 days). Significantly, shorter (P < 0.001) hospital stay was observed among TBSA burn > 76% (2 days), suicidal intent (4 days) and those who succumbed to burn injury (4 days). Longer hospital stay was observed among TBSA burn 2650% (16 days), but no significant difference in median hospital stay was observed between male and female patients (P = 0.747) [Table 4].
Table 4.
Burn characteristics according to hospital stay (days)
Mortality
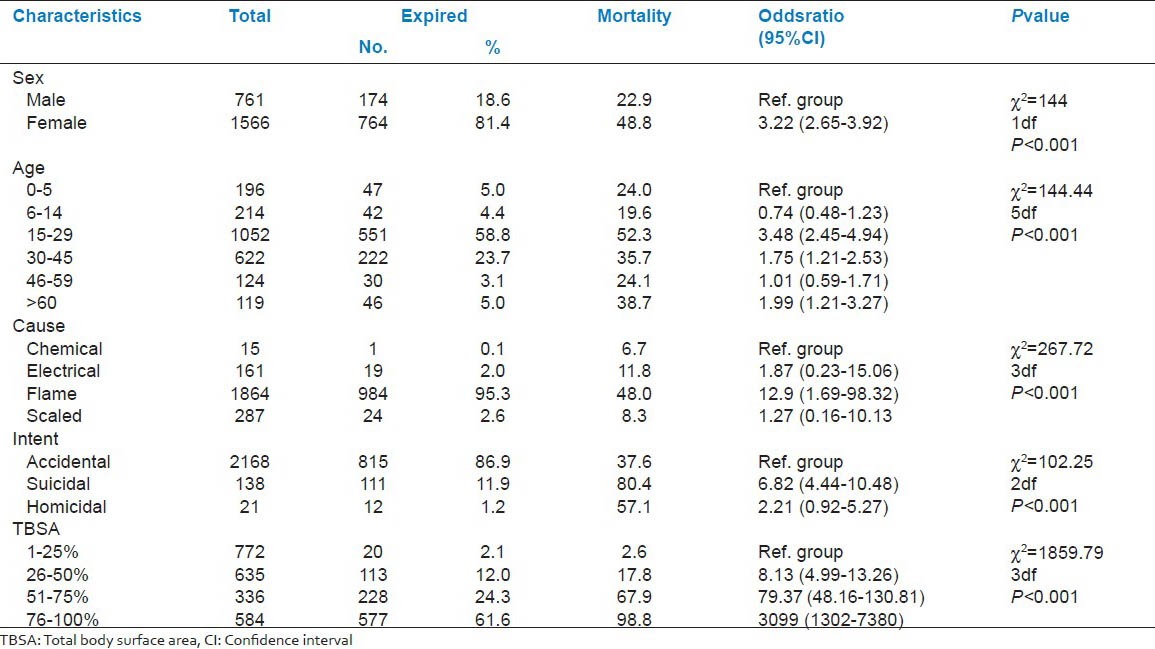
Females had significantly higher (48.8% vs. 22.9%, P < 0.005) mortality than males and they are also more likely succumbed to burn injury than males (odds ratio [OR] 3.22, 95% confidence interval [CI] 2.65-3.92). 15-29yearold patients had highest mortality (52.3%) and were more likely to succumb to burn injury (OR 3.48, 95% CI 2.45-4.94). Suicidal burn cases had the highest mortality (80.4%) and most often resulted in patient death (OR 6.82, 95% CI 4.44-10.48). Flame burn had highest mortality (48.0%) and was most likely to result in death (OR 12.9, 95% CI 1.69-98.32). Increase in TBSA significantly (Z = 1859.79, 3df, P < 0.001) increased mortality; thus, highest mortality (98.8%) was observed in patients with 76-100% TBSA burn [Table 5]. Septicemia was most common cause of death (45.8%), followed by burn shock (41.0%), pneumonia (11.8%) and other factors (1.4%).
Table 5.
