

Abstract
Warfarin is the most common anticoagulant prescribed and its metabolism has been linked to two specific genes, CYP2C9 and VKORC1. This study analyzed 113 patients from 4 different ethnic backgrounds (Asian, Native Hawaiian, Portuguese, and Caucasian) and investigated the association between the mean daily dose of warfarin and ethnicity. Caucasian patients required the highest mean daily dose of warfarin 4.4 mg/day while Asian patients required the lowest mean daily dose of warfarin 2.5 mg/day. Portuguese patients and Native Hawaiian patients required mean of 3.8 mg/day. All three groups required a significantly lower dose than Caucasians. When adjusted for weight in kilograms, Native Hawaiian patients required a dose of 4.3 × 10−2 mg/kg, Portuguese 4.4 × 10−2 mg/kg and Asians 4.0 × 10−2 mg/kg. These three populations had similar mean milligrams/kilogram dose requirements while Caucasians required a significantly higher dose of 5.3 × 10−2 mg/kg. This data suggests that ethnicity should be taken into consideration when dosing warfarin.
Introduction
Despite the introduction of new anti-thrombotics including Pradaxa, Xarelto, and Eliquis, warfarin continues to be the most commonly prescribed medication for the treatment and prevention of thromboembolic states, including atrial fibrillation, deep venous thrombosis, pulmonary emboli, valvular heart disease, and hypercoagulable states.1 The problem with warfarin is it has to be titrated within a narrow therapeutic index, usually between the International Normalized Ratio (INR) of 2.0 to 3.0.2 This narrow therapeutic window increases the risk of either under anticoagulating or over anticoagulating. In the past, certain clinical variables including age, weight, sex, diet, co-morbid conditions, and concomitant medications have been considered as factors that affect warfarin metabolism.1 Compliance is often an issue and lifestyle variations including frequent travel may also play a role. In addition, there is an increasing body of evidence that genetics plays an important role in warfarin metabolism. Currently there are two studies being conducted to investigate this; the first is the Clarification of Optimal Anticoagulation through Genetics (COAG) study which is sponsored by the National Heart, Lung, and Blood Institute. The second study is the European Pharmacogenetics of Anticoagulant Therapy-Phenprocoumon (EU-PACT) study that is being conducted in Europe. These two studies are looking into whether genetic information should be considered when warfarin is administered.3,4
Two genes have been extensively studied regarding their roles in warfarin metabolism. The first is the cytochrome P-450 gene (specifically, CYP2C9) and the second is vitamin K epoxide reductase subunit 1 gene (VKORC1).5 The CYP2C9 enzyme acts as a catalyst in many different reactions including the metabolism of warfarin. Two single nucleotide polymorphisms (SNPs) affecting warfarin metabolism have been identified. The alleles with these SNPs are referred to as CYP2C9*2 and CYP2C9*3, with the wild type being referred to as CYP2C9*1. VKORC1 is the enzyme that regenerates reduced vitamin K and the VKORC1 enzyme is inhibited by warfarin.6 As a result, in the presence of warfarin, the coagulation factors become hypofunctional. SNPs in the VKORC1 gene decrease the enzymatic activity of the VKORC1 enzyme, ultimately requiring less warfarin. The effects of CYP2C9 and VKORC1 on warfarin metabolism are exhibited in Figure 1.6
Figure 1.
