

Abstract
Although the morphological features of hepatitis C virus (HCV) recurrence after orthotopic liver transplantation (OLT) have been well established in the last decades, the differential diagnosis still represents a challenge for the pathologist, especially early recurrent hepatitis C vs mild acute cellular rejection. The present review focuses on the role of the pathologist and the pathology laboratory in the management of recipients with recurrent hepatitis C, the usefulness of early and late post-OLT liver biopsies, and the potential role of ancillary techniques (immunohistochemistry and reverse transcription-polymerase chain reaction, RT-PCR). The English literature on the topic is reviewed, focusing on the histopathology, the immunohistochemistry and the use of RT-PCR on HCV-positive post-OLT biopsies. The different histopathological illustrations of early and chronic recurrent hepatitis C are presented, with special focus on the main differential diagnoses and those features with prognostic relevance (cholestasis above all). The usefulness of ancillary techniques are discussed, especially HCV RNA quantitation by RT-PCR. Finally, the usefulness of long-term protocol biopsies is addressed: their usefulness for the study of allograft disease progression is clear, but their meaning in the long term is still debated. The significance of plasma cell infiltrate in HCV-positive allografts, the prognostic weight of graft steatosis, and the impact of donor age in recurrent hepatitis C also represent additional open issues.
Keywords: Hepatitis C virus, Histopathology, Immunohistochemistry, Orthotopic liver transplantation, Recurrent hepatitis C, Polymerase chain reaction
Core tip: Recently, tissue hepatitis C virus (HCV) RNA quantitation by means of reverse transcription-polymerase chain reaction has been largely used in the early post-orthotopic liver transplantation (OLT) phases, especially in the differential diagnosis of recurrent hepatitis C vs mild acute rejection, replacing immunohistochemistry in some laboratories. Nevertheless, the importance of tissue HCV RNA quantitation in the long post-OLT term has not been clarified yet. The suitability and usefulness of protocol biopsies are still debated: protocol biopsies may be necessary in order to answer other open questions, such as the significance of plasma cell infiltrate in HCV-positive allografts, the prognostic weight of HCV-induced steatosis, and the impact of donor age in recurrent hepatitis C.
INTRODUCTION
End-stage liver disease due to chronic hepatitis C virus (HCV) infection is the leading indication for orthotopic liver transplantation (OLT) in Western countries[1]. HCV reinfection is virtually universal after OLT, and up to 70% of patients are expected to experience histological recurrent hepatitis C[2-13], with a higher risk of graft loss and mortality compared to recipients undergoing transplantion for other etiologies[5,14-16]. It is noteworthy that the incidence of HCV disease in allografts has increased since the nineties according to the literature, probably due to the application of more effective immunosuppression regimens. Indeed immunosuppression, especially the steroid boluses given in the case of acute cellular rejection (ACR), inevitably accelerate the virus-mediated graft damage, with a more aggressive course compared with HCV disease in native livers[17-20]. Although some authors have recently underlined a good outcome of HCV-positive recipients at 5 years after OLT[13], recurrent hepatitis C still represents the major cause of graft failure.
In this setting, it is now recognized that the histopathological analysis of post-OLT liver biopsies can produce valuable data for the diagnosis and prognosis of recurrent hepatitis C, and therefore for the management of HCV-positive recipients, though in this case, no universal approach is recognized. Moreover, the histopathological diagnosis of recurrent hepatitis C implies many pitfalls and a wide range of differential diagnoses, and it can be very challenging especially in the early post-OLT phases.
The present review focuses on the role of pathologist and pathology laboratory in the diagnosis of recurrent hepatitis C, the objective usefulness of early and late post-OLT liver biopsies, and the potential role of ancillary techniques in the diagnosis and prediction of the disease progression.
LIVER BIOPSY IN EARLY ACUTE RECURRENT HEPATITIS C
The timing and the indications of post-OLT liver biopsies represent a key step in the management of HCV-positive recipients. Although the decision is normally made by the surgical team, and therefore does not directly involve the pathologist, the practice of protocol biopsies after OLT might influence the whole transplant team.
As early recurrent hepatitis C, as well as the early allograft damage that can simulate it, are clinically and serologically evident, early liver biopsies are usually performed for established clinical indications. Moreover, complications after liver biopsy are rare but potentially serious, and the histopathological report of a biopsy performed with normal tests does not usually influence the therapeutic approach[21]. For these reasons, there has been a progressive cessation of early protocol biopsies in many centers. In our center, protocol biopsies are not performed, and we introduced the concept of “first-event” biopsy. The “first-event” biopsy is defined as the biopsy taken at the very first increase in transaminase level and/or clinical worsening after OLT[22]. Although we realize that this approach cannot be free from selection bias, the histopathological and reverse transcription-polymerase chain reaction (RT-PCR) studies of the tissue obtained from the “first-event” biopsies can provide valuable diagnostic and prognostic data on HCV recurrent disease (see also the RT-PCR section)[22,23].
The onset of “typical “ acute recurrent hepatitis C is generally recorded within 4-12 wk after OLT, but according to Demetris, it “can be detected as early as 10 to 14 d”[12]. Saraf et al[24] reported a case of a woman who experienced recurrent hepatitis C at day 9, attributing the early onset to the advanced donor and recipient ages. In our most recent experience, 75% of HCV-positive recipients had a histopathological diagnosis of recurrent hepatitis C after a mean of 86 d, but with a high variability, including a case of recurrent hepatitis C after 3 d[22]. This finding is in agreement with Pacholczyk et al[13], who reported the minimum recurrence time in their series at 5 d. These “extreme” cases of early recurrent hepatitis C are very rare, but they are not to be excluded a priori, also taking into account HCV virulence and immunosuppression suitability. In any case, experience has taught us that the diagnosis of recurrent hepatitis C after such a short period requires tissue HCV RNA quantitation, as well as the clinical and histopathological exclusion of other possible causes of graft damage, e.g., ACR, early surgical complications, ischemia/reperfusion injuries, and other early complications, which have a much higher incidence in the first days after OLT.
HISTOPATHOLOGY OF EARLY RECURRENT HEPATITIS C
Typical acute recurrent hepatitis C
On the basis of nearly 20 years of publications, Demetris classified the histopathological presentation of recurrent hepatitis C into three groups: the “typical” presentation (acute and chronic), fibrosing cholestatic HCV hepatitis (FCH), and a plasma cell-rich variant[12]. Each of these histopathological variants can be intertwined with other post-OLT complications (ACR above all).
Lobular hepatitis observed in “typical” acute recurrent hepatitis C is similar to the acute viral damage observed in the very first phases of hepatitis C in non-transplanted livers, but has very low (or absent) portal tract involvement. In particular, early recurrent hepatitis C is characterized by lobular architectural disarray with Councilman bodies and spotty necrosis, Kupffer cells activation, and mild lymphocytic sinusoidal infiltrate[1,12,25,26] (Figure 1). The Councilman bodies (or acidophilic bodies) are the expression of the apoptotic death of hepatocytes during lobular damage. The formation of apoptotic bodies was described during hepatitis C, both in native livers and OLT allografts, as a consequence of several mechanisms including direct cytotoxicity by HCV, activation of the extrinsic apoptotic pathway by the recipient immune system, and sensitization to the FasL/CD95 intrinsic pathway by HCV core proteins[27-29]. In the OLT setting, the morphological features are further complicated by immunosuppression. The first quantitation of Councilman bodies in the allograft differential diagnosis was performed in 2002 by Saxena et al[30], who found a two-fold higher mean number of apoptotic bodies per cm2 in recurrent hepatitis C than in ACR. The authors also suggested that the finding of > 50 acidophilic bodies in the whole biopsy was strongly indicative of recurrent hepatitis C[30]. Some years later, in order to obtain more reproducible results, our group evaluated the so-called “Councilman bodies/portal tract ratio” (“C/P ratio”), which simply represents the mean number of Councilman bodies for each portal tract counted in the biopsy[22,23]. The C/P ratio was the only histopathological variable able to discriminate recurrent hepatitis C from other conditions, as well as the only variable directly correlated with the intrahepatic HCV RNA load. Moreover, high-risk recipients showed more Councilman bodies than others, with a mean C/P ratio of 1.5 (see below)[22].
Figure 1.
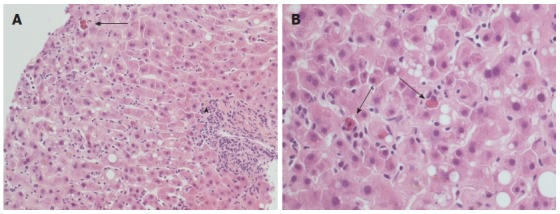
Typical histopathological appearance of acute recurrent hepatitis C. A: Lobular architectural disarray, lobular necrosis with lymphocytic sinusoidal infiltrate and visible Councilman bodies (black arrow) are evident, as well as a mild portal tract inflammation (arrowhead); hematoxylin-eosin stain, × 20 magnification; B: Detail of the same case at × 40 magnification: note the high number of Councilman bodies in a single field (black arrows), and a minimal amount of macrovesicular steatosis.
Histopathological variants: Fibrosing cholestatic HCV hepatitis
FCH is a quite peculiar presentation of recurrent hepatitis C, although it was first described in a HBV-positive OLT recipient[31]. FCH is characterized by an early onset (within 1 year) and an overall poor prognosis, due to the rapid fibrosis progression and the poor response to conventional antiviral therapies[6,32]. At histology, FCH shows hepatocyte swelling and ballooning, spotty necrosis with Councilman bodies, cholestasis with ductular reaction and a ductular-type interface activity, with a mild mixed portal infiltrate (Figure 2A-C). Late alterations include periportal fibrosis and cirrhosis (Figure 2D)[6,12,32-35]. In a previous study on 10 FCH cases (on 135 HCV-positive recipients), the median hepatitis activity grade and the Banff score were significantly higher than in “usual” acute recurrent hepatitis C[34]. The occurrence of a peculiar sinusoidal pattern of fibrosis was also described as important for the diagnosis of FCH[34]. According to a recent paper, the diagnosis of “cholestatic HCV” requires at least three out of four histological features (ductular reaction, cholestasis, hepatocyte ballooning and periportal sinusoidal fibrosis), 1 mo after OLT, after exclusion of other causes of cholestasis. These histological features seem to have a prognostic meaning as well[35].
Figure 2.
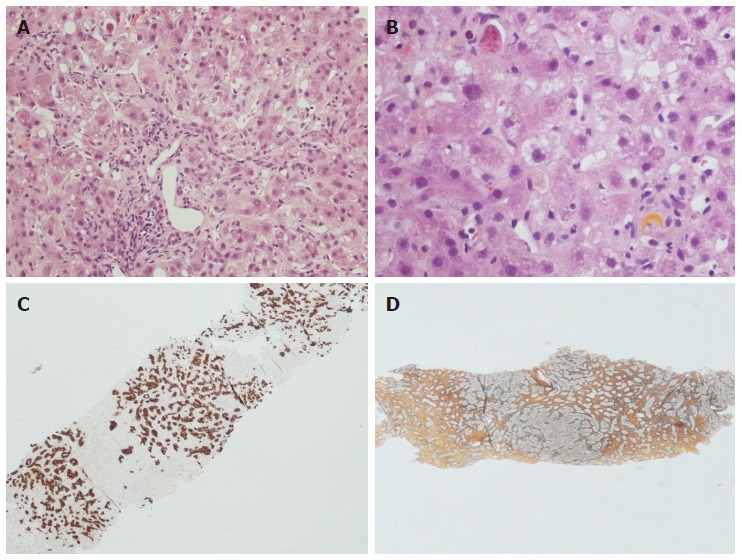
Histopathological appearance of fibrosing cholestatic recurrent hepatitis C. Hematoxylin-eosin stain × 10 (A) and × 40 (B) magnification: note the lobular architectural disarray, the portal tract fibrosis and distortion, the lobular necrosis with Councilman bodies and the cholestasis with hepatocellular feathery degeneration and ballooning. The immunohistochemistry for keratin 19 (C) highlights the prominent ductular reaction, while the reticulin stain (D) indicates advanced fibrosis.