Burn mortality (n=2327)
DISCUSSION
Seasonal variance in burn injuries are previously reported from Western (Ahmedabad)[5] and Central India (Nagpur).[6] Very high temperature and low humidity during the summer in these regions are responsible for burn injuries. However, in winter, people in rural regions use “open wood fire” and “Gorsy” (burning coal on an earthen container) as a source of heat, which also increase the incidence of accidental burns. The incidence is also considerable in the month of November, attributed to firecracker accidents during customary celebration of “Diwali” (the festival of lights).
In our study, large number burns were due to the domestic activities (96%) and the majority of the incidences occurred in kitchen (54.8%). It is essential to note that in rural Rewa region people don’t have a separate kitchen area and rather cook inside or beside their living room/cottage. Most of the studies from India[7,8] and other low income countries such as Egypt,[9] Pakistan[10] also report similar trend. Flame (80.1%) was most common cause of burn, which is consistent with other studies reported in India[5,6,7,8] and other developing countries,[9 11] ] although equipments responsible vary widely.
Earthen Chulha in the present study was the most common (28.8%) equipment responsible for burn accidents. Rural Indian housewives cook food on this traditional floor level earthen using charcoal/wood as fuel, which is very dangerous and lack fire safety features. This has increased susceptibility to burn injuries among rural Indian housewives and children playing around her. Hence, it is essential to make the cooking space safe by separating it from the living room and adopting necessary safety precautions while cooking. Government projects providing brick made house for rural people must be enforced to create fire safe cooking environment to reduce the incidence of burn injuries.
Chimney (26.7%) was the second most common source of accident identified in our study and is consistent with many other reports from India[6,8] and Sri Lanka.[11] Chimney is indigenously made and is used as a source of light in rural areas. A hole is made over the cap of a glass bottle or tin jar and a piece of cloth is passed through this hole and dipped in bottle/jar containing kerosene. This bottle lamp is very unstable because of its shape, where center of gravity remains at a higher level and easily tilts down. When this chimney falls down, kerosene and fire spreads all over and burn accidents occurs. Product modification for this kerosene lamp is needed; a conical shaped lamp with a wide base may give better gravitational stability so that it will not tilt/fall down easily. Kerosene lamp related accidents could be reduced more effectively by providing an alternate source of light. Hence, electrification or installing solar system in all villages and providing lighting from 5 pm to 10 pm will certainly decrease the use of chimney and hence the incidence of burns.
Kerosene pressure stoves was the third common (10.4%) cause of burn injury in our study and it is the most common source of accident in the urban India[6,12,13] and SubSaharan countries,[9] where kerosene is easily available and affordable. The mechanism of stove injury is very unique, sometimes the burner hole is choked by carbon deposits or by any particulate impurities in kerosene; when the whole is pinned for cleaning, a large volume of aerosol comes jets out under high pressure as a fire ball and accidents occurs. A land mark study by Ahuja and Bhattacharya[12] from Delhi showed that banning of kerosene pressure stove decreased burn admission by 25%. Consequently, Delhi has become the first kerosene free city in India.[14] However, without providing an alternative, banning of kerosene stoves all over India may not be practical, because kerosene is affordable and stoves are very handy to use. Hence, promotion of nonpressurized kerosene stove are recommended along with strictly regulating the quality of pressure stoves, purity of kerosene and providing community based training for correct and safe use of kerosene stoves. Scalds were responsible for 12.4% of total burn accidents and children (54.19%) were the most commonly affected. Similar incidence of scalds among children are also reported from both high[15] and low income countries.[16,17]
Gender wise distribution of burn patients greatly differ in high and low income countries. With male predominance in highincome countries such as Norway[18] and Australia[19] and female predominance in the middle and low income countries such as Egypt,[9] Pakistan,[10] Sri Lanka[11] and India.[12,20] Such gender differences observed are multi factorial and related to varying sociocultural behaviors. People of all ages are susceptible to burn, although the household circumstances, work place and physical activity may increase or decrease the susceptibility rate. Mean age of burn injuries in our study was 25 years (median 26 years), which is comparable to reports from developed countries[18,19] and other studies from India.[5,6,8] Children are also at a higher risk of burn injuries, both in highincome and low/middleincome countries.[9,10,18,19] We found a significant number (17.9%) of patients in the pediatric age group (0-14 years). Similar pattern (20.28%) of pediatric burns are also reported by Ganesamoni et al.[13] in south India. Among the pediatric burn patients, a considerable proportion (8.6%) of children was found to be young (0-5 year). This is because preschool children crawl into danger areas accidentally.