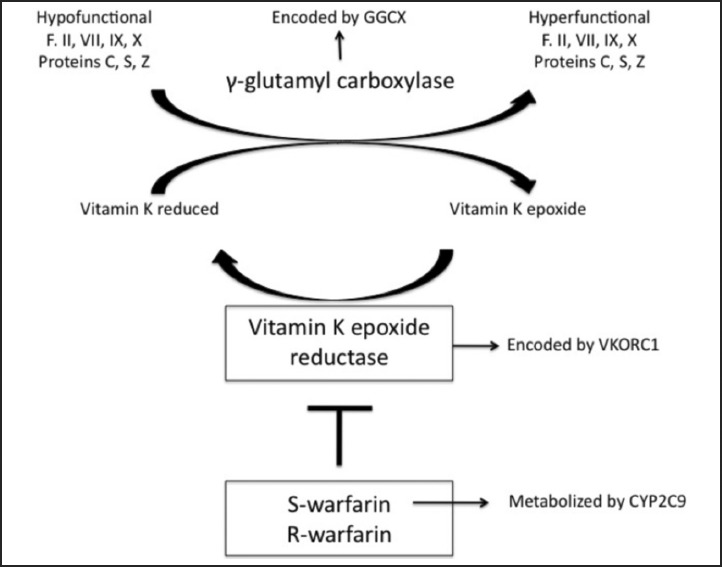
Metabolism of S-Warfarin within the liver.6 (Reproduced with permission.)
Many physicians even in Hawai‘i are not aware that ethnicity plays a role in the dosing of warfarin and many of the major health insurers in Hawai‘i currently do not pay for genetic testing to assist with warfarin dosing. Therefore, ethnicity can serve as a useful proxy. This study evaluates whether significant differences in dosing of warfarin exist by ethnicity.
Methods
This study was conducted in 2013 and was limited to just these four ethnic-racial groups: Asians, Native Hawaiians, Portuguese, and Caucasians. Ethnicity was self-reported, and either determined by chart review or by direct questioning. Native Hawaiian was defined as having any Hawaiian ancestry, no data on full Hawaiians were available for this study. Asians in this study were predominantly of Japanese ancestry. Portuguese are generally classified as Caucasians, however, they were separated in this study to see if there were any differences between individuals identifying as Portuguese and other Caucasians, to enable comparison to the literature. Most of the patients included in the study were current patients and had to be on a stable dose of warfarin for at least three months with an INR between 2.0 and 3.0. There were no other inclusion criteria other than ethnicity and being on a stable dose of warfarin with an INR between 2.0 and 3.0. Data was obtained from four private practices located in Hilo Hawai‘i, and one individual, either a physician or a nurse, from each of the practices was responsible for following the inclusion criteria and compiling the data. The data obtained was pooled and statistically analyzed using an ANOVA test available through MicroCase®. Mean dose of warfarin per day and the mean dose per day per kilogram between the ethnic groups were compared.
Results
A total of 113 patients fulfilled the inclusion criteria. Of these, 43 (38%) were Asians, 23 (20%) Native Hawaiians, 17 (15%) Portuguese and 30 (26%) Caucasians. There were 73 (65%) men and 40 (35%) women between the ages of 51 and 101 years (mean age of 76). Patients were stratified according to age, ethnicity, required daily dose of warfarin (mg), and daily dose of warfarin divided by total weight in kilograms (mg/kg). Asians needed the lowest dose per day with an average of 2.5 mg/day, followed by Native Hawaiians and Portuguese each with a dose of 3.8 mg/day, and Caucasians with a dose of 4.4 mg/day. The difference in means across groups was determined to be statistically significant (P < .05). When adjusted by weight in kilograms, Asians had a dose of 4.0 × 10−2 mg per kg, Native Hawaiians had a dose of 4.3 × 10−2 mg per kg, Portuguese had a dose of 4.4 × 10−2 mg per kg followed by Caucasians with a dose of 5.3 × 10−2 mg per kg. Again, the difference in means across groups was statistically significant (P < .05). The effects of ethnicity on warfarin dosing are exhibited in Tables 1 and 2.
Table 1.
Average Warfarin Dose (mg) Across the Population
| Ethnicity | N | Mean (mg) | Std. Dev. |
| Hawaiian | 23 | 3.8 | 2.3 |
| Caucasian | 30 | 4.4 | 1.9 |
| Portuguese | 17 | 3.8 | 1.7 |
| Asian | 43 | 2.5 | 1.1 |
P-value <.05
Table 2.