FCH is likely to affect over-immunosuppressed recipients[36], with a massive viral replication, as reflected by the occurrence of very high viral loads in both serum and liver tissue, as reported in different papers from the end of the nineties[22,33,37]. Notably, in one paper, the tissue HCV RNA levels in the native explanted liver correlated with a higher risk of FCH[38].
Histopathological variants: Plasma cell-rich recurrent hepatitis, a still open issue
In 2007, Khettry et al[11] described nine cases (10% of their series) of recurrent hepatitis C with periportal and centrolobular necrosis and inflammation, characterized by a prominent plasma cell component. The authors named this entity “post-liver transplantation autoimmune-like hepatitis” and postulated that the interplay among the recipient’s immune system, HCV replication and antigenicity, and immunosuppression therapy might occur in the development of this “hyperimmune” inflammatory reaction. Furthermore, although on the basis of non-scheduled biopsies, this “autoimmune-like hepatitis” seemed to be related to fibrosis progression[11]. In the same period, Fiel et al[39] highlighted that more than 80% of “plasma cell hepatitis” in their series occurred after a reduction in immunosuppression (calcineurin inhibitors), and that 55% had at least one previous episode of rejection. These findings led the authors to the conclusion that the plasma cell hepatitis was a form of rejection. An editorial by Demetris et al[45] in the same year underlined that HCV can stimulate some types of autoimmune alterations both in allografts and native livers[12]. Moreover, antiviral therapy can unleash “autoimmune-mediated” liver damage, as described for pegylated-interferon with or without ribavirin[40-43]. Finally, a case-control study described the worse prognosis of plasma cell-rich hepatitis, which interestingly was also correlated with the presence of plasma cells in the explanted liver in one study, suggesting the existence of an immunological “disposition” in some patients[44]. In 2009, Demetris classified the plasma cell-rich “autoimmune” hepatitis as a histopathological variant of recurrent hepatitis C, albeit stating that “determining whether this represents an autoimmune variant of HCV, acute rejection, actual autoimmune hepatitis, or a combination of these possibilities requires a more thorough patient evaluation than what is currently done at most centers and further study”[12,45].
Histopathological variants: recurrent hepatitis C with granulomas
Not included in the Demetris’ classification of 2009[12], was the possibility of a liver granulomatous reaction as presentation of HCV recurrent disease, first postulated in a case reported by Bárcena et al[46], although HCV was already listed as a possible cause of post-OLT granulomas in a series of 42 recipients in 1995[47]. Ten years later, non-necrotizing lobular (more rarely portal) granulomas were observed in unscheduled biopsies of four (8%) out of 53 HCV-positive recipients[48]. After the exclusion of other etiologies, the authors ascribed the granulomatous disease to hepatitis C. In another retrospective study in the same period, granulomas were found in 14 (1.7%) out of 820 HCV-positive recipients[49]. In this series, 10 cases were found on protocol biopsies, and four on biopsies performed for clinical indications: the prevalent lobular localization of the granulomas was confirmed, and since most patients received pegylated interferon, the authors hypothesized that “granuloma formation may be indicative of antiviral stimulation against intrahepatic HCV”[49]. The question whether this very rare biopsy finding represents a form of antiviral immune reaction, ultimately drug-modulated, still remains open, as is the role of the granulomatous reaction in fibrosis progression and graft survival.
“CHOLESTATIC” RECURRENT HEPATITIS C: PROGNOSTIC ROLE OF POST-OLT LIVER BIOPSY
Apart from the assessment of fibrosis progression, which will be discussed below, histopathological evaluation can play a prognostic role in the identification of those morphological features predictive of a worse outcome. In addition to some still debated histopathological characteristics, e.g., steatosis[50,51], apoptosis, or bile duct proliferation[52], another feature with a well-known impact on recipient outcome is cholestasis (Figure 3). The relationship between cholestasis and a more severe form of recurrent hepatitis C is well established[6,53]. Recently, Moreira et al[54] proposed the so-called “Histological Aggressiveness Score”, based on the presence or absence of a prominent ductular reaction, hepatocellular ballooning, cholestasis, and periportal/sinusoidal fibrosis, all features typical of the most severe form of recurrent hepatitis C, i.e., FCH. In this study, 170 recipients were stratified into three risk groups using these four histopathological features, which are not included in the conventional grading systems of chronic hepatitis[54]. In our recent experience, the occurrence of a cholestatic recurrent hepatitis C was associated with a significantly higher tissue HCV RNA, and also with a poorer outcome[22]. Although we agree that FCH is by far one of the most aggressive forms of recurrent hepatitis C, we also believe that severe HCV recurrence is not always an indication of FCH. In our routine experience, more “traditional” features such as the amount of lobular necrosis (i.e., Councilman bodies), as well as the quantitation of intrahepatic HCV RNA (as mentioned below), are strong predictors of a poor outcome as well. Nonetheless, our results are in agreement with Moreira’s, since 35% of our “high-risk group” (or group 3, with both tissue and serum high viral loads) experienced a cholestatic recurrent hepatitis C[22]. It should be borne in mind that Moreira et al[54] excluded recipients with post-OLT biliary complications from their study; conversely, we included these recipients in our series, since a connection between recurrent hepatitis C and post-OLT biliary complications has been previously proposed[55]. We found that most recipients with previous biliary complications belonged to the “high risk group”[22]. Future studies are required to investigate the intriguing cross-connection among biliary complications, HCV replication and recurrent hepatitis C.
Figure 3.
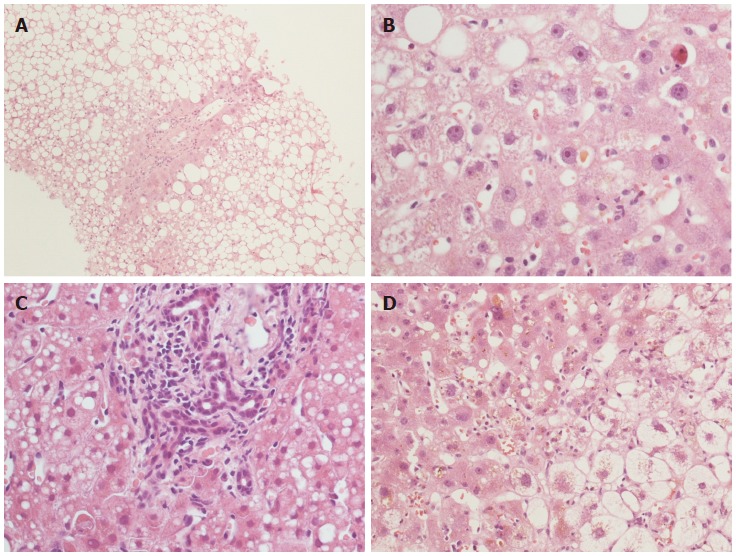
Histopathological features with a prognostic significance in recurrent hepatitis C. Steatosis (A) and cholestasis (B) are well shown. Cholestasis can be associated with bile duct proliferation (C) and/or hepatocellular ballooning (D). Hematoxylin-eosin stain, × 10 (A) and × 40 (B-D) magnification.
CHRONIC RECURRENT HEPATITIS C: THE PROTOCOL LIVER BIOPSY QUESTION
Protocol biopsies and fibrosis progression
Chronic (late) recurrent hepatitis C generally presents 6-12 mo after OLT. The main morphological features are portal tract inflammatory infiltrate, mostly composed of lymphocytes, with interface hepatitis and ductular reaction; the lobular necrosis with hepatocellular polymorphism persists depending also on the response to anti-viral therapy[4,12,20,56]. The overall picture becomes similar to the histopathological presentation of C hepatitis in native livers. The differential diagnosis of chronic recurrent hepatitis C is usually not difficult for the pathologist, because of the typical histological picture, and because the diagnosis of hepatitis C in liver allograft has already been made on clinical grounds, if not with a previous biopsy. Therefore, there is no full agreement on the usefulness and indications of liver biopsy in this phase, since fibrosis progression in allografts represents the only valuable parameter in the long term for prediction of OLT outcome[10,57-60]. The severity of fibrosis progression in the allograft is determined early: some authors demonstrated that hepatitis grade and fibrosis stage within the first year after OLT might identify those patients with a possible rapid fibrotic evolution[18,52,61]. In order to evaluate and follow fibrosis progression, some centers adopt annual protocol liver biopsies, while others favor the clinical follow-up, with the execution of biopsies only in the case of an increase in transaminase levels or worsening of the clinical picture.
In a first key study conducted on recipients followed by protocol biopsies, Gane et al[5] concluded that recipients with moderate chronic hepatitis at 1 year bore a significantly higher risk of cirrhosis development at 5 years, than recipients with mild hepatitis activity. Years later, large analyses on the usefulness of long-term protocol biopsies showed that the proportion of healthy allografts tended to decrease with time after OLT[62,63]. Moreover, in a series of 245 patients with at least 1 year of follow-up the presence of normal transaminase levels virtually excluded liver damage in non-HCV recipients, while in HCV-positive recipients, the serum tests seemed to be less sensitive, and the authors concluded that the long-term protocol biopsies were useful to assess the progression of recurrent hepatitis C[62]. This is confirmed by the fact that most centers worldwide do not perform long-term protocol biopsies for indications other than HCV[21], while in HCV-positive recipients protocol biopsies are still applied in most centers.
The assessment of the hepatitis grade is important as well, as it correlates with staging and fibrosis progression[57,64,65]. Firpi et al[66] found that a fibrosis stage > 2 according to Ishak and/or an hepatitis activity index > 4 at 1 year correlated with a faster fibrosis progression. In a highly selected series of patients, Baiocchi et al[67] found a strong relationship between grade (especially portal inflammation) and fibrosis progression after 1 year. Furthermore, in a series of 159 patients, Ghabril et al[68] found that the HCV activity grade (Ishak > 4) even in the explanted liver was predictive of a more rapid graft fibrosis progression after OLT.
In a series, the fibrosis progression in HCV-positive recipients was calculated as 0.8 units (according to Ishak) per year; interestingly, this mean value increased with donor age > 55 years, and decreased with donor age < 35 years[66]. Donor age was confirmed to be an important predictor of faster fibrosis progression in HCV-positive recipients also in further studies[69-74], although not in others[65,75]. Other risk factors include viral quasi-species, number of episodes of ACR, and changes in immunosuppression, as well as the sustained virological response to antiviral therapy[52,58,76].
Graft steatosis in recurrent hepatitis C
Steatosis is another long-term histopathological alteration that was firstly considered specific of HCV recurrent disease after OLT in the past[77], especially in association with the HCV genotype 3[78,79], and it was described also in C hepatitis in non-transplanted livers[80]. Recently, Brandman et al[50] have confirmed the presence of some degree of steatosis in nearly 30% (45 out of 152) HCV-positive recipients 1 year after OLT, especially with genotype 3 infection. HCV can directly induce steatosis by alteration of mitochondrial functions or by interference with the lipid metabolism pathway[79]. However, many factors other than HCV infection are likely to play a role in graft steatosis, including donor-specific characteristics such as donor age, or the occurrence of pre-transplant hypertension[50]. This issue surely deserves further studies, since post-OLT steatosis and metabolic syndrome seem to be related, with a higher risk of fibrosis progression 1 year after OLT[50,70,81,82], although not all investigators agree[83,84].
