

Abstract
This study is to report the rare localization of a radicular groove on the palatal aspect of the maxillary lateral incisor and to discuss the pathology and management of the concomitant endo-periodontal defect. Unilateral palato-radicular groove was located on the Maxillary right lateral incisor of an 18-year-old female patient. The groove was associated with deep local periodontal pocket resulting in pulp necrosis and the formation of a large periapical lesion. A collaborative management was carried out using a combination of endodontic therapy, surgical enucleation, odontoplasty, and periodontal regenerative procedure resulting the successful healing of the periapical lesion.
Keywords: Palatogingival groove, periodontal-endodontic lesion, periodontal regeneration
INTRODUCTION
The palatal groove is defined as “a developmental groove in root, that when present is usually found on the palatal aspect of the maxillary incisor teeth.” Palato-radicular groove is a rare developmental anomaly with prevalence rate of 2.8-8.5%, mostly present on the lingual surface of the maxillary lateral incisor. These grooves typically begin in the central fossa area of the incisors, extend over the cingulum and continue apically down the root surface.[1]
The exact etiology of this defect is not fully understood. Some clinicians believe that the radicular groove represents the mildest form of dens invaginatus and therefore, the pathogenic mechanism is relatively common. This means that there is minimal infolding of the enamel organ and epithelial sheath of Heartwig during odontogenesis.[2]
Deep radicular groove can pre-dispose to pulp necrosis and establishment of combined periodontal and endodontic lesions. The inherent difficulties in treating the palatogingival groove make its diagnostic complex for practitioners. This can result in ineffective Endodontic treatment attempts, because the lesion can be exclusively periodontal, or if not, as in combined case, the treatment can be of little use without the removal of the local pre-disposing factor and treatment of the resulting periodontal pathosis.[3]
Considering, the great clinical importance of the palato-radicular groove and rare occurrence, the purpose of this paper is to report a case of deep palato-radicular groove on a maxillary lateral incisor with associated periodontal and pulpal involvement. A multidisciplinary treatment approach was carried out, which resulted in periodontal healing and resolution of periradicular radiolucency.
CASE REPORT
An 18-year-old female patient reported to the Department of Conservative Dentistry and Endodontics with a chief complaint of intermittent pain and discharge in the upper front tooth region since 6 months. No history of trauma was given. The patient medical and family histories were non-contributory, and the results of the extra oral examination were unremarkable.
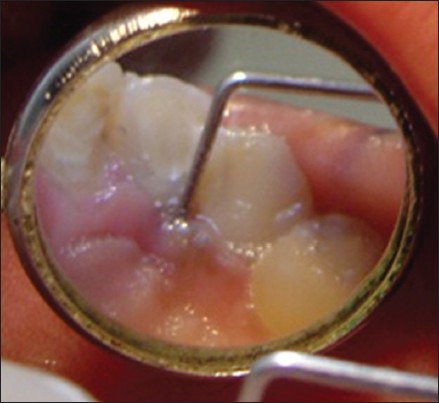
Intraoral examination revealed, discolored right lateral incisor with presence of grade I mobility. Examination on palatal aspect revealed a localized pocket of 8 mm depth with pus discharge from the pocket. On careful examination, a deep palatogingival groove was observed, which was extending deep into the apical region [Figure 1].
Figure 1.

Revealing palatogingival groove on lateral incisor
The tooth did not respond to vitality testing using Electronic Pulp Tester (Parkell Electronics Division, New York, USA). Radiographic examination revealed a well-defined radiolucency in relation to right lateral incisor extending until the apical region of the right central incisor [Figure 2].
Figure 2.

Pre-operative radiograph
Diagnosis
Based on the history, clinical and radiographic examination the lesion was provisionally diagnosed as pulp necrosis, suppurative periradicular periodontitis and moderate localized periodontitis secondary to the palatoradicular groove.
TREATMENT
A collaborative management was planned using a combination of endodontic therapy, odontoplasty, and periodontal regenerative procedure.
Root canal treatment was initiated on right lateral and central incisors since the lesion was extending to the apical region of the right central incisor. Access cavity was prepared after rubber dam application and necrotic debris was removed. There was pus discharge from the canal. Working length was determined by radiographic as well as electronic methods (Root ZX™ J. Morita Co., Kyoto, Japan). Chemo-mechanical preparation was performed using step-back technique. Ca(OH)2 dressing was given for a week. In the following visit after removing Ca(OH)2, master cone was selected and obturation was completed by Gutta-percha and AH-26 sealer (Dentsply Maillefer, Bellaigues, Switzerland) using cold lateral condensation technique [Figure 3].
Figure 3.

Post-obturation
Surgical procedure
The surgical area was made aseptic and local anesthesia was administered. Since, the discharge and the bony defect was on the palatal side, sulcular incisions were placed on palatal side [Figure 4] and a full thickness mucoperiosteal flap was raised on palatal aspect to access the palatogingival groove.
Figure 4.

Flap reflected
On reflection, a distinct groove was visible extending until the apical third. Apical curettage and root planning was carried out [Figure 5] and the groove was restored with glass-ionomer cement [Figure 6] (Fuji II; GC Corporation, Tokyo, Japan). A resorbable membrane (Guided tissue regeneration) was placed to guide the periodontal ligament cells for regeneration.
Figure 5.

Curettage done
Figure 6.