The median TBSA burn in our study was 40%. Most importantly, 47.3% cases had > 40% TBSA burn. Such higher TBSA burns are also reported in many Indian studies.[3,4,5,12] However, in highincome countries[18,21] mean TBSA was 11.5-19.5% and only 4-8.2% cases had 30% or more TBSA burn. Significantly, (Z = 250.6, 9df, P < 0.001) more females than male cases had TBSA exceeding 10% in our study and above 70% TBSA burn, 86.3% cases were females. Hence in addition to traditional causes, we should also focus on the intent, which may bring some light into this gender difference. Indeed burn injuries may be intentional or nonintentional, but sometimes it is very difficult to determine it. Memchoubi and Nabachandra.[22] has reported a high rate of suicidal (24.61%) and homicidal (29.23%) burn in autopsy cases. Other studies from India[6,13,23,24] have also reported a high rate of homicidal and suicidal burns among females. However, in our study, no significant association between female sexes with homicidal/suicidal burn was observed, this may be probably due to under reporting of the exact intent by the attendants to avoid litigation.
Severity of burns determines hospital stay. Our data is consistent with the previous report by Attia et al.[9] who reported mean hospital stay of 21.5 and 5.3 days by surviving and patients succumbing to burn injuries respectively. Comparing and interpreting burn mortality data's are very difficult, because, study population, management protocol and statistical analysis differ widely among different studies. High mortality (40.3%) was observed in our study and is consistent with other studies from India and other low income countries.[9,12,13,16,20] In contrast to these results, very low mortality is reported from highincome countries, for example, in Norway[18] only 4% mortality was reported in a 20 year study with median 15% TBSA burn. A study from Israel[25] also reported low (4.4%) mortality rate, but amongst severe burns (TBSA > 90%) mortality was 96.6%, which is consistent with our study (98.8% mortality rate in TBSA > 76%). These data are also consistent with Dastgiri et al.[26] where higher risk of death was observed with higher TBSA > 75%. Indeed every 1% increase in TBSA is significantly associated with 6% increase in risk of death.[27] Hence, we can conclude that among severe burns mortality is comparable between low and highincome countries and management of severe burn is challenging in all set up. Age and gender are also a very important independent factor to predict mortality,[28] young age (15-29 year) and females[29,30] being the most vulnerable group, which is consistent with observations in our study. Septicemia was identified the most common cause of death (45.8%) in our study, followed by burn shock (41.0%). Our results are consistent with other reports.[4,22,24] Severely, burnt patients suffer from burn shock and delay in resuscitation increases mortality.[12] The pitfall of conservative management is delayed wound excision because the burnt tissue serves good media for bacterial colonization, which is subsequently followed by bacteremia and septicemia. Thus, significant numbers of patients succumb due to septicemia in our country. This treatment protocol needs to be improved.
CONCLUSION
Causes of burn in the Rewa region of central India are very “primitive” in nature and are related to cooking (Chulha) and lightening (Chimney) equipments, which are very basic needs of life. Hence, to decrease burn accidents, local administrations must enforce Government housing programs optimally and lighting through conventional and unconventional ways should be provided to all houses. As young people are most affected, educating through community interaction programs to emphasize on safe cooking practices, fire safety precautions, firstaid training must be implemented. Finally, home violence on females in India is a shameful reality; just drafting strict laws will not decrease this crime; education seems to be the answer to this sociocultural problem.
To conclude, in our study we have tried to describe the epidemiology of burn injury and proposed some primary prevention strategies for prevention of burn injuries. Nevertheless, further research and resources are required for secondary and tertiary prevention of burn injuries.