HISTOPATHOLOGICAL DIFFERENTIAL DIAGNOSES OF RECURRENT HEPATITIS C
Recurrent hepatitis C vs acute cellular rejection
The most important differential diagnosis in the early post-transplant phases lies between recurrent viral hepatitis and ACR, especially of mild grade, and is primarily based on liver biopsy[12,26]. Actually, fully reliable guidelines clearly distinguishing recurrent hepatitis C from mild ACR at histology are not available yet, and the diagnosis is still characterized by low inter- and intra-observer agreement[85]: pathologist experience and the interplay between clinician and pathologist play a pivotal role in diagnosis and recipient management. The more characteristic histopathological features of early recurrent hepatitis C are lobular necrosis, steatosis, and Kupffer cell hyperplasia[26,30,32]. Conversely, the commonest findings in ACR include mixed portal tract inflammatory infiltrate with interface hepatitis, bile duct damage and venulitis, with or without lobular damage[30,86,87] (Figure 4), although in mild ACR these morphological features can be lacking in small biopsies. Since ACR and recurrent hepatitis C often co-exist in the same allograft[12], and since early HCV recurrent disease can sometimes mimic some ACR features (e.g., venulitis or biliary damage)[88,89] (Figure 4C and G), it was also suggested that the Banff criteria should be downgraded in HCV-positive recipients. For example, ACR should be diagnosed only in cases with > 50% of portal tract inflammation with biliary damage and/or > 50% of venulitis[26]. The relevance of this topic is that an ACR over-diagnosis might lead to over-immunosuppression, with serious consequences on HCV replication and graft survival. In fact, in order not to lose any graft to rejection, it is the protocol of many institutions to give the recipient a steroid bolus even only on the basis of a clinical suspicious of ACR, sometimes without liver biopsy. Although the typical features of ACR and HCV recurrence are easily recognizable when singularly present, the “overlap” of the two conditions still represents a challenge for the pathologist; in our institution RT-PCR for HCV RNA quantitation is mostly used for this differential diagnosis, as also suggested by others[23,28,90,91]. Other important, albeit less frequent conditions that are included in the differential diagnosis with early recurrent hepatitis C are ischemia/reperfusion injury, post-OLT surgical complications, and drug reactions. Of note, the occurrence of preservation injuries in HCV-positive recipients was correlated with a poorer outcome[92].
Figure 4.
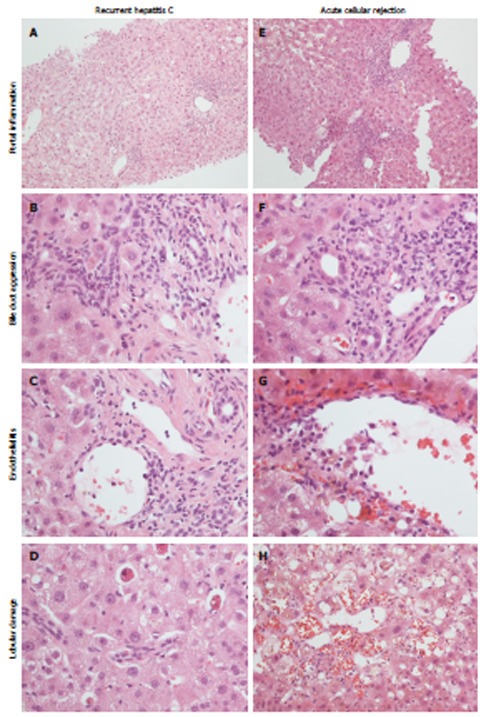
Histopathological appearance of recurrent hepatitis C (left) and acute cellular rejection (right). Portal inflammation is commonly mild in recurrent hepatitis C (A), with a predominant lympho-monocytic infiltrate and mild bile duct invasion (B), while in acute cellular rejection there is a mixed and more pronounced inflammatory infiltrate (E), with evident bile duct invasion (F). Endothelialitis can be found in both conditions (C, G). Lobular necrosis is more typical of recurrent hepatitis C (D); in acute cellular rejection hemorrhage and sinusoid dilatation are more evident (H).
Other differential diagnoses
The FCH histopathological picture is quite peculiar, and the main differential diagnoses include: ischemic injury due to hepatic artery thrombosis, extrahepatic biliary obstruction, adverse drug reactions, and chronic rejection (after 6 mo). All these conditions are characterized by hepatocyte ballooning, perivenular centro-lobular necrosis, cholestasis and Kupffer cell activation, as seen in FCH[32,35,93]. However, some features are distinctive of particular conditions, such as pilocytic neutrophil infiltrate in ascending cholangitis, portal edema, ductular reaction with neutrophils, and periductular fibrosis in large bile duct obstruction, and a scarcity of biliary ducts with mild portal inflammation in chronic rejection. In this latter case, the timing is important too. Finally, the distinction between FCH and “typical” recurrent hepatitis C, with or without fibrosis or cholestasis, is mainly based on the rapidity of graft failure and the lack of response to antiviral therapy. However, histology alone cannot be enough for a certain diagnosis of FCH, and the clinical picture, together with HCV RNA quantitation are required[94].
As discussed above, the differential diagnosis of plasma cell-rich hepatitis is very difficult, also because the distinction between “autoimmune” damage, “hyperimmune” damage (HCV- or drug-induced), and “alloimmune” damage (i.e., a plasma cell-rich rejection) is not always sharp. The clinical setting is crucial for the correct diagnosis of the recipient: the occurrence of de novo autoimmune antibodies (antinuclear antibodies, smooth muscle antibodies, LKM1 > 1:320 and anti-GSTT1), a concurrent autoimmune disease and/or the serum markers can lead to the diagnosis of de novo autoimmune hepatitis[12,39]. According to a recent proposal by Fiel et al[39], a diagnosis of de novo autoimmune hepatitis is recommended when plasma cells represent at least 30% of the total inflammation, and interface hepatitis and lobular necrosis are mainly represented by plasma cells.
Cytomegalovirus (CMV) infection is a common complication of OLT (up to 17%)[95], and is not likely to influence the course of HCV disease or ACR[96]. Since the distinctive features of CMV infection (e.g., nuclear inclusions) are frequently absent in the post-OLT biopsy, lobular necrosis and disarray together with variable portal inflammation can add to the differential diagnosis in early recurrent hepatitis C[95]. Other non-specific, albeit helpful morphological findings in CMV infection, apart from the typical inclusions, are represented by mild bile duct damage, lobular microabscesses and lobular microgranulomas. In cases where CMV infection is suspected, specific immunohistochemistry (IHC) is recommended.
Chronic recurrent hepatitis C is characterized by a portal mononuclear infiltrate with variable degrees of interface hepatitis. The biliary damage can be present, but it is not as severe and/or widespread as in chronic rejection, where bile duct regression can be the prevalent feature, also in the absence of inflammatory infiltrate[12].
ANCILLARY TECHNIQUES: IMMUNOHISTOCHEMISTRY
HCV detection in liver tissue
Since the nineties, many studies have tried to investigate the possible use of IHC to establish the presence of HCV antigens (mainly nonstructural antigen 4 or NS4, and c-100) in liver tissue. Notably, almost all these studies identified some grade of IHC positivity in HCV-positive patients, but without correlations with the histological findings and the clinical data[97-101]. However, it must be borne in mind that these IHC techniques often lacked reproducibility between laboratories, and cross-reactions were found in some cases[37,102].
Ballardini et al[103] first applied IHC for different HCV antigens (c100, c33, c22, NS5) in HCV-positive OLT recipients, and showed that IHC positivity appeared in hepatocyte cytoplasm “in almost all livers at day 20 post-OLT”[104]. Among the cases with acute lobular hepatitis, a median of 80% of positive hepatocytes was found, while in all other cases the percentage positivity was never greater than 30%[103]. The authors concluded that IHC might be used to support the diagnosis of recurrent hepatitis C when histology alone was not conclusive[104]. Studies from our group confirmed a strong correlation between IHC positivity in hepatocyte cytoplasm and intrahepatic viral load with RT-PCR[23,105]. IHC detection of HCV was associated with the typical histopathological features of hepatitis C (hepatocyte single-cell necrosis, bile duct damage, cholestasis, lymphoid aggregate) in a single study[106], while in another paper post-OLT IHC positivity for anti-HCV core proteins correlated with IHC positivity in explanted livers and with the development of a cholestatic recurrent hepatitis C[107]. Finally, a recent work with a monoclonal antibodies against HCV-envelope 2 found a stronger positivity in definite or probable recurrent hepatitis C than in other conditions (including ACR)[108]; this IHC positivity did not correlate with HCV RNA serum levels.
Hepatic stellate cell activation
IHC has been used in the investigation of some features which can indirectly be related to recurrent hepatitis C diagnosis and progression. Some papers of the same period applied IHC for α smooth muscle actin (α-SMA) in order to detect activated mesenchymal hepatic stellate cells (HSC) in the portal tracts and fibrous septa in OLT specimens from HCV-positive recipients[109-111]. The amount of α-SMA-positive cells were predictive of recurrent hepatitis C with high histological activity, leading to an HSC-mediated rapid fibrosis[110], regardless of the amount of collagen deposition measured by the trichrome stain[111]. For the study of HSC activation in recurrent hepatitis C, glial fibrillary acid protein has also been proposed and compared with α-SMA[112].
Meriden et al[52] have studied keratin 19 (K19) in bile duct proliferation and the expression of vimentin in HSC, portal mesenchymal cells and some biliary epithelial cells, with an increased expression of both markers in those patients with faster fibrosis progression, independently of the amount of collagen deposition as measured by Sirius Red. Early activation of HSC preceding collagen deposition was also described and, together with bile duct proliferation, was determined to play a role in fibrosis progression.
Other applications of immunohistochemistry
Claudin-1 protein is a tight junction protein expressed mainly on the apical-canalicular site of hepatocytes, and represents one of the most important HCV receptors. A recent study by Zadori et al[113] on 12 HCV-positive allografts found that cases with low apical Claudin-1 IHC expression at 1 year after OLT had a better response to antiviral therapy. Moreover, a correlation between Claudin-1 and the degree of fibrosis was found.
As far as the differential diagnosis between recurrent hepatitis C and ACR is concerned, some markers have been proposed. The utility of IHC for C4d is still debated: some preliminary analyses reported that C4d tissue positivity, detected by means of IHC or immunofluorescence, was markedly higher in rejection cases than in recurrent hepatitis C[114-116]. However, a more recent study found C4d positivity in 17.6% of ACR biopsies vs 25.9% of recurrent hepatitis C[117]. These results illustrate the controversial use of C4d for routine diagnosis.
MacQuillan et al[118] studied the expression of MxA protein, a GTPase involved in interferon pathway activation, on 14 HCV-positive OLT patients, and found higher MxA expression in hepatocytes and monocytes of recurrent hepatitis C cases. These results are in contrast with Borgogna et al[119], who found a positive correlation between MxA expression and ACR, although they also observed a lower rate of fibrosis progression in patients with recurrent hepatitis C and concomitant strong MxA expression. These studies included cases with HCV-ACR overlap and cases treated with steroid boluses, which were likely to further confuse the scenario, and according to the same authors, validations on wider series are required.
The IHC evaluation of the cell-cycle marker minichromosome maintenance protein-2 (Mcm-2) was also proposed in the literature: a single study found up to 24% of Mcm-2 positive hepatocytes in recipients who later developed fibrosis, vs 5% of patients without fibrosis[120]. Moreover, the portal tracts in ACR biopsies were reported to show more Mcm-2-positive lymphocytes, than in recurrent hepatitis C biopsies[121].
