

Abstract
Introduction:
Bone metastases are frequently seen in patients with malignancies, but only 0.007% to 0.3% of these metastases are located in the hand or foot. In 16%, the metastasis is the first manifestation of a malignancy. These acrometastases have a poor prognoses with a median survival of 6 months. Treatment is usually palliative and consists of radiation or amputation.
Case Description:
An 83-year-old woman was seen with pain and swelling of the right middle finger since 3 months. A radiograph of this finger showed a lytic lesion of the proximal phalanx. A metastasis, primary bone tumor, or osteomyelitis was considered. Because of a radically resected colon carcinoma in patient’s medical history, the carcinoembryonic antigen level was analyzed and proved to be elevated. Computed tomography scan of thorax and abdomen showed 2 (primary) pulmonary tumors with mesenteric metastases. Patient refrained from further analysis and treatment of these lung tumors. However, because of persistent pain the right middle finger was amputated. Pathological examination of the finger confirmed the diagnosis of an adenocarcinoma most likely to be a metastasis of lung cancer. Lung cancer is in most cases responsible for metastases in the hand.
Conclusion:
Acrometastasis may be the first manifestation of malignancy. Given the poor prognosis, early diagnosis is important to offer adequate treatment. Delay of appropriate treatment can adversely affect the quality of life in these often preterminal patients. This case report could contribute to a (more) rapid recognition of acrometastases as patients with acrometastases are often presented to specialists who do not frequently deal with cancer.
Keywords: musculoskeletal tumor