Average mg/kg to Achieve Optimal INR Across the Population
| Ethnicity | N | Mean (mg/kg) | Std. Dev. |
| Hawaiian | 23 | 4.3 × 10−2 | 2.3 × 10−2 |
| Caucasian | 30 | 5.3 × 10−2 | 2.1 × 10−2 |
| Portuguese | 17 | 4.4 × 10−2 | 2.0 × 10−2 |
| Asian | 43 | 4.0 × 10−2 | 1.4 × 10−2 |
P-value <.05
Discussion
The most common genotype of CYP2C9 is homozygous CYP2C9*1/CYP2C9*1 which is also referred to as the wild type genotype. There are two common variants of the CYP2C9 allele, the CYP2C9*2 and the CYP2C9*3 both of which encode enzymes that have less activity, ultimately requiring a lower dose of warfarin. Both homozygous and heterozygous states also exist for CYP2C9*2 and CYP2C9*3. The heterozygous states may significantly lower the warfarin dose anywhere from 20% to 57%. The homozygous states of the CYP2C9*2 and CYP2C9*3 alleles may lower the dose anywhere from 36% to 78%.5 However, most Asians (85%) are predominantly homozygous for the CYP2C9*1/CYP2C9*1 alleles7 and as a result, the decreased warfarin requirements in the Asian population cannot be explained by variants in this genotype.
Instead, the decreased dose of warfarin in the Asian population can be adequately explained by the VKORC1 enzyme. Mutations in VKORC1 cause a deficiency in the vitamin K dependent clotting factors ultimately resulting in increased sensitivity to warfarin and lowered dosages. Patients can be homozygous for this enzyme (A/A or non A/non A) or heterozygous (A/non A). Those individuals who are homozygous for the (A/A) genotype require about 50% less warfarin than the non A/non A genotype, and those that are heterozygous (A/nonA) require about 26% less warfarin than the non A/non A genotype.8 These findings regarding the VKORC1 have been most extensively studied in the Japanese and Chinese populations.5,10–12 However, not all Asians require a lower dose of warfarin. In the East Indian population, the mean daily dose of warfarin was higher compared to two other Asian groups, the Chinese and Malay (4.9 mg/day, 3.7 mg/day, and 3.1 mg/day respectively).9 This could be explained in part by the finding that East Indians have a higher frequency of the non A/non A genotype.13,14 In addition, it may be hypothesized that other Southeast Asian populations including Filipino, Thai, Vietnamese, and Indonesian patients will have similar VKORC1 genotypes as the Chinese, Japanese and Korean populations and will ultimately require lower doses of warfarin.13
In this study, Portuguese in Hawai‘i seemed to require less warfarin than the rest of the Caucasian population. However, a recent article confirms that the genetic variations in the Portuguese regarding the CYP2C9 and the VKORC1 genes are similar to the rest of the Caucasian population.15
African Americans generally require higher warfarin doses compared to other ethnic groups including Caucasians. This may be in part due to the lower frequencies of the CYP2C9*2, CYP2C9*3 and VKORC1 A alleles present in African Americans. A variant allele of gamma glutamyl carboxylase (GGCX), an enzyme that catalyzes the formation of vitamin K-dependent clotting factors, has been found to be present at a higher frequency within the African American population. This may be responsible in part for the higher dosing requirement needed in African Americans.16 In that study, it was estimated that approximately 25% of African Americans require doses greater than 7.5 mg of warfarin per day. The Puerto Rican population which is a mixture of European, Amerindian, and African ancestry may require a lower warfarin dose;17 this also appears to be true in the Mexican population.18
The findings of the current study suggest that Native Hawaiians appear to require a lower dose of warfarin than Caucasians; moreover, when adjusted for weight, at least three Hawai‘i ethnic groups (Asians, Portuguese and Native Hawaiians) have similar dosing requirements. The local diet commonly shared among these three ethnic groups could be a factor.1 Further research should be done on Hawai‘i's Native Hawaiian and Pacific Islander populations.