ANCILLARY TECHNIQUES: RT-PCR
HCV RNA quantitation in liver tissue
The first study of tissue HCV RNA quantitation was carried by Di Martino et al[122] on 84 biopsies from 33 HCV-positive recipients and HCV RNA was markedly higher in biopsies of HCV recurrence with lobular hepatitis, regardless of the occurrence of genotype 1b. Moreover, tissue HCV RNA seemed to decrease in the transition from lobular (acute) hepatitis to chronic hepatitis C, probably due to the host’s response against HCV in the long term. Finally, an interesting positive correlation between the levels of HCV RNA at the first pre-transplant biopsy and the risk of chronization was found[122]. In the same year, Cirocco et al[90] confirmed on a series of 23 biopsies that tissue HCV RNA was significantly higher in recurrent hepatitis C cases than in other allograft conditions: moreover, the same authors confirmed these data using in situ RT-PCR on 25 recipients[123]. According to Aardema et al[124], who studied four sequential protocol biopsies in 26 recipients, intrahepatic HCV RNA was directly related to the degree of lobular hepatitis, but not to serum HCV. A semi-quantitative analysis of the HCV intermediate RNA filament, a marker of viral replication, showed that HCV started replicating very early after OLT: interestingly, this replication correlated with the other viral antigens, but neither with histological hepatic damage nor with serum HCV[125]. A further semi-quantitative PCR analysis on non-protocol biopsies showed that intrahepatic HCV RNA correlated with Fas mRNA and DNA fragmentation, which represent important indexes of liver cells apoptosis[28].
Gottschlich et al[91] confirmed in 2001 the usefulness of tissue HCV RNA quantitation in the differential diagnosis between recurrent hepatitis C and ACR, on 72 biopsies from a series of 36 OLT recipients. After stratifying the recipients into different histopathological groups, i.e., recurrent hepatitis C (probable and definite), indeterminate, and ACR (probable and definite), they noticed significantly higher HCV RNA levels in the HCV groups, even if the “probable rejection” group had high levels as well. The authors hypothesized that ACR episodes might be able to increase viral replication or, more likely, that recurrent hepatitis C and ACR can coexist, with hepatitis C as the predominant process. The conclusions were that recipients with low intrahepatic HCV RNA were not likely to have recurrent hepatitis C, although high HCV RNA did not exclude ACR[91].
Starting from these assumptions, in 2008 our group carried out RT-PCR quantitation of non-scheduled biopsies from 65 consecutive HCV recipients: in this work we confirmed that intrahepatic HCV RNA correlated with IHC positivity for viral antigens and Councilman bodies (C/P ratio, see above), and we described a 73% sensitivity and 85% specificity for RT-PCR in discriminating recurrent hepatitis C from other conditions, assuming a cut-off value of 1.1 IU/ng[23]. One year later, in a methodological study on 215 biopsies, we described the correlation between intrahepatic HCV RNA and IHC, serum HCV RNA, and the main liver serum markers[105]. Finally, we recently proposed that the quantitation of HCV RNA on the “first biopsy”, together with the serum HCV RNA, might have a prognostic impact. Indeed, on the basis of tissue and serum HCV RNA loads, we stratified 83 HCV recipients into three categories: (1) tissue HCV RNA ≤ 1.5 IU/ng with any serum HCV RNA (68% recurrence rate and 0% HCV-related mortality); (2) tissue HCV RNA > 1.5 IU/ng and serum HCV RNA < 4 × 107 copies/mL (91% recurrence rate and 14% mortality); and (3) tissue HCV RNA > 1.5 IU/ng and serum HCV RNA ≥ 4 × 107 copies/mL (100% recurrence rate and 45% HCV-related mortality). Moreover, we lowered the diagnostic cut-off value to 0.85 IU/ng, with 89% sensitivity and 71% specificity[22]. Prospective studies on larger series are required in order to confirm the true prognostic value of HCV RNA quantitation, and it is our opinion (together with Gottschlich)[91] that RT-PCR alone can be misleading, and it must always be interpreted in the context of the overall clinical and morphological background.
Interleukin-28B polymorphism
Apart from the quantitation of serum and intrahepatic viral load, RT-PCR technology has recently also been applied in the study of recipient genetic variability, such as the case of interleukin 28B (IL-28B), or type-III interferon, whose polymorphism has been correlated with the response to antiviral therapy, or even spontaneous viral clearance, in hepatitis C[126]. As for the OLT setting, in an intriguing case report of a recipient engrafted with two liver lobes from two different living donors, different stages of fibrosis and different tissue HCV RNA were found in the two grafts after 2 years; the authors attributed this diversity to the IL-28B genetic variants in the two grafts[127]. In recent studies, different rates of sustained virological response to therapy were reported according to the presence or absence of “favorable” IL-28B genotypes (C/C and/or T/T genotype, according to the different studies) both in donor and recipient livers[128-132]. Moreover, recipient IL-28B “non-C/C genotype” was an independent risk factor for cholestatic recurrent hepatitis C[133]. As underlined by Fabris et al[134] in non-transplanted HCV patients, and also in OLT recipients, the decision about antiviral therapy is driven by clinical indications, such as transaminases level and HCV genotype, and nowadays donor/recipient genotyping still does not help the clinician in the decision. However, we guess that the application of these technical procedures on donor and recipient tissue will represent a valid aid for the pathologist (and the clinician) for the routine management of HCV-positive recipients in the future.
Other cytokines analyzed by RT-PCR in the post-OLT HCV setting are IL-2 and IL-4: in a series of 52 OLT recipients and 22 non-transplanted patients, Dharancy et al[135] found that IL-4 expression was high in severe hepatitis recurrence C cases, and lower in mild HCV infection and HCV-negative cases; IL-4 expression was confirmed in tissue by means of IHC.
Nowadays, molecular techniques such as microarrays have been validated for use in the differential diagnosis between recurrent hepatitis C and ACR[136]; this issue is not discussed in the present review.
CONCLUSION
Although the morphological features of recurrent hepatitis C have been well described in the last few decades, differential diagnosis can still represent a challenge for pathologists, especially in the setting of early recurrent hepatitis C and mild ACR. In addition to the clinical data, essential for the exclusion of other pathological conditions, many ancillary techniques have been proposed, and are mainly based on IHC. Very few of these techniques have been used routinely, and nowadays HCV RNA quantitation by means of RT-PCR has largely replaced IHC for HCV in most laboratories. Indeed, albeit more expensive, RT-PCR is by far more sensitive and specific than IHC, and can be of great help in the early post-OLT management of recipients, even if RT-PCR itself is likely to be replaced in the future by some new technologies (not included in the present review). An open question is whether RT-PCR might be useful in the long post-OLT term, i.e., if HCV RNA intrahepatic viral load after 1 year or more might have a prognostic meaning, for example in predicting fibrosis progression, or if other factors prevail, such as the host immune system, HSC activation, etc. Future prospective studies with an adequate follow-up are surely required. Protocol biopsies represent another important issue: without doubt they are very useful in the study of allograft disease progression, but they are not free from complications and might not be accepted by patients. It is likely that each transplant team will formulate its policy for post-transplant biopsies in the future, since arguments exist both in support of and against protocol biopsies.
There is no doubt that protocol biopsies will be indispensable in answering other open questions, such as the significance of plasma cell infiltrate in HCV-positive allografts, the real prognostic weight of HCV-induced graft steatosis, and the impact of donor age and graft characteristics in recurrent hepatitis C.
Footnotes
P- Reviewers: Gruttadauria S, Hanazaki K, Pan JJ S- Editor: Gou SX L- Editor: Cant MR E- Editor: Ma S
References
- 1.Terrault N. Liver transplantation in the setting of chronic HCV. Best Pract Res Clin Gastroenterol. 2012;26:531–548. doi: 10.1016/j.bpg.2012.09.010. [DOI] [PubMed] [Google Scholar]
- 2.Belli LS, Alberti A, Rondinara GF, de Carlis L, Romani F, Ideo G, Belli L. Recurrent HCV hepatitis after liver transplantation. Lancet. 1993;341:378. doi: 10.1016/0140-6736(93)90188-m. [DOI] [PubMed] [Google Scholar]
- 3.Shiffman ML, Contos MJ, Luketic VA, Sanyal AJ, Purdum PP, Mills AS, Fisher RA, Posner MP. Biochemical and histologic evaluation of recurrent hepatitis C following orthotopic liver transplantation. Transplantation. 1994;57:526–532. [PubMed] [Google Scholar]
- 4.Greenson JK, Svoboda-Newman SM, Merion RM, Frank TS. Histologic progression of recurrent hepatitis C in liver transplant allografts. Am J Surg Pathol. 1996;20:731–738. doi: 10.1097/00000478-199606000-00011. [DOI] [PubMed] [Google Scholar]
- 5.Gane EJ, Portmann BC, Naoumov NV, Smith HM, Underhill JA, Donaldson PT, Maertens G, Williams R. Long-term outcome of hepatitis C infection after liver transplantation. N Engl J Med. 1996;334:815–820. doi: 10.1056/NEJM199603283341302. [DOI] [PubMed] [Google Scholar]
- 6.Schluger LK, Sheiner PA, Thung SN, Lau JY, Min A, Wolf DC, Fiel I, Zhang D, Gerber MA, Miller CM, et al. Severe recurrent cholestatic hepatitis C following orthotopic liver transplantation. Hepatology. 1996;23:971–976. doi: 10.1002/hep.510230505. [DOI] [PubMed] [Google Scholar]