ACKNOWLEDGMENTS
We acknowledge Prof. Dr. G. P. Shrivastava, (M.S., Fellow, Interplast Australia), Professor and Head, Department of Surgery, S.S. Medical College, Rewa, (M.P.) India, for his constant encouragement, guidance and supervision throughout this project. We also thank Dr. Deepak Shukla, M.Sc., Ph.D., for his assistance in statistical analysis and to Dr. Udhav Agrawal, M.Sc., Ph.D., for his excellent computer works and technical assistance.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Sawhney CP, Ahuja RB, Goel A. Burns in India: epidemiology and problems in management. Indian J Burns. 1993;1:1. [Google Scholar]
- 2.New Delhi, India: 2011. National Crimes Record Bureau; Ministry of Home Aff airs, Government of India. Accidental Deaths and Suicides in India 2011. [Google Scholar]
- 3.Shanmugakrishnan RR, Narayanan V, Thirumalaikolundusubrama nian P. Epidemiology of burns in a teaching Hospital in south India. Indian J Plast Surg. 2008;41:347. doi: 10.4103/0970-0358.41108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Akther JM, Nerker NE, Reddy PS, Khan MI, Chauhan MK, Shahapurkar VV. Epidemiology of burned patients admitted in burn unit of a rural tertiary teaching Hospital. Pravara Med Rev. 2010;5:11–7. [Google Scholar]
- 5.Kumar P, Chaddha A. Epidemiological study of burn cases and their mortality experiences amongst adults from a tertiary level care centre. Indian J Community Med. 1997;4:160–7. [Google Scholar]
- 6.Naralwar UW, Meshram FA. Epidemiological determinants of burns and its outcome in Nagpur. Milestone J DMER. 2004;3:19–23. [Google Scholar]
- 7.Jayaraman V, Ramakrishnan KM, Davies MR. Burns in Madras, India: An analysis of 1368 patients in 1 year. Burns. 1993;19:339–44. doi: 10.1016/0305-4179(93)90124-q. [DOI] [PubMed] [Google Scholar]
- 8.Shankar G, Naik VA, Powar R. Epidemiolgical study of burn injuries admitted in two Hospitals of north Karnataka. Indian J Community Med. 2010;35:509–12. doi: 10.4103/0970-0218.74363. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Attia RA, Sherif AA, Mandil AM, Massoud N, Mervat W, Abou-Nazel, et al. Epidemiological and sociocultural study of burn patients in Alexandria, Egypt. East Mediterr Health J. 1997;3:452–61. [Google Scholar]
- 10.Muqim R, Zareen M, Dilbag, Hayat M, Khan MI. Epidemiology and outcome of burns at Khyber teaching Hospital Peshawar. Pak J Med Sci. 2007;23:420–4. [Google Scholar]
- 11.Laloë V. Epidemiology and mortality of burns in a general Hospital of Eastern Sri Lanka. Burns. 2002;28:778–81. doi: 10.1016/s0305-4179(02)00202-4. [DOI] [PubMed] [Google Scholar]
- 12.Ahuja RB, Bhattacharya S. An analysis of 11,196 burn admissions and evaluation of conservative management techniques. Burns. 2002;28:555–61. doi: 10.1016/s0305-4179(02)00069-4. [DOI] [PubMed] [Google Scholar]
- 13.Ganesamoni S, Kate V, Sadasivan J. Epidemiology of hospitalized burn patients in a tertiary care Hospital in South India. Burns. 2010;36:422–9. doi: 10.1016/j.burns.2009.06.212. [DOI] [PubMed] [Google Scholar]
- 14.New Delhi: The Indian Express; 2012. [Updated on 2012 Aug 22; Cited on 2013 Mar 29]. To make Delhi kerosene-free, 3.5 lakh families to get free LPG cylinders, stoves. Available from: http://www.indianexpress.com/news/ http://www.indianexpress.com/news/to-make-delhi-kerosenefree-3.5-lakhfamilies-to-get-free-lpg-cylinders-stoves/991362 . [Google Scholar]