There are significant implications regarding these ethnic differences in the dosing of warfarin and suggest that race-ethnicity should be taken into consideration when initiating the dose of the warfarin and when trying to calculate the maintenance dose. Current algorithms for warfarin dosing used in hospitals do not consider these ethnic differences. In addition to ethnic differences, age and BMI should also be considered. There are several articles proposing algorithms based on pharmacogenetics and warfarin dosing, including ones from Korea and Italy.19,20 The COAG study and EU-PACT 3,4 should be completed soon. Further studies are being conducted on the role genetics plays in warfarin dosing, which include other genes like GGCX and CYP4F2, another enzyme in the cytochrome P-450 family.21 Currently most HMSA plans including HMSA Quest do not pay for CYP2C9 and the VKORC1 gene testing. Some of the Medicare plans including Part A do pay for it as does University Health Alliance, United Healthcare and Tricare. The results of the EU-PACT and COAG studies may determine whether other insurance companies pay for this testing. According to a correspondence with Doctor Chelestes Grace of Clinical Laboratories of Hawai‘i currently costs run at approximately $250 to $350 for both tests (written communication, October 2013). Limitations of this study include the small sample size, and inaccuracies inherent to capturing ethnicity through chart review or self-reporting. The low sample size precluded a finer analysis of the distinctions among Asian populations in Hawai‘i.
Conclusions
This study confirms that there are ethnic differences in the dosing of warfarin, and weight is also an important factor to consider. Caucasians need almost 2 mg per day more warfarin than Asians. When adjusted for weight, Asians, Portuguese, and Native Hawaiians have similar dosing requirements. This clustering despite the difference in genetic makeup seems to implicate other factors that may be involved, including diet. However, when adjusted for weight, Asians, Portuguese, and Native Hawaiians need a lower dose than the Caucasians. These findings have significant clinical implications.
Acknowledgements
Special thanks to Drs. Henry Lee Loy, Djon Lim, Don Matsuura, and Alton Okinaka.
Conflict of Interest
None of the authors identify a conflict of interest.
References
- 1.Moon HW, Noh J, Yeo-Min Y, et al. The effect of CYP2C9, VKORC1 genotypes and old age on warfarin pharmacologic sensitivity in Korean patients with thromboembolic disease. Annals of Clinical & Laboratory Science. 2011;41:229–235. [PubMed] [Google Scholar]
- 2.Anderson J, Horne B, Stevens S, et al. Randomized trial of genotype-guided versus standard warfarin dosing in patients initiating oral anticoagulation. Circulation. 2007;116:2563–2570. doi: 10.1161/CIRCULATIONAHA.107.737312. [DOI] [PubMed] [Google Scholar]
- 3.Clinical Trials A Service of the U.S. National Institutes of Health, author. Clarification of Optimal Anticoagulation through Genetics. [July, 2013]. http://www.clinicaltrials.gov/ct2/show/NCT00839657.
- 4.Clinical Trials A Service of the U.S. National Institutes of Health, author. European Pharmacogenetics of Anticoagulant Therapy. [July, 2013]. http://www.clinicaltrials.gov/ct2/show/NCT01119300.