- 7.Guerrero RB, Batts KP, Burgart LJ, Barrett SL, Germer JJ, Poterucha JJ, Wiesner RH, Charlton MR, Persing DH. Early detection of hepatitis C allograft reinfection after orthotopic liver transplantation: a molecular and histologic study. Mod Pathol. 2000;13:229–237. doi: 10.1038/modpathol.3880043. [DOI] [PubMed] [Google Scholar]
- 8.McCaughan GW, Zekry A. Pathogenesis of hepatitis C virus recurrence in the liver allograft. Liver Transpl. 2002;8:S7–S13. doi: 10.1053/jlts.2002.35856. [DOI] [PubMed] [Google Scholar]
- 9.Garcia-Retortillo M, Forns X, Feliu A, Moitinho E, Costa J, Navasa M, Rimola A, Rodes J. Hepatitis C virus kinetics during and immediately after liver transplantation. Hepatology. 2002;35:680–687. doi: 10.1053/jhep.2002.31773. [DOI] [PubMed] [Google Scholar]
- 10.Guo L, Orrego M, Rodriguez-Luna H, Balan V, Byrne T, Chopra K, Douglas DD, Harrison E, Moss A, Reddy KS, et al. Living donor liver transplantation for hepatitis C-related cirrhosis: no difference in histological recurrence when compared to deceased donor liver transplantation recipients. Liver Transpl. 2006;12:560–565. doi: 10.1002/lt.20660. [DOI] [PubMed] [Google Scholar]
- 11.Khettry U, Huang WY, Simpson MA, Pomfret EA, Pomposelli JJ, Lewis WD, Jenkins RL, Gordon FD. Patterns of recurrent hepatitis C after liver transplantation in a recent cohort of patients. Hum Pathol. 2007;38:443–452. doi: 10.1016/j.humpath.2006.08.028. [DOI] [PubMed] [Google Scholar]
- 12.Demetris AJ. Evolution of hepatitis C virus in liver allografts. Liver Transpl. 2009;15 Suppl 2:S35–S41. doi: 10.1002/lt.21890. [DOI] [PubMed] [Google Scholar]
- 13.Pacholczyk M, Łągiewska B, Lisik W, Tronina O, Wasiak D, Cieciura T, Chmura A. Liver transplantation for HCV cirrhosis; cautious optimism after 10 years of experience. Ann Transplant. 2012;17:5–10. doi: 10.12659/aot.883688. [DOI] [PubMed] [Google Scholar]
- 14.Wright TL, Donegan E, Hsu HH, Ferrell L, Lake JR, Kim M, Combs C, Fennessy S, Roberts JP, Ascher NL. Recurrent and acquired hepatitis C viral infection in liver transplant recipients. Gastroenterology. 1992;103:317–322. doi: 10.1016/0016-5085(92)91129-r. [DOI] [PubMed] [Google Scholar]
- 15.Randhawa PS, Demetris AJ. Hepatitis C virus infection in liver allografts. Pathol Annu. 1995;30 Pt 2:203–226. [PubMed] [Google Scholar]
- 16.Gallegos-Orozco JF, Yosephy A, Noble B, Aqel BA, Byrne TJ, Carey EJ, Douglas DD, Mulligan D, Moss A, de Petris G, et al. Natural history of post-liver transplantation hepatitis C: A review of factors that may influence its course. Liver Transpl. 2009;15:1872–1881. doi: 10.1002/lt.21954. [DOI] [PubMed] [Google Scholar]
- 17.Shuhart MC, Bronner MP, Gretch DR, Thomassen LV, Wartelle CF, Tateyama H, Emerson SS, Perkins JD, Carithers RL. Histological and clinical outcome after liver transplantation for hepatitis C. Hepatology. 1997;26:1646–1652. doi: 10.1002/hep.510260638. [DOI] [PubMed] [Google Scholar]
- 18.Prieto M, Berenguer M, Rayón JM, Córdoba J, Argüello L, Carrasco D, García-Herola A, Olaso V, De Juan M, Gobernado M, et al. High incidence of allograft cirrhosis in hepatitis C virus genotype 1b infection following transplantation: relationship with rejection episodes. Hepatology. 1999;29:250–256. doi: 10.1002/hep.510290122. [DOI] [PubMed] [Google Scholar]
- 19.Sugo H, Balderson GA, Crawford DH, Fawcett J, Lynch SV, Strong RW, Futagawa S. The influence of viral genotypes and rejection episodes on the recurrence of hepatitis C after liver transplantation. Surg Today. 2003;33:421–425. doi: 10.1007/s10595-002-2537-5. [DOI] [PubMed] [Google Scholar]
- 20.Germani G, Tsochatzis E, Papastergiou V, Burroughs AK. HCV in liver transplantation. Semin Immunopathol. 2013;35:101–110. doi: 10.1007/s00281-012-0329-5. [DOI] [PubMed] [Google Scholar]
- 21.Mells G, Neuberger J. Protocol liver allograft biopsies. Transplantation. 2008;85:1686–1692. doi: 10.1097/TP.0b013e318176b1fd. [DOI] [PubMed] [Google Scholar]
- 22.Vasuri F, Morelli MC, Gruppioni E, Fiorentino M, Ercolani G, Cescon M, Pinna AD, Grigioni WF, D’Errico-Grigioni A. The meaning of tissue and serum HCV RNA quantitation in hepatitis C recurrence after liver transplantation: a retrospective study. Dig Liver Dis. 2013;45:505–509. doi: 10.1016/j.dld.2012.11.015. [DOI] [PubMed] [Google Scholar]
- 23.D’Errico-Grigioni A, Fiorentino M, Vasuri F, Gruppioni E, Fabbrizio B, Zucchini N, Ballardini G, Morelli C, Pinna AD, Grigioni WF. Tissue hepatitis C virus RNA quantification and protein expression help identify early hepatitis C virus recurrence after liver transplantation. Liver Transpl. 2008;14:313–320. doi: 10.1002/lt.21375. [DOI] [PubMed] [Google Scholar]
- 24.Saraf N, Fiel MI, Deboccardo G, Emre S, Schiano TD. Rapidly progressive recurrent hepatitis C virus infection starting 9 days after liver transplantation. Liver Transpl. 2007;13:913–917. doi: 10.1002/lt.21188. [DOI] [PubMed] [Google Scholar]
- 25.Park YN, Boros P, Zhang DY, Sheiner P, Kim-Schluger L, Thung SN. Serum hepatitis C virus RNA levels and histologic findings in liver allografts with early recurrent hepatitis C. Arch Pathol Lab Med. 2000;124:1623–1627. doi: 10.5858/2000-124-1623-SHCVRL. [DOI] [PubMed] [Google Scholar]
- 26.Demetris AJ, Eghtesad B, Marcos A, Ruppert K, Nalesnik MA, Randhawa P, Wu T, Krasinskas A, Fontes P, Cacciarelli T, et al. Recurrent hepatitis C in liver allografts: prospective assessment of diagnostic accuracy, identification of pitfalls, and observations about pathogenesis. Am J Surg Pathol. 2004;28:658–669. doi: 10.1097/00000478-200405000-00015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Crespo J, Rivero M, Mayorga M, Fabrega E, Casafont F, Gomez-Fleitas M, Pons-Romero F. Involvement of the fas system in hepatitis C virus recurrence after liver transplantation. Liver Transpl. 2000;6:562–569. doi: 10.1053/jlts.2000.9742. [DOI] [PubMed] [Google Scholar]
- 28.Di Martino V, Brenot C, Samuel D, Saurini F, Paradis V, Reynés M, Bismuth H, Féray C. Influence of liver hepatitis C virus RNA and hepatitis C virus genotype on FAS-mediated apoptosis after liver transplantation for hepatitis C. Transplantation. 2000;70:1390–1396. doi: 10.1097/00007890-200011150-00021. [DOI] [PubMed] [Google Scholar]
- 29.Lim EJ, Chin R, Angus PW, Torresi J. Enhanced apoptosis in post-liver transplant hepatitis C: effects of virus and immunosuppressants. World J Gastroenterol. 2012;18:2172–2179. doi: 10.3748/wjg.v18.i18.2172. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Saxena R, Crawford JM, Navarro VJ, Friedman AL, Robert ME. Utilization of acidophil bodies in the diagnosis of recurrent hepatitis C infection after orthotopic liver transplantation. Mod Pathol. 2002;15:897–903. doi: 10.1038/modpathol.3880626. [DOI] [PubMed] [Google Scholar]
- 31.Davies SE, Portmann BC, O’Grady JG, Aldis PM, Chaggar K, Alexander GJ, Williams R. Hepatic histological findings after transplantation for chronic hepatitis B virus infection, including a unique pattern of fibrosing cholestatic hepatitis. Hepatology. 1991;13:150–157. [PubMed] [Google Scholar]
- 32.Narang TK, Ahrens W, Russo MW. Post-liver transplant cholestatic hepatitis C: a systematic review of clinical and pathological findings and application of consensus criteria. Liver Transpl. 2010;16:1228–1235. doi: 10.1002/lt.22175. [DOI] [PubMed] [Google Scholar]
- 33.Taga SA, Washington MK, Terrault N, Wright TL, Somberg KA, Ferrell LD. Cholestatic hepatitis C in liver allografts. Liver Transpl Surg. 1998;4:304–310. doi: 10.1002/lt.500040401. [DOI] [PubMed] [Google Scholar]
- 34.Dixon LR, Crawford JM. Early histologic changes in fibrosing cholestatic hepatitis C. Liver Transpl. 2007;13:219–226. doi: 10.1002/lt.21011. [DOI] [PubMed] [Google Scholar]
- 35.Verna EC, Abdelmessih R, Salomao MA, Lefkowitch J, Moreira RK, Brown RS. Cholestatic hepatitis C following liver transplantation: an outcome-based histological definition, clinical predictors, and prognosis. Liver Transpl. 2013;19:78–88. doi: 10.1002/lt.23559. [DOI] [PubMed] [Google Scholar]
- 36.McCaughan GW, Zekry A. Mechanisms of HCV reinfection and allograft damage after liver transplantation. J Hepatol. 2004;40:368–374. doi: 10.1016/j.jhep.2004.01.014. [DOI] [PubMed] [Google Scholar]
- 37.Doughty AL, Painter DM, McCaughan GW. Nonspecificity of monoclonal antibody Tordji-22 for the detection of hepatitis C virus in liver transplant recipients with cholestatic hepatitis. Liver Transpl Surg. 1999;5:40–45. doi: 10.1002/lt.500050104. [DOI] [PubMed] [Google Scholar]
- 38.Deshpande V, Burd E, Aardema KL, Ma CK, Moonka DK, Brown KA, Abouljoud MS, Nakhleh RE. High levels of hepatitis C virus RNA in native livers correlate with the development of cholestatic hepatitis in liver allografts and a poor outcome. Liver Transpl. 2001;7:118–124. doi: 10.1053/jlts.2001.21278. [DOI] [PubMed] [Google Scholar]
- 39.Fiel MI, Agarwal K, Stanca C, Elhajj N, Kontorinis N, Thung SN, Schiano TD. Posttransplant plasma cell hepatitis (de novo autoimmune hepatitis) is a variant of rejection and may lead to a negative outcome in patients with hepatitis C virus. Liver Transpl. 2008;14:861–871. doi: 10.1002/lt.21447. [DOI] [PubMed] [Google Scholar]
- 40.Kontorinis N, Agarwal K, Elhajj N, Fiel MI, Schiano TD. Pegylated interferon-induced immune-mediated hepatitis post-liver transplantation. Liver Transpl. 2006;12:827–830. doi: 10.1002/lt.20706. [DOI] [PubMed] [Google Scholar]
- 41.Berardi S, Lodato F, Gramenzi A, D’Errico A, Lenzi M, Bontadini A, Morelli MC, Tamè MR, Piscaglia F, Biselli M, et al. High incidence of allograft dysfunction in liver transplanted patients treated with pegylated-interferon alpha-2b and ribavirin for hepatitis C recurrence: possible de novo autoimmune hepatitis? Gut. 2007;56:237–242. doi: 10.1136/gut.2006.092064. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Selzner N, Guindi M, Renner EL, Berenguer M. Immune-mediated complications of the graft in interferon-treated hepatitis C positive liver transplant recipients. J Hepatol. 2011;55:207–217. doi: 10.1016/j.jhep.2010.11.012. [DOI] [PubMed] [Google Scholar]
