

Abstract
Background:
Bronchial asthma is an important public health problem at the global level. There is paucity of studies on bronchial asthma among school children in Urban India.
Objective:
To assess the prevalence and associated factors of bronchial asthma among school children.
Materials and Methods:
A cross-sectional study was conducted among 263 children studying in the 8th, 9th, and 10th standard using the modified International Study on Allergy and Asthma in Childhood questionnaire in Urban Puducherry. Data on associated factors that include family history of asthma, type of fuel used for cooking, placement of kitchen in the house, number of windows in sleeping room, pet animals, smoking among family members, birth order, and smoke outlet were collected. Data were analyzed by univariate analysis and expressed in proportion or percentages.
Results:
Prevalence of ever bronchial asthma was found to be 5.3%, of which 4.2% had current episode of asthma during the last 1-year period. About 72.7% of the current asthmatics had cold or rhinitis and 54.5% each had itching or rashes and nocturnal dry cough. Prevalence is more among the 12-13 years age group (6.5%) compared to the 14-16 years age group (3.6%). Boys (5.4%) and girls (5.2%) had comparable prevalence rates. The prevalence was significantly more among those with a family history of asthma, having smoking habits in any of the family members, and the absence of smoke outlet in the house (P < 0.05).
Conclusion:
Bronchial asthma is an important health problem among children in urban Puducherry. Intervention on exposure to passive smoking and provision of smoke outlets may help to reduce the burden of disease at the community level.
Keywords: Bronchial asthma, prevalence, school children, urban India
INTRODUCTION
Bronchial asthma is an important health issue, especially in developing countries like India. In the year 2004, India accounted for 277 Disability Adjusted Life Years lost per 1,00,000 population and 57,000 deaths.[1] During the childhood period, bronchial asthma is often underdiagnosed and undertreated, which may lead to severe psychosocial disturbances in the family.[2] National Family Health Survey-3 showed that the prevalence of bronchial asthma among school children of the age group 15-19 years in India is as little as 0.9%, whereas other studies showed varied results ranging from 1.9% to 16.6% in different age groups.[1] In urban areas, this problem is increasing due to increase in environmental smoke and air pollution resulting from urbanization and industrialization. A study conducted in Bangalore city among less than 18 years of age showed that asthma prevalence increased to quite a great extent from the year 1979 (9%) to 1999 (29.5%).[3]
There is paucity of information on the epidemiology of asthma in Urban India.[4] Contribution of each risk factor may vary in different settings and understanding the risk factors associated with asthma such as family history, type of fuel used, pet animals, indoor air pollution, birth order, smoking among family members, and others will help in adopting appropriate preventive strategies. With this background, this cross-sectional study was conducted to assess the prevalence and associated factors of bronchial asthma among school children in Urban Puducherry, India.
MATERIALS AND METHODS
Setting and sample size
This cross-sectional study was conducted during July-August 2012 in three schools of urban field practice area of a Medical Institution in Puducherry. The schools included two Government Schools, namely Calve College and Government Middle School, Kuruchikuppam, and one aided private society school. Since both government and private schools were included, we assume that it represents all the socio-economic strata from the population. Minimum sample size was found to be 250 subjects based on 22% prevalence rate, precision of 25%, and non-response rate of 10%. All 271 students studying in the 8th to 10th standard from the three schools were included as study subjects.
Method of data collection
Prior written permission was obtained from the principals of schools to allow the students to participate in the study. A pretested and validated questionnaire was designed on the lines of the International Study on Allergy and Asthma in childhood questionnaire.[5] This was translated to the local language Tamil and translated back into English to ensure reliability and validity. A pilot test was conducted before initiating the study to consider the feasibility of administration of the questionnaire and accordingly minor modifications were carried out. After obtaining the informed consent, the designated respondent was interviewed as per the questionnaire. A child with symptom of wheezing or whistling in the chest in the past was considered as criteria for defining asthma. Other symptoms associated with asthma, which included numbers of attacks of wheezing, sleep and speech disturbance, and nocturnal cough, were collected.
A semi-structured proforma containing data regarding age and associated factors that include family history of asthma, type of fuel used, placement of kitchen in the house, number of windows in sleeping room, pet animals, smoking among family members, birth order, and smoke outlet were collected.
Statistical analysis
The collected data was entered and analyzed using SPSS (Statistical Package for Social Sciences) version 11.0 for Windows. The findings were expressed in terms of proportions or percentages. Univariate analysis was carried out for associated factors to test the differences between proportions. P < 0.05 was considered as significant.