Groove preparation and restoration
The flap was repositioned and stabilized with sutures [Figure 7]. Patient was put under medication and sutures were removed after a week.
Figure 7.

Sutures placed
Patient was recalled at an interval of 1, 3 [Figure 8] and 6 [Figure 9] months for the follow-up.
Figure 8.

Three months follow-up
Figure 9.

Six months follow-up
Six month follow-up revealed absence of signs and symptoms and periodontal pocket [Figure 10]. Radiograph also showed bony healing.
Figure 10.
Reduced pocket depth
DISCUSSION
Historic perspective: Oehlers in 1958 for the first time described such condition as radicular invagination in an upper lateral incisor in a Chinese female. The term palatogingival groove was coined by Lee, Lee and Poon in 1968.[4]
Lee et al. speculated that the palatal groove represents an in folding of the enamel organ and Hertwig's epithelial root sheath and parallels the pathogenesis of dens invaginatus.[4]
Palatoradicular groove could manifest either as:
Periodontal disease
A true endodontic disease
It may appear as a combined endodontic – Periodontal problem.
For anatomical reasons, the radicular groove is an ideal plaque trap for promoting periodontal break-down and pulp necrosis. Reason for the occurrence of combined lesions is existence of communication between the pulp chamber and the periodontium. Friedman and Goultschin have suggested that pulpal necrosis followed by apical periodontitis is often the earliest manifestation of palato radicular groove.[5,6]
Treatment Modalities proposed: Kerezoudis et al.
Surgical removal of granulation tissue and irritants
Gingivectomy and apically positioned flap
Surgical exposure and flattening of the groove by grinding, with or without application of guided tissue regeneration techniques
Placing amalgam restoration in the groove
Orthodontic extrusion of the tooth.
The prognosis of a tooth with a palatal groove depends mainly on location of the groove, severity of the periodontal problem, accessibility of the defect and the type of groove (shallow or deep, short or long).[7,8,9]
To enhance periodontal attachment on the denuded root dentine, Guided tissue regeneration technique was used to regenerate the lost periodontal structures through differential tissue development. Techniques used are classified as: Barriers and Enamel matrix derived proteins.[7] In this case, a bioresorbable collagen based barrier was used, which showed satisfactory result by reducing the pocket depth to 2-3 mm. The rate of healing of the surgical site was good and the radiographic bone regeneration was rapid and impressive without any signs of external root resorption.
CONCLUSION
This case report presented the successful treatment of a pulpal-periodontal combined lesion on a maxillary lateral incisor associated with a palato radicular groove. The key to achieving long-term favorable results in this particular type of developmental anomaly is accurate diagnosis and elimination of inflammatory irritants and contributory factors. Clinician's awareness of existence of such a peculiarity may help to avoid misdiagnosis and improper treatment of these patients.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Schwartz SA, Koch MA, Deas DE, Powell CA. Combined endodontic-periodontic treatment of a palatal groove: A case report. J Endod. 2006;32:573–8. doi: 10.1016/j.joen.2005.08.003. [DOI] [PubMed] [Google Scholar]
- 2.Simon JH, Dogan H, Ceresa LM, Silver GK. The radicular groove: Its potential clinical significance. J Endod. 2000;26:295–8. doi: 10.1097/00004770-200005000-00012. [DOI] [PubMed] [Google Scholar]
- 3.Lara VS, Consolaro A, Bruce RS. Macroscopic and microscopic analysis of the palato-gingival groove. J Endod. 2000;26:345–50. doi: 10.1097/00004770-200006000-00009. [DOI] [PubMed] [Google Scholar]
- 4.Schäfer E, Cankay R, Ott K. Malformations in maxillary incisors: Case report of radicular palatal groove. Endod Dent Traumatol. 2000;16:132–7. doi: 10.1034/j.1600-9657.2000.016003132.x. [DOI] [PubMed] [Google Scholar]
- 5.Wei PC, Geivelis M, Chan CP, Ju YR. Successful treatment of pulpal-periodontal combined lesion in a birooted maxillary lateral incisor with concomitant palato-radicular groove. A case report. J Periodontol. 1999;70:1540–6. doi: 10.1902/jop.1999.70.12.1540. [DOI] [PubMed] [Google Scholar]
- 6.Friedman S, Goultschin J. The radicular palatal groove - A therapeutic modality. Endod Dent Traumatol. 1988;4:282–6. doi: 10.1111/j.1600-9657.1988.tb00649.x. [DOI] [PubMed] [Google Scholar]
- 7.Lara VS, Consolaro A, Bruce RS. Macroscopic and microscopic analysis of the palato-gingival groove. J Endod. 2000;26:345–50. doi: 10.1097/00004770-200006000-00009. Kerezoudis NP, Siskos GJ, Tsatsas V Bilateral buccal radicular groove in maxillary incisors: Case report Int Endod J 2003;36:898-906. [DOI] [PubMed] [Google Scholar]
- 8.Kozlovsky A, Tal H, Yechezkiely N, Mozes O. Facial radicular groove in a maxillary central incisor. A case report. J Periodontol. 1988;59:615–7. doi: 10.1902/jop.1988.59.9.615. [DOI] [PubMed] [Google Scholar]
- 9.Bacić M, Karakas Z, Kaić Z, Sutalo J. The association between palatal grooves in upper incisors and periodontal complications. J Periodontol. 1990;61:197–9. doi: 10.1902/jop.1990.61.3.197. [DOI] [PubMed] [Google Scholar]