- 43.Levitsky J, Fiel MI, Norvell JP, Wang E, Watt KD, Curry MP, Tewani S, McCashland TM, Hoteit MA, Shaked A, et al. Risk for immune-mediated graft dysfunction in liver transplant recipients with recurrent HCV infection treated with pegylated interferon. Gastroenterology. 2012;142:1132–1139.e1. doi: 10.1053/j.gastro.2012.01.030. [DOI] [PubMed] [Google Scholar]
- 44.Ward SC, Schiano TD, Thung SN, Fiel MI. Plasma cell hepatitis in hepatitis C virus patients post-liver transplantation: case-control study showing poor outcome and predictive features in the liver explant. Liver Transpl. 2009;15:1826–1833. doi: 10.1002/lt.21949. [DOI] [PubMed] [Google Scholar]
- 45.Demetris AJ, Sebagh M. Plasma cell hepatitis in liver allografts: Variant of rejection or autoimmune hepatitis? Liver Transpl. 2008;14:750–755. doi: 10.1002/lt.21518. [DOI] [PubMed] [Google Scholar]
- 46.Bárcena R, Sanromán AL, Del Campo S, García M, Moreno A, De Vicente E, Candela A. Posttransplant liver granulomatosis associated with hepatitis C? Transplantation. 1998;65:1494–1495. doi: 10.1097/00007890-199806150-00015. [DOI] [PubMed] [Google Scholar]
- 47.Ferrell LD, Lee R, Brixko C, Bass NM, Lake JR, Roberts JP, Ascher N, Rabkin J. Hepatic granulomas following liver transplantation. Clinicopathologic features in 42 patients. Transplantation. 1995;60:926–933. [PubMed] [Google Scholar]
- 48.Vakiani E, Hunt KK, Mazziotta RM, Emond JC, Brown RS, Lefkowitch JH, Bhagat G. Hepatitis C-associated granulomas after liver transplantation: morphologic spectrum and clinical implications. Am J Clin Pathol. 2007;127:128–134. doi: 10.1309/NN03WMD8V0GK6HFW. [DOI] [PubMed] [Google Scholar]
- 49.Fiel MI, Shukla D, Saraf N, Xu R, Schiano TD. Development of hepatic granulomas in patients receiving pegylated interferon therapy for recurrent hepatitis C virus post liver transplantation. Transpl Infect Dis. 2008;10:184–189. doi: 10.1111/j.1399-3062.2007.00258.x. [DOI] [PubMed] [Google Scholar]
- 50.Brandman D, Pingitore A, Lai JC, Roberts JP, Ferrell L, Bass NM, Terrault NA. Hepatic steatosis at 1 year is an additional predictor of subsequent fibrosis severity in liver transplant recipients with recurrent hepatitis C virus. Liver Transpl. 2011;17:1380–1386. doi: 10.1002/lt.22389. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Subramanian V, Seetharam AB, Vachharajani N, Tiriveedhi V, Angaswamy N, Ramachandran S, Crippin JS, Shenoy S, Chapman WC, Mohanakumar T, et al. Donor graft steatosis influences immunity to hepatitis C virus and allograft outcome after liver transplantation. Transplantation. 2011;92:1259–1268. doi: 10.1097/TP.0b013e318235a1ab. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Meriden Z, Forde KA, Pasha TL, Hui JJ, Reddy KR, Furth EE, Wells RG. Histologic predictors of fibrosis progression in liver allografts in patients with hepatitis C virus infection. Clin Gastroenterol Hepatol. 2010;8:289–296, 296.e1-8. doi: 10.1016/j.cgh.2009.10.034. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Rosen HR, Gretch DR, Oehlke M, Flora KD, Benner KG, Rabkin JM, Corless CL. Timing and severity of initial hepatitis C recurrence as predictors of long-term liver allograft injury. Transplantation. 1998;65:1178–1182. doi: 10.1097/00007890-199805150-00006. [DOI] [PubMed] [Google Scholar]
- 54.Moreira RK, Salomao M, Verna EC, Brown RS, Lefkowitch JH. The Hepatitis Aggressiveness Score (HAS): a novel classification system for post-liver transplantation recurrent hepatitis C. Am J Surg Pathol. 2013;37:104–113. doi: 10.1097/PAS.0b013e31826a92ac. [DOI] [PubMed] [Google Scholar]
- 55.Fujita S, Fujikawa T, Mizuno S, Reed AI, Kim RD, Howard RJ, Firpi RJ, Nelson DR, Hemming AW. Is early recurrence of hepatitis C associated with biliary anastomotic stricture after liver transplantation? Transplantation. 2007;84:1631–1635. doi: 10.1097/01.tp.0000295983.55088.96. [DOI] [PubMed] [Google Scholar]
- 56.Guzman G, Chennuri R, Voros A, Boumendjel R, Locante A, Patel R, Valyi-Nagy T. Nucleometric study of anisonucleosis, diabetes and oxidative damage in liver biopsies of orthotopic liver transplant recipients with chronic hepatitis C virus infection. Pathol Oncol Res. 2011;17:191–199. doi: 10.1007/s12253-010-9296-0. [DOI] [PubMed] [Google Scholar]
- 57.Guido M, Fagiuoli S, Tessari G, Burra P, Leandro G, Boccagni P, Cillo U, Naccarato R, Rugge M. Histology predicts cirrhotic evolution of post transplant hepatitis C. Gut. 2002;50:697–700. doi: 10.1136/gut.50.5.697. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Roche B, Sebagh M, Canfora ML, Antonini T, Roque-Afonso AM, Delvart V, Saliba F, Duclos-Vallee JC, Castaing D, Samuel D. Hepatitis C virus therapy in liver transplant recipients: response predictors, effect on fibrosis progression, and importance of the initial stage of fibrosis. Liver Transpl. 2008;14:1766–1777. doi: 10.1002/lt.21635. [DOI] [PubMed] [Google Scholar]
- 59.McKenna GJ, Trotter JF, Klintmalm E, Onaca N, Ruiz R, Jennings LW, Neri M, O’Leary JG, Davis GL, Levy MF, et al. Limiting hepatitis C virus progression in liver transplant recipients using sirolimus-based immunosuppression. Am J Transplant. 2011;11:2379–2387. doi: 10.1111/j.1600-6143.2011.03767.x. [DOI] [PubMed] [Google Scholar]
- 60.Calvaruso V, Dhillon AP, Tsochatzis E, Manousou P, Grillo F, Germani G, Patch D, O’Beirne J, Burroughs AK. Liver collagen proportionate area predicts decompensation in patients with recurrent hepatitis C virus cirrhosis after liver transplantation. J Gastroenterol Hepatol. 2012;27:1227–1232. doi: 10.1111/j.1440-1746.2012.07136.x. [DOI] [PubMed] [Google Scholar]
- 61.Berenguer M, Aguilera V, Prieto M, Carrasco D, Rayón M, San Juan F, Landaverde C, Mir J, Berenguer J. Delayed onset of severe hepatitis C-related liver damage following liver transplantation: a matter of concern? Liver Transpl. 2003;9:1152–1158. doi: 10.1053/jlts.2003.50240. [DOI] [PubMed] [Google Scholar]
- 62.Berenguer M, Rayón JM, Prieto M, Aguilera V, Nicolás D, Ortiz V, Carrasco D, López-Andujar R, Mir J, Berenguer J. Are posttransplantation protocol liver biopsies useful in the long term? Liver Transpl. 2001;7:790–796. doi: 10.1053/jlts.2001.23794. [DOI] [PubMed] [Google Scholar]
- 63.Sebagh M, Rifai K, Féray C, Yilmaz F, Falissard B, Roche B, Bismuth H, Samuel D, Reynès M. All liver recipients benefit from the protocol 10-year liver biopsies. Hepatology. 2003;37:1293–1301. doi: 10.1053/jhep.2003.50231. [DOI] [PubMed] [Google Scholar]
- 64.Sreekumar R, Gonzalez-Koch A, Maor-Kendler Y, Batts K, Moreno-Luna L, Poterucha J, Burgart L, Wiesner R, Kremers W, Rosen C, et al. Early identification of recipients with progressive histologic recurrence of hepatitis C after liver transplantation. Hepatology. 2000;32:1125–1130. doi: 10.1053/jhep.2000.19340. [DOI] [PubMed] [Google Scholar]
- 65.Samonakis DN, Triantos CK, Thalheimer U, Quaglia A, Leandro G, Teixeira R, Papatheodoridis GV, Sabin CA, Rolando N, Davies S, et al. Immunosuppression and donor age with respect to severity of HCV recurrence after liver transplantation. Liver Transpl. 2005;11:386–395. doi: 10.1002/lt.20344. [DOI] [PubMed] [Google Scholar]
- 66.Firpi RJ, Abdelmalek MF, Soldevila-Pico C, Cabrera R, Shuster JJ, Theriaque D, Reed AI, Hemming AW, Liu C, Crawford JM, et al. One-year protocol liver biopsy can stratify fibrosis progression in liver transplant recipients with recurrent hepatitis C infection. Liver Transpl. 2004;10:1240–1247. doi: 10.1002/lt.20238. [DOI] [PubMed] [Google Scholar]
- 67.Baiocchi L, Angelico M, Petrolati A, Perrone L, Palmieri G, Battista S, Carbone M, Tariciotti L, Longhi C, Orlando G, et al. Correlation between liver fibrosis and inflammation in patients transplanted for HCV liver disease. Am J Transplant. 2008;8:673–678. doi: 10.1111/j.1600-6143.2007.02107.x. [DOI] [PubMed] [Google Scholar]
- 68.Ghabril M, Dickson RC, Krishna M, Machicao V, Aranda-Michel J, Bonatti H, Nguyen JH. Explanted liver inflammatory grade predicts fibrosis progression in hepatitis C recurrence. Liver Transpl. 2011;17:685–694. doi: 10.1002/lt.22250. [DOI] [PubMed] [Google Scholar]
- 69.Neumann UP, Berg T, Bahra M, Seehofer D, Langrehr JM, Neuhaus R, Radke C, Neuhaus P. Fibrosis progression after liver transplantation in patients with recurrent hepatitis C. J Hepatol. 2004;41:830–836. doi: 10.1016/j.jhep.2004.06.029. [DOI] [PubMed] [Google Scholar]
- 70.Foxton MR, Quaglia A, Muiesan P, Heneghan MA, Portmann B, Norris S, Heaton ND, O’Grady JG. The impact of diabetes mellitus on fibrosis progression in patients transplanted for hepatitis C. Am J Transplant. 2006;6:1922–1929. doi: 10.1111/j.1600-6143.2006.01408.x. [DOI] [PubMed] [Google Scholar]
- 71.Belli LS, Burroughs AK, Burra P, Alberti AB, Samonakis D, Cammà C, De Carlis L, Minola E, Quaglia A, Zavaglia C, et al. Liver transplantation for HCV cirrhosis: improved survival in recent years and increased severity of recurrent disease in female recipients: results of a long term retrospective study. Liver Transpl. 2007;13:733–740. doi: 10.1002/lt.21093. [DOI] [PubMed] [Google Scholar]
- 72.Rayhill SC, Wu YM, Katz DA, Voigt MD, Labrecque DR, Kirby PA, Mitros FA, Kalil RS, Miller RA, Stolpen AH, et al. Older donor livers show early severe histological activity, fibrosis, and graft failure after liver transplantation for hepatitis C. Transplantation. 2007;84:331–339. doi: 10.1097/01.tp.0000270313.31328.63. [DOI] [PubMed] [Google Scholar]
- 73.Tallón Aguilar L, Molina García D, Barrera Pulido L, Pareja Ciuró F, Suárez Artacho G, Alamo Martínez JM, Bernal Bellido C, García González I, Serrano Díaz-Canedo J, Gómez Bravo MA, et al. Influence of donor age on survival in liver transplantation due to hepatitis C virus. Transplant Proc. 2008;40:2968–2970. doi: 10.1016/j.transproceed.2008.08.105. [DOI] [PubMed] [Google Scholar]