RESULTS
A total of 263 subjects in the age group of 12-16 years age group were analyzed with a response rate of 97.1%. The study found that most of the children belonged to the 12-13 years age group (58.2%) and were males (63.5%). Prevalence of ever bronchial asthma was found to be 5.3% and 4.2% had a current episode of asthma during the last 1-year period. About 72.7% of current asthmatics had cold or rhinitis. Nearly half (45.5%) of the current asthmatics had >3 episodes of wheezing and 54.5% of them had itching or rashes and nocturnal dry cough. About 18.2% of them were not diagnosed or treated for it [Table 1].
Table 1.
Distribution of symptoms of asthma in the past year, N=11
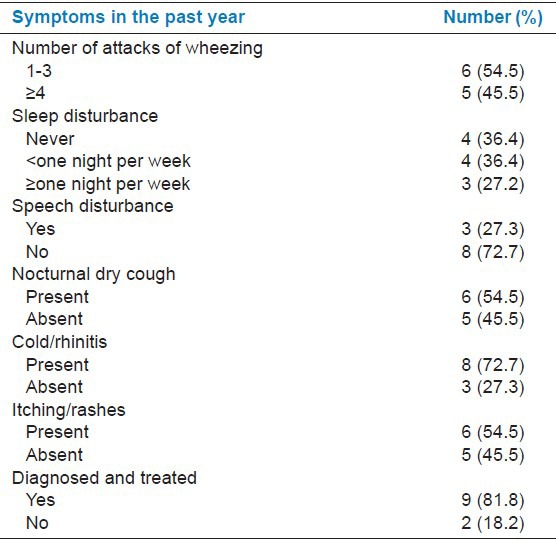
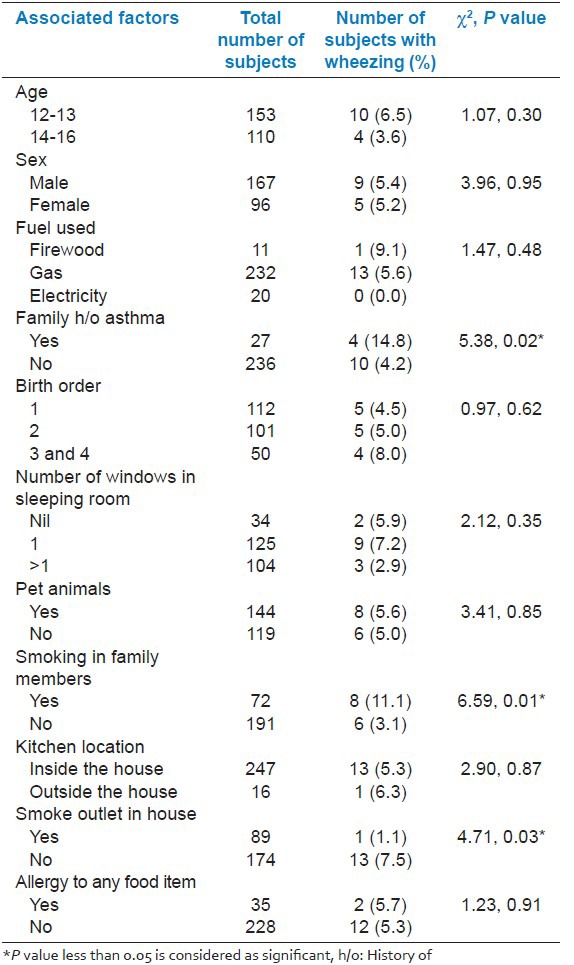
Prevalence of asthma was more among the 12-13 years age group (6.5%) compared to the 14-16 years age group (3.6%); however, this difference was not found to be significant. Boys (5.4%) and girls (5.2%) had comparable prevalence rates of asthma. It was found that prevalence was significantly more among those with a family history of asthma, having smoking habits in any of family members, and the absence of smoke outlet in the house (P < 0.05) [Table 2].
Table 2.
Associated factors of asthma among school children in Urban Puducherry
DISCUSSION
Bronchial asthma among children is an important health issue for the concerned authorities in developing countries like India. A recent review analysis of 15 epidemiological studies showed that the mean prevalence of asthma among children was 7.24%. Urban and male predominance was observed with wide interregional variation.[4] Recent studies in India showed varied prevalence rates in different age groups and locations ranging from 0.9% to 15.7%.[6,7,8,9,10,11,12,13] The low level of prevalence found in National Family Health Survey-3 (2005-06) may be because of the lesser sensitivity of the questionnaire and self-reporting or lack of uniformity in the data collection process.