- 15.Rawlins JM, Khan AA, Shenton AF, Sharpe DT. Epidemiology and outcome analysis of 208 children with burns attending an emergency department. Pediatr Emerg Care. 2007;23:289–93. doi: 10.1097/01.pec.0000248698.42175.2b. [DOI] [PubMed] [Google Scholar]
- 16.Groohi B, Alaghehbandan R, Lari AR. Analysis of 1089 burn patients in province of Kurdistan, Iran. Burns. 2002;28:569–74. doi: 10.1016/s0305-4179(02)00099-2. [DOI] [PubMed] [Google Scholar]
- 17.Light TD, Latenser BA, Heinle JA, Stolpen MS, Quinn KA, Ravindran V, et al. Demographics of pediatric burns in Vellore, India. J Burn Care Res. 2009;30:50–4. doi: 10.1097/BCR.0b013e318191fc91. [DOI] [PubMed] [Google Scholar]
- 18.Onarheim H, Guttormsen AB, Eriksen E. Burn treated at the Haukeland University Hospital Burn Centre – 20 years of experience. Tidsskr Nor Laegeforen. 2008;128:1168–71. [PubMed] [Google Scholar]
- 19.Pegg SP. Burn epidemiology in the Brisbane and Queensland area. Burns. 2005;31(Suppl 1):S27–31. doi: 10.1016/j.burns.2004.10.004. [DOI] [PubMed] [Google Scholar]
- 20.Subrahmanyam M, Joshi AV. Analysis of burn injuries treated during a one year period at a district Hospital in India. Ann Burns Fire Disasters. 2003;16:74–6. [Google Scholar]
- 21.Song C, Chua A. Epidemiology of burn injuries in Singapore from 1997 to 2003. Burns. 2005;31(Suppl 1):S18–26. doi: 10.1016/j.burns.2004.10.005. [DOI] [PubMed] [Google Scholar]
- 22.Memchoubi PH, Nabachandra H. A study of burn deaths in Imphal. J Indian Acad Forensic Med. 2007;29:0971–3. [Google Scholar]
- 23.Chakraborty S, Bisoi S, Chattopadhyay D, Mishra R, Bhattacharya N, Biswas B. A study on demographic and clinical profile of burn patients in an Apex Institute of West Bengal. Indian J Public Health. 2010;54:27–9. doi: 10.4103/0019-557X.70545. [DOI] [PubMed] [Google Scholar]
- 24.Jaiswal AK, Aggarwal H, Solanki P, Lubana PS, Mathur RK. Epidemiological and socio-cultural study of burn patients in M.Y. Hospital, Indore, India. Indian J Plast Surg. 2007;40:158–63. [Google Scholar]
- 25.Haik J, Liran A, Tessone A, Givon A, Orenstein A, Peleg K, et al. Burns in Israel: Demographic, etiologic and clinical trends, 1997-2003. Isr Med Assoc J. 2007;9:659–62. [PubMed] [Google Scholar]
- 26.Dastgiri S, Kalankesh LR, Pourafkary N, Vahidi RG, Mahmoodzadeh F. Incidence, survival pattern and prognosis of self-immolation: A case study in Iran. J Public Health. 2006;14:2–6. [Google Scholar]
- 27.Meshulam-Derazon S, Nachumovsky S, Ad-El D, Sulkes J, Hauben DJ. Prediction of morbidity and mortality on admission to a burn unit. Plast Reconstr Surg. 2006;118:116–20. doi: 10.1097/01.prs.0000221111.89812.ad. [DOI] [PubMed] [Google Scholar]
- 28.Suzuki M, Aikawa N, Kobayashi K, Higuchi R. Prognostic implications of inhalation injury in burn patients in Tokyo. Burns. 2005;31:331–6. doi: 10.1016/j.burns.2004.10.016. [DOI] [PubMed] [Google Scholar]
- 29.Kerby JD, McGwin G, Jr, George RL, Cross JA, Chaudry IH, Rue LW., 3rd Sex differences in mortality after burn injury: Results of analysis of the national burn repository of the American burn association. J Burn Care Res. 2006;27:452–6. doi: 10.1097/01.BCR.0000225957.01854.EE. [DOI] [PubMed] [Google Scholar]
- 30.George RL, McGwin G, Jr, Schwacha MG, Metzger J, Cross JM, Chaudry IH, et al. The association between sex and mortality among burn patients as modified by age. J Burn Care Rehabil. 2005;26:416–21. doi: 10.1097/01.bcr.0000176888.44949.87. [DOI] [PubMed] [Google Scholar]