- 5.Lam M, Cheung B. The pharmacogenetics of the response to warfarin in Chinese. British Journal of Clinical Pharmacology. 2011;73(3):340–347. doi: 10.1111/j.1365-2125.2011.04097.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Yin T, Miyata T. Warfarin dose and the pharmacogenomics of CYP2C9 and VKORC1 - rationale and perspectives. Thrombosis research. 2007;120:1–10. doi: 10.1016/j.thromres.2006.10.021. [DOI] [PubMed] [Google Scholar]
- 7.Gulseth M, Grice G, Dager W. Pharmacogenomics of warfarin: uncovering a piece of the warfarin mystery. Am J Health-Syst Pharm. 2009;66:123–133. doi: 10.2146/ajhp080127. [DOI] [PubMed] [Google Scholar]
- 8.Weitz J. Harrison's Principles of Internal Medicine. 18th edition. New York, NY: McGraw Hill Medical; 2012. pp. 998–1000. [Google Scholar]
- 9.Gan GG, Phipps M, Lee M, et al. Contribution of VKORC1 and CYP2C9 polymorphisms in the interethnic variability of warfarin dose in Malaysian populations. Ann Hematology. 2011;90:635–641. doi: 10.1007/s00277-010-1119-6. [DOI] [PubMed] [Google Scholar]
- 10.Mushiroda T, Ohnishi Y, Saito S, et al. Association of VKORC1 and CYP2C9 polymorphisms with warfarin dose requirements in Japanese patients. J Hum Genet. 2006;51:249–253. doi: 10.1007/s10038-005-0354-5. [DOI] [PubMed] [Google Scholar]
- 11.Obayashi K, Nakamura K, Kawana J, et al. VKORC1 gene variations are the major contributors of variation in warfarin dose in Japanese patients. Clinical Pharmacology & Therapeutics. 2006;80(2):169–178. doi: 10.1016/j.clpt.2006.04.010. [DOI] [PubMed] [Google Scholar]
- 12.Ma C, Zhang Y, Xu Q, et al. Influence of warfarin dose-associated genotypes on the risk of hemorrhagic complications in Chinese patients on warfarin. Int J Hematol. 2012;96:719–728. doi: 10.1007/s12185-012-1205-8. [DOI] [PubMed] [Google Scholar]
- 13.Lee M, Chen CH, Chuang H, et al. VKORC1 haplotypes in five East-Asian populations and Indians. Pharmacogenomics. 2009;10(10):1209–1216. doi: 10.2217/pgs.09.80. [DOI] [PubMed] [Google Scholar]
- 14.Lee SC, Ng SS, Oldenburg J, et al. Interethnic variability of warfarin maintenance requirement is explained by VKORC1 genotype in an Asian population. Clinical Pharmacology & Therapeutics. 2006;79(3):197–205. doi: 10.1016/j.clpt.2005.11.006. [DOI] [PubMed] [Google Scholar]
- 15.Jorge E, Pego JM, Baptista R, et al. Genetic characterization of warfarin sensitivity in a population of cardiovascular patients on chronic anticoagulation. Rev Port Cardiol. 2010;29(12):1831–1838. [PubMed] [Google Scholar]
- 16.Cavallari L, Perera M, Wadelius M, et al. Association of the GGCX (CAA)16/17 repeat polymorphism with higher warfarin dose requirements in African Americans. Pharmacogenet Genomics. 2012;22(2):152–158. doi: 10.1097/FPC.0b013e32834f288f. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Valentin IV, Vazquez J, Rivera-Miranda G, et al. Prediction of warfarin dose reductions in Puerto Rican patients, based on combinatorial CYP2C9 and VKORC1 genotypes. The Annals of Pharmacotherapy. 2012;46:208–2018. doi: 10.1345/aph.1Q190. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Llerena A, Dorado P, O'Kirwan F, et al. Lower frequency of CYP2C9*2 in Mexican-Americans compared to Spaniards. The Pharmacogenomics Journal. 2004;4:403–406. doi: 10.1038/sj.tpj.6500278. [DOI] [PubMed] [Google Scholar]
- 19.Choi J, Kim J, Kang D, et al. Proposal of pharmacogenetics-based warfarin dosing algorithm in Korean patients. Journal of Human Genetics. 2011;56:290–295. doi: 10.1038/jhg.2011.4. [DOI] [PubMed] [Google Scholar]
- 20.Cini M, Legnani C, Cosmi B, et al. A new warfarin dosing algorithm including VKORC1 3730 G > A polymorphisms: comparison with results obtained by other published algorithms. Eur J Clin Pharmacol. 2012;68:1167–1174. doi: 10.1007/s00228-012-1226-5. [DOI] [PubMed] [Google Scholar]
- 21.Chan S, Goh B, Chia K, et al. Effects of CYP4F2 and GGCX genetic variants on maintenance warfarin dose in a multi-ethnic Asian population. Thrombosis and Haemostasis. 2011;105:1100–1102. doi: 10.1160/TH11-01-0018. [DOI] [PubMed] [Google Scholar]