Studies have shown that prevalence is more in urban areas compared to rural areas.[4,9] A study conducted in Shimla city among school children aged 6-13 years showed the prevalence as 2.3%.[12] Another study from Jaipur conducted among urban school children aged 5-15 years showed the prevalence of asthma as 7.59%.[13] A study conducted in Bangalore among school children aged 6-15 years in heavy traffic area showed prevalence as high as 19.34%.[3] The prevalence of ever asthma was reported as 2.4% in a population study on 73,605 individuals of all age groups conducted simultaneously at four major centers in India.[14] Prevalence of asthma and wheeze reported were 3.3% and 7.8%, respectively, in a study conducted at Lucknow, in the age group 13-14 years.[8]
Studies from rural areas also show different prevalence rates. A recent study from rural Puducherry showed the prevalence as 8.6%, which is higher than that found in the present study.[15] A rural study from Karnataka showed the prevalence of bronchial asthma among the 6-15 years age group as 10.3%.[6] The prevalence of ever wheezers in a study among 10-18 years age group from rural Karnataka was 8.4% and current wheezers was 5.2%.[11] However, in general it was found that prevalence rate is more in the United Kingdom, Canada, Australia, New Zealand, Brazil, and other developed countries, ranging from 15% to 20%.[1,16,17] A very high prevalence of history of wheezing was found in three studies in Costa Rica with 46.8%, 42.9%, and 45.1% in different age groups conducted among school children.[18] In contrast to this, it was shown by an Indian study that prevalence of asthma among adults aged ≥15 years is 2.05%.[19] This variation may be because of the difference in the exposure status of different risk factors in different geographical locations. Moreover, the definition of asthma, instrument used to define it, age group studied, methodology adopted, and urban – rural difference – all were responsible for this varied observation.
The prevalence of asthma was similar in both sexes in contrast to other studies.[4,6] It was comparatively more among younger age groups similar to other studies.[4] It was observed in our study that prevalence is significantly more among those with a family history of bronchial asthma similar to other studies.[6,15] Indoor air pollution due to biomass or solid fuel combustion is an important risk factor in the Indian setting.[3,20] Although the prevalence is more among those using firewood, we could not find any association with it. Our study has shown that the proportion of cases was significantly less among those who live in houses with smoke outlets. Exposure to passive tobacco smoke was shown to be an important risk factor in our study, similar to that in other studies.[14,21,22] A study has shown interactions between genotypes at specific loci or genome regions and environmental tobacco smoke exposure with risk for development of asthma.[23]
We could not find any association between bronchial asthma and factors like pets at home, birth order, and absence of windows in living rooms in contrast to other studies.[1,7,15] The study findings may not be generalized due to the different socio-demographic characteristics and the associated risk factors in the different settings. In addition, quantification of some of the risk factors could not be ascertained and diagnostic tests could not be conducted due to feasibility constraints.
CONCLUSION
Asthma among school children is a public health problem in urban Puducherry. Our study provides valuable information on the magnitude of the problem and certain risk factors, which can be utilized for preventive measures to be taken in the future. Intervention on exposure to passive smoking and provision of smoke outlets may help in the reduction of burden of disease at the community level. Further studies are required to explore the risk factors of bronchial asthma among children in different geographical regions.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Sutapa Agrawal. South Asia Network for chronic Disease. New Delhi, India: 2010. [Last accessed 2012 Oct 20]. Factsheet on Asthma in India. Available from: http//www.sancd.org/uploads/pdf/Asthma_factsheet.pdf . [Google Scholar]