- 74.Jain A, Singhal A, Kashyap R, Safadjou S, Ryan CK, Orloff MS. Comparative analysis of hepatitis C recurrence and fibrosis progression between deceased-donor and living-donor liver transplantation: 8-year longitudinal follow-up. Transplantation. 2011;92:453–460. doi: 10.1097/TP.0b013e3182259282. [DOI] [PubMed] [Google Scholar]
- 75.Yilmaz N, Shiffman ML, Stravitz RT, Sterling RK, Luketic VA, Sanyal AJ, Mills AS, Contos MJ, Coterell A, Maluf D, et al. A prospective evaluation of fibrosis progression in patients with recurrent hepatitis C virus following liver transplantation. Liver Transpl. 2007;13:975–983. doi: 10.1002/lt.21117. [DOI] [PubMed] [Google Scholar]
- 76.Lionetti R, Tisone G, Palmieri G, Almerighi C, Anselmo A, Tariciotti L, Lenci I, De Luca L, Monaco A, Angelico M. Maintenance ribavirin monotherapy delays fibrosis progression in liver transplant recipients with recurrent hepatitis C at high risk of progression. Dig Liver Dis. 2010;42:297–303. doi: 10.1016/j.dld.2009.08.008. [DOI] [PubMed] [Google Scholar]
- 77.Baiocchi L, Tisone G, Palmieri G, Rapicetta M, Pisani F, Orlando G, Casciani CU, Angelico M. Hepatic steatosis: a specific sign of hepatitis C reinfection after liver transplantation. Liver Transpl Surg. 1998;4:441–447. doi: 10.1002/lt.500040613. [DOI] [PubMed] [Google Scholar]
- 78.Gordon FD, Pomfret EA, Pomposelli JJ, Lewis WD, Jenkins RL, Khettry U. Severe steatosis as the initial histologic manifestation of recurrent hepatitis C genotype 3. Hum Pathol. 2004;35:636–638. doi: 10.1016/j.humpath.2004.01.014. [DOI] [PubMed] [Google Scholar]
- 79.Testino G, Sumberaz A, Leone S, Borro P. Recurrent hepatitis C and non-alcoholic fatty liver disease in transplanted patients: a review. Minerva Med. 2013;104:225–232. [PubMed] [Google Scholar]
- 80.Rubbia-Brandt L, Quadri R, Abid K, Giostra E, Malé PJ, Mentha G, Spahr L, Zarski JP, Borisch B, Hadengue A, et al. Hepatocyte steatosis is a cytopathic effect of hepatitis C virus genotype 3. J Hepatol. 2000;33:106–115. doi: 10.1016/s0168-8278(00)80166-x. [DOI] [PubMed] [Google Scholar]
- 81.Pelletier SJ, Iezzoni JC, Crabtree TD, Hahn YS, Sawyer RG, Pruett TL. Prediction of liver allograft fibrosis after transplantation for hepatitis C virus: persistent elevation of serum transaminase levels versus necroinflammatory activity. Liver Transpl. 2000;6:44–53. doi: 10.1002/lt.500060111. [DOI] [PubMed] [Google Scholar]
- 82.Hanouneh IA, Feldstein AE, McCullough AJ, Miller C, Aucejo F, Yerian L, Lopez R, Zein NN. The significance of metabolic syndrome in the setting of recurrent hepatitis C after liver transplantation. Liver Transpl. 2008;14:1287–1293. doi: 10.1002/lt.21524. [DOI] [PubMed] [Google Scholar]
- 83.Toniutto P, Fabris C, Avellini C, Minisini R, Bitetto D, Rossi E, Smirne C, Pirisi M. Excess body weight, liver steatosis, and early fibrosis progression due to hepatitis C recurrence after liver transplantation. World J Gastroenterol. 2005;11:5944–5950. doi: 10.3748/wjg.v11.i38.5944. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84.Mindikoglu AL, Regev A, Casanova-Romero PY, Bejarano PA, Martinez EJ, Tzakis AG, Schiff ER. The impact of nonalcoholic fatty liver disease and the metabolic syndrome on progression of fibrosis in patients with recurrent HCV after liver transplantation. Transplant Proc. 2006;38:1440–1444. doi: 10.1016/j.transproceed.2006.02.060. [DOI] [PubMed] [Google Scholar]
- 85.Regev A, Molina E, Moura R, Bejarano PA, Khaled A, Ruiz P, Arheart K, Berho M, Drachenberg CB, Mendez P, et al. Reliability of histopathologic assessment for the differentiation of recurrent hepatitis C from acute rejection after liver transplantation. Liver Transpl. 2004;10:1233–1239. doi: 10.1002/lt.20245. [DOI] [PubMed] [Google Scholar]
- 86.Petrovic LM, Villamil FG, Vierling JM, Makowka L, Geller SA. Comparison of histopathology in acute allograft rejection and recurrent hepatitis C infection after liver transplantation. Liver Transpl Surg. 1997;3:398–406. doi: 10.1002/lt.500030407. [DOI] [PubMed] [Google Scholar]
- 87.Petrovic LM. Early recurrence of hepatitis C virus infection after liver transplantation. Liver Transpl. 2006;12:S32–S37. doi: 10.1002/lt.20942. [DOI] [PubMed] [Google Scholar]
- 88.Yeh MM, Larson AM, Tung BY, Swanson PE, Upton MP. Endotheliitis in chronic viral hepatitis: a comparison with acute cellular rejection and non-alcoholic steatohepatitis. Am J Surg Pathol. 2006;30:727–733. doi: 10.1097/00000478-200606000-00008. [DOI] [PubMed] [Google Scholar]
- 89.Leung JY, Abraczinskas DR, Bhan AK, Terella AM, Pascual M, Cosimi AB, Chung RT. Recurrent allograft HCV presenting as acute cellular rejection: successful management with interferon and ribavirin alone. Clin Transplant. 2003;17:275–283. doi: 10.1034/j.1399-0012.2003.00049.x. [DOI] [PubMed] [Google Scholar]
- 90.Cirocco R, Fragulidis GP, Weppler D, Zucker K, Markou M, Zervos XA, Viciana A, Esquinazi V, Nery JR, Reddy KR, et al. Recurrent hepatitis C infection following orthotopic liver transplantation is predicted by posttransplant serum and hepatic allograft viral titers. Transplant Proc. 1997;29:2839–2840. doi: 10.1016/s0041-1345(97)00699-4. [DOI] [PubMed] [Google Scholar]
- 91.Gottschlich MJ, Aardema KL, Burd EM, Nakhleh RE, Brown KA, Abouljoud MS, Hirst K, Moonka DK. The use of hepatitis C viral RNA levels in liver tissue to distinguish rejection from recurrent hepatitis C. Liver Transpl. 2001;7:436–441. doi: 10.1053/jlts.2001.23909. [DOI] [PubMed] [Google Scholar]
- 92.Watt KD, Lyden ER, Gulizia JM, McCashland TM. Recurrent hepatitis C posttransplant: early preservation injury may predict poor outcome. Liver Transpl. 2006;12:134–139. doi: 10.1002/lt.20583. [DOI] [PubMed] [Google Scholar]
- 93.Xiao SY, Lu L, Wang HL. Fibrosing cholestatic hepatitis: clinicopathologic spectrum, diagnosis and pathogenesis. Int J Clin Exp Pathol. 2008;1:396–402. [PMC free article] [PubMed] [Google Scholar]
- 94.Satapathy SK, Sclair S, Fiel MI, Del Rio Martin J, Schiano T. Clinical characterization of patients developing histologically-proven fibrosing cholestatic hepatitis C post-liver transplantation. Hepatol Res. 2011;41:328–339. doi: 10.1111/j.1872-034X.2011.00781.x. [DOI] [PubMed] [Google Scholar]
- 95.Adeyi O, Fischer SE, Guindi M. Liver allograft pathology: approach to interpretation of needle biopsies with clinicopathological correlation. J Clin Pathol. 2010;63:47–74. doi: 10.1136/jcp.2009.068254. [DOI] [PubMed] [Google Scholar]
- 96.Teixeira R, Pastacaldi S, Davies S, Dhillon AP, Emery VC, Rolles K, Davidson B, Patch D, Burroughs AK. The influence of cytomegalovirus viraemia on the outcome of recurrent hepatitis C after liver transplantation. Transplantation. 2000;70:1454–1458. doi: 10.1097/00007890-200011270-00010. [DOI] [PubMed] [Google Scholar]
- 97.Blight K, Rowland R, Hall PD, Lesniewski RR, Trowbridge R, LaBrooy JT, Gowans EJ. Immunohistochemical detection of the NS4 antigen of hepatitis C virus and its relation to histopathology. Am J Pathol. 1993;143:1568–1573. [PMC free article] [PubMed] [Google Scholar]
- 98.González-Peralta RP, Fang JW, Davis GL, Gish RG, Kohara M, Mondelli MU, Urdea MS, Mizokami M, Lau JY. Significance of hepatic expression of hepatitis C viral antigens in chronic hepatitis C. Dig Dis Sci. 1995;40:2595–2601. doi: 10.1007/BF02220447. [DOI] [PubMed] [Google Scholar]
- 99.Vargas V, Krawczynski K, Castells L, Martinez N, Esteban J, Allende H, Esteban R, Guardia J. Recurrent hepatitis C virus infection after liver transplantation: immunohistochemical assessment of the viral antigen. Liver Transpl Surg. 1998;4:320–327. doi: 10.1002/lt.500040407. [DOI] [PubMed] [Google Scholar]
- 100.Brody RI, Eng S, Melamed J, Mizrachi H, Schneider RJ, Tobias H, Teperman LW, Theise ND. Immunohistochemical detection of hepatitis C antigen by monoclonal antibody TORDJI-22 compared with PCR viral detection. Am J Clin Pathol. 1998;110:32–37. doi: 10.1093/ajcp/110.1.32. [DOI] [PubMed] [Google Scholar]
- 101.Nayak NC, Sathar SA. Immunohistochemical detection of hepatitis C virus antigen in paraffin embedded liver biopsies from patients with chronic liver disease. Acta Histochem. 1999;101:409–419. doi: 10.1016/S0065-1281(99)80041-5. [DOI] [PubMed] [Google Scholar]
- 102.Fenwick F, Bassendine MF, Agarwal K, Bevitt D, Pumeechockchai W, Burt AD, Toms GL. Immunohistochemical assessment of hepatitis C virus antigen in cholestatic hepatitis after liver transplantation. J Clin Pathol. 2006;59:174–178. doi: 10.1136/jcp.2005.028126. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 103.Ballardini G, De Raffele E, Groff P, Bioulac-Sage P, Grassi A, Ghetti S, Susca M, Strazzabosco M, Bellusci R, Iemmolo RM, et al. Timing of reinfection and mechanisms of hepatocellular damage in transplanted hepatitis C virus-reinfected liver. Liver Transpl. 2002;8:10–20. doi: 10.1053/jlts.2002.30141. [DOI] [PubMed] [Google Scholar]
- 104.Grassi A, Quarneti C, Ravaioli M, Bianchini F, Susca M, D’Errico A, Piscaglia F, Tamè MR, Andreone P, Grazi G, et al. Detection of HCV antigens in liver graft: relevance to the management of recurrent post-liver transplant hepatitis C. Liver Transpl. 2006;12:1673–1681. doi: 10.1002/lt.20882. [DOI] [PubMed] [Google Scholar]
- 105.Gruppioni E, Vasuri F, Fiorentino M, Capizzi E, Altimari A, Pirini MG, Grazi GL, Malvi D, Grigioni WF, D’Errico-Grigioni A. Real-time quantitative assay for routine testing of HCV RNA in formalin-fixed, paraffin-embedded liver samples. Diagn Mol Pathol. 2009;18:232–238. doi: 10.1097/PDM.0b013e3181916e31. [DOI] [PubMed] [Google Scholar]
- 106.Nuovo GJ, Holly A, Wakely P, Frankel W. Correlation of histology, viral load, and in situ viral detection in hepatic biopsies from patients with liver transplants secondary to hepatitis C infection. Hum Pathol. 2002;33:277–284. doi: 10.1053/hupa.2002.32211. [DOI] [PubMed] [Google Scholar]
- 107.Pessôa MG, Alves VA, Wakamatsu A, Gomes JG, Maertens G, van der Borght B, Kim M, Ferrell L, Wright TL. Post-transplant recurrent hepatitis C: immunohistochemical detection of hepatitis C virus core antigen and possible pathogenic implications. Liver Int. 2008;28:807–813. doi: 10.1111/j.1478-3231.2008.01739.x. [DOI] [PubMed] [Google Scholar]