- 2.Von Mutius E. The burden of childhood asthma. Arch Dis Child. 2000;82(Suppl 2):ii2–ii5. doi: 10.1136/adc.82.suppl_2.ii2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Paramesh H. Epidemiology of asthma in India. Indian J Pediatr. 2002;69:309–12. doi: 10.1007/BF02723216. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Pal R, Dahal S, Pal S. Prevalence of bronchial asthma in Indian children. Indian J Community Med. 2009;34:310–6. doi: 10.4103/0970-0218.58389. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Asher MI, Keil U, Anderson HR, Beasley R, Crane J, Martinez F, et al. International Study of Asthma and Allergies in Childhood (ISAAC): Rationale and methods. Eur Respir J. 1995;8:483–91. doi: 10.1183/09031936.95.08030483. [DOI] [PubMed] [Google Scholar]
- 6.Jain A, Vinod Bhat H, Acharya D. Prevalence of bronchial asthma in rural Indian children: A cross sectional study from South India. Indian J Pediatr. 2010;77:31–5. doi: 10.1007/s12098-009-0308-6. [DOI] [PubMed] [Google Scholar]
- 7.Pokharel PK, Kabra SK, Kapoor SK, Pandey RM. Risk factors associated with bronchial asthma in school going children of rural Haryana. Indian J Pediatr. 2001;68:103–6. doi: 10.1007/BF02722022. [DOI] [PubMed] [Google Scholar]
- 8.Awasthi S, Kalra E, Roy S, Awasthi S. Prevalence and risk factors of asthma and wheeze in school-going children in Lucknow, North India. Indian Pediatr. 2004;41:1205–10. [PubMed] [Google Scholar]
- 9.Chakravarthy S, Singh RB, Swaminathan S, Venkatesan P. Prevalence of asthma in urban and rural children in Tamil Nadu. Natl Med J India. 2002;15:260–3. [PubMed] [Google Scholar]
- 10.Narayana PP, Prasanna MP, Narahari SR, Guruprasad AM. Prevalence of asthma in school children in rural India. Ann Thorac Med. 2010;5:118–9. doi: 10.4103/1817-1737.62478. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Dhabadi BB, Athavale A, Meundi A, Rekha R, Suruliraman M, Shreeranga A, et al. Prevalence of asthma and associated factors among schoolchildren in rural South India. Int J Tuberc Lung Dis. 2012;16:120–5. doi: 10.5588/ijtld.11.0195. [DOI] [PubMed] [Google Scholar]
- 12.Behl RK, Kashyap S, Sarkar M. Prevalence of bronchial asthma in school children of 6-13 years of age in Shimla city. Indian J Chest Dis Allied Sci. 2010;52:145–8. [PubMed] [Google Scholar]
- 13.Sharma BS, Kumar MG, Chandel R. Prevalence of asthma in urban school children in Jaipur, Rajasthan. Indian Pediatr. 2012;49:835–6. doi: 10.1007/s13312-012-0188-0. [DOI] [PubMed] [Google Scholar]
- 14.Jindal SK. Bronchial asthma: The Indian scene. Curr Opin Pulm Med. 2007;13:8–12. doi: 10.1097/MCP.0b013e32800ffd09. [DOI] [PubMed] [Google Scholar]
- 15.Kumar SG, Premarajan KC, Sarkar S, Sahu SK, Sahana, Ambika, et al. Prevalence and factors associated with asthma among school children in rural Puducherry, India. Curr Pediatr Res. 2012;16:159–63. [Google Scholar]
- 16.de Luna Mde F, Almeida PC, Silva MG. Prevalence of asthma among adolescents in the city of Fortaleza, Brazil. J Bras Pneumol. 2009;35:1060–7. doi: 10.1590/s1806-37132009001100002. [DOI] [PubMed] [Google Scholar]
- 17.Maia JG, Marcopito LF, Amaral AN, Tavares Bde F, Santos FA. Prevalence of asthma and asthma symptoms among 13 and 14-year-old school children, Brazil. Rev Saude Publica. 2004;38:292–9. doi: 10.1590/s0034-89102004000200020. [DOI] [PubMed] [Google Scholar]
- 18.Soto-Quiros ME, Soto-Martinez M, Hanson LA. Epidemiological studies of the very high prevalence of asthma and related symptoms among school children in Costa Rica from 1989 to 1998. Pediatr Allergy Immunol. 2002;13:342–9. doi: 10.1034/j.1399-3038.2002.02035.x. [DOI] [PubMed] [Google Scholar]
- 19.Jindal SK, Aggarwal AN, Gupta D, Agarwal R, Kumar R, Kaur T, et al. Indian study on epidemiology of asthma, respiratory symptoms and chronic bronchitis in adults (INSEARCH) Int J Tuberc Lung Dis. 2012;16:1270–7. doi: 10.5588/ijtld.12.0005. [DOI] [PubMed] [Google Scholar]
- 20.Agrawal S. Effect of indoor air pollution from biomass and solid fuel combustion on prevalence of self-reported asthma among adult men and women in India: Findings from a nationwide large-scale cross-sectional survey. J Asthma. 2012;49:355–65. doi: 10.3109/02770903.2012.663030. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Parasuramalu BG, Huliraj N, Rudraprasad BM, Prashanth Kumar SP, Gangaboraiah, Ramesh Masthi NR. Prevalence of bronchial asthma and its association with smoking habits among adult population in rural area. Indian J Public Health. 2010;54:165–8. doi: 10.4103/0019-557X.75742. [DOI] [PubMed] [Google Scholar]
- 22.Sharma SK, Banga A. Prevalence and risk factors for wheezing in children from rural areas of north India. Allergy Asthma Proc. 2007;28:647–53. doi: 10.2500/aap.2007.28.3059. [DOI] [PubMed] [Google Scholar]
- 23.Kurz T, Ober C. The role of environmental tobacco smoke in genetic susceptibility to asthma. Curr Opin Allergy Clin Immunol. 2004;4:335–9. doi: 10.1097/00130832-200410000-00002. [DOI] [PubMed] [Google Scholar]