- 108.Sadamori H, Yagi T, Iwagaki H, Matsuda H, Shinoura S, Umeda Y, Ohara N, Yanai H, Ogino T, Tanaka N. Immunohistochemical staining of liver grafts with a monoclonal antibody against HCV-Envelope 2 for recurrent hepatitis C after living donor liver transplantation. J Gastroenterol Hepatol. 2009;24:574–580. doi: 10.1111/j.1440-1746.2008.05638.x. [DOI] [PubMed] [Google Scholar]
- 109.Carpino G, Morini S, Ginanni Corradini S, Franchitto A, Merli M, Siciliano M, Gentili F, Onetti Muda A, Berloco P, Rossi M, et al. Alpha-SMA expression in hepatic stellate cells and quantitative analysis of hepatic fibrosis in cirrhosis and in recurrent chronic hepatitis after liver transplantation. Dig Liver Dis. 2005;37:349–356. doi: 10.1016/j.dld.2004.11.009. [DOI] [PubMed] [Google Scholar]
- 110.Gawrieh S, Papouchado BG, Burgart LJ, Kobayashi S, Charlton MR, Gores GJ. Early hepatic stellate cell activation predicts severe hepatitis C recurrence after liver transplantation. Liver Transpl. 2005;11:1207–1213. doi: 10.1002/lt.20455. [DOI] [PubMed] [Google Scholar]
- 111.Russo MW, Firpi RJ, Nelson DR, Schoonhoven R, Shrestha R, Fried MW. Early hepatic stellate cell activation is associated with advanced fibrosis after liver transplantation in recipients with hepatitis C. Liver Transpl. 2005;11:1235–1241. doi: 10.1002/lt.20432. [DOI] [PubMed] [Google Scholar]
- 112.Carotti S, Morini S, Corradini SG, Burza MA, Molinaro A, Carpino G, Merli M, De Santis A, Muda AO, Rossi M, et al. Glial fibrillary acidic protein as an early marker of hepatic stellate cell activation in chronic and posttransplant recurrent hepatitis C. Liver Transpl. 2008;14:806–814. doi: 10.1002/lt.21436. [DOI] [PubMed] [Google Scholar]
- 113.Zadori G, Gelley F, Torzsok P, Sárváry E, Doros A, Deak AP, Nagy P, Schaff Z, Kiss A, Nemes B. Examination of claudin-1 expression in patients undergoing liver transplantation owing to hepatitis C virus cirrhosis. Transplant Proc. 2011;43:1267–1271. doi: 10.1016/j.transproceed.2011.03.066. [DOI] [PubMed] [Google Scholar]
- 114.Schmeding M, Dankof A, Krenn V, Krukemeyer MG, Koch M, Spinelli A, Langrehr JM, Neumann UP, Neuhaus P. C4d in acute rejection after liver transplantation--a valuable tool in differential diagnosis to hepatitis C recurrence. Am J Transplant. 2006;6:523–530. doi: 10.1111/j.1600-6143.2005.01180.x. [DOI] [PubMed] [Google Scholar]
- 115.Lorho R, Turlin B, Aqodad N, Triki N, de Lajarte-Thirouard AS, Camus C, Lakehal M, Compagnon P, Dupont-Bierre E, Meunier B, et al. C4d: a marker for hepatic transplant rejection. Transplant Proc. 2006;38:2333–2334. doi: 10.1016/j.transproceed.2006.06.120. [DOI] [PubMed] [Google Scholar]
- 116.Jain A, Ryan C, Mohanka R, Orloff M, Abt P, Romano J, Bryan L, Batzold P, Mantry P, Bozorgzadeh A. Characterization of CD4, CD8, CD56 positive lymphocytes and C4d deposits to distinguish acute cellular rejection from recurrent hepatitis C in post-liver transplant biopsies. Clin Transplant. 2006;20:624–633. doi: 10.1111/j.1399-0012.2006.00528.x. [DOI] [PubMed] [Google Scholar]
- 117.Fayek SA. The value of C4d deposit in post liver transplant liver biopsies. Transpl Immunol. 2012;27:166–170. doi: 10.1016/j.trim.2012.08.004. [DOI] [PubMed] [Google Scholar]
- 118.MacQuillan GC, de Boer WB, Allan JE, Platten MA, Reed WD, Jeffrey GP. Hepatocellular MxA protein expression supports the differentiation of recurrent hepatitis C disease from acute cellular rejection after liver transplantation. Clin Transplant. 2010;24:252–258. doi: 10.1111/j.1399-0012.2009.01068.x. [DOI] [PubMed] [Google Scholar]
- 119.Borgogna C, Toniutto P, Smirne C, Azzimonti B, Rittà M, Avellini C, Fabris C, Landolfo S, Gariglio M, Pirisi M. Expression of the interferon-inducible proteins MxA and IFI16 in liver allografts. Histopathology. 2009;54:837–846. doi: 10.1111/j.1365-2559.2009.03311.x. [DOI] [PubMed] [Google Scholar]
- 120.Marshall A, Rushbrook S, Morris LS, Scott IS, Vowler SL, Davies SE, Coleman N, Alexander G. Hepatocyte expression of minichromosome maintenance protein-2 predicts fibrosis progression after transplantation for chronic hepatitis C virus: a pilot study. Liver Transpl. 2005;11:427–433. doi: 10.1002/lt.20347. [DOI] [PubMed] [Google Scholar]
- 121.Unitt E, Gelson W, Davies SE, Coleman N, Alexander GJ. Minichromosome maintenance protein-2-positive portal tract lymphocytes distinguish acute cellular rejection from hepatitis C virus recurrence after liver transplantation. Liver Transpl. 2009;15:306–312. doi: 10.1002/lt.21680. [DOI] [PubMed] [Google Scholar]
- 122.Di Martino V, Saurini F, Samuel D, Gigou M, Dussaix E, Reynès M, Bismuth H, Féray C. Long-term longitudinal study of intrahepatic hepatitis C virus replication after liver transplantation. Hepatology. 1997;26:1343–1350. doi: 10.1053/jhep.1997.v26.pm0009362382. [DOI] [PubMed] [Google Scholar]
- 123.Fragulidis GP, Cirocco RE, Weppler D, Berho M, Gillian G, Markou M, Viciana A, Esquenazi V, Nery JR, Miller J, et al. In situ enzymatic oligonucleotide amplification of hepatitis C virus-RNA in liver biopsy specimens (reverse transcriptase in situ polymerase chain reaction) after orthotopic liver transplantation for hepatitis C-related liver disease. Transplantation. 1998;66:1472–1476. doi: 10.1097/00007890-199812150-00010. [DOI] [PubMed] [Google Scholar]
- 124.Aardema KL, Nakhleh RE, Terry LK, Burd EM, Ma CK, Moonka DK, Brown KA, Abouljoud MS. Quantitation of hepatitis C virus RNA in liver tissue of allografts: correlation with histologic features and liver function tests. Transplant Proc. 1999;31:477–478. doi: 10.1016/s0041-1345(98)01716-3. [DOI] [PubMed] [Google Scholar]
- 125.Negro F, Giostra E, Krawczynski K, Quadri R, Rubbia-Brandt L, Mentha G, Colucci G, Perrin L, Hadengue A. Detection of intrahepatic hepatitis C virus replication by strand-specific semi-quantitative RT-PCR: preliminary application to the liver transplantation model. J Hepatol. 1998;29:1–11. doi: 10.1016/s0168-8278(98)80172-4. [DOI] [PubMed] [Google Scholar]
- 126.Ge D, Fellay J, Thompson AJ, Simon JS, Shianna KV, Urban TJ, Heinzen EL, Qiu P, Bertelsen AH, Muir AJ, et al. Genetic variation in IL28B predicts hepatitis C treatment-induced viral clearance. Nature. 2009;461:399–401. doi: 10.1038/nature08309. [DOI] [PubMed] [Google Scholar]
- 127.Motomura T, Taketomi A, Fukuhara T, Mano Y, Takeishi K, Toshima T, Harada N, Uchiyama H, Yoshizumi T, Soejima Y, et al. The impact of IL28B genetic variants on recurrent hepatitis C in liver transplantation: significant lessons from a dual graft case. Am J Transplant. 2011;11:1325–1329. doi: 10.1111/j.1600-6143.2011.03537.x. [DOI] [PubMed] [Google Scholar]
- 128.Coto-Llerena M, Pérez-Del-Pulgar S, Crespo G, Carrión JA, Martínez SM, Sánchez-Tapias JM, Martorell J, Navasa M, Forns X. Donor and recipient IL28B polymorphisms in HCV-infected patients undergoing antiviral therapy before and after liver transplantation. Am J Transplant. 2011;11:1051–1057. doi: 10.1111/j.1600-6143.2011.03491.x. [DOI] [PubMed] [Google Scholar]
- 129.Eurich D, Boas-Knoop S, Ruehl M, Schulz M, Carrillo ED, Berg T, Neuhaus R, Neuhaus P, Neumann UP, Bahra M. Relationship between the interleukin-28b gene polymorphism and the histological severity of hepatitis C virus-induced graft inflammation and the response to antiviral therapy after liver transplantation. Liver Transpl. 2011;17:289–298. doi: 10.1002/lt.22235. [DOI] [PubMed] [Google Scholar]
- 130.Charlton MR, Thompson A, Veldt BJ, Watt K, Tillmann H, Poterucha JJ, Heimbach JK, Goldstein D, McHutchison J. Interleukin-28B polymorphisms are associated with histological recurrence and treatment response following liver transplantation in patients with hepatitis C virus infection. Hepatology. 2011;53:317–324. doi: 10.1002/hep.24074. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 131.Duarte-Rojo A, Deneke MG, Charlton MR. Interleukin-28B polymorphism in hepatitis C and liver transplantation. Liver Transpl. 2013;19:49–58. doi: 10.1002/lt.23554. [DOI] [PubMed] [Google Scholar]
- 132.Kawaoka T, Takahashi S, Takaki S, Hiramatsu A, Waki K, Hiraga N, Miki D, Tsuge M, Imamura M, Kawakami Y, et al. Interleukin-28B single nucleotide polymorphism of donors and recipients can predict viral response to pegylated interferon/ribavirin therapy in patients with recurrent hepatitis C after living donor liver transplantation. J Gastroenterol Hepatol. 2012;27:1467–1472. doi: 10.1111/j.1440-1746.2012.07129.x. [DOI] [PubMed] [Google Scholar]
- 133.Graziadei IW, Zoller HM, Schloegl A, Nachbaur K, Pfeiffer KP, Mark W, Mikuz G, Pratschke J, Margreiter R, Vogel W. Early viral load and recipient interleukin-28B rs12979860 genotype are predictors of the progression of hepatitis C after liver transplantation. Liver Transpl. 2012;18:671–679. doi: 10.1002/lt.23402. [DOI] [PubMed] [Google Scholar]
- 134.Fabris C, Falleti E, Cussigh A, Bitetto D, Fontanini E, Colletta C, Vandelli C, Cmet S, Ceriani E, Smirne C, et al. The interleukin 28B rs12979860 C/T polymorphism and serum cholesterol as predictors of fibrosis progression in patients with chronic hepatitis C and persistently normal transaminases. J Med Virol. 2012;84:747–755. doi: 10.1002/jmv.23259. [DOI] [PubMed] [Google Scholar]
- 135.Dharancy S, Podevin P, Aoudjehane L, Batteux F, Rosenberg AR, Soubrane O, Calmus Y, Conti F. Elevated interleukin-4 expression in severe recurrent hepatitis C virus after liver transplantation. Transplantation. 2007;83:906–911. doi: 10.1097/01.tp.0000258729.68871.be. [DOI] [PubMed] [Google Scholar]
- 136.Gehrau R, Maluf D, Archer K, Stravitz R, Suh J, Le N, Mas V. Molecular pathways differentiate hepatitis C virus (HCV) recurrence from acute cellular rejection in HCV liver recipients. Mol Med. 2011;17:824–833. doi: 10.2119/molmed.2011.00072. [DOI] [PMC free article] [PubMed] [Google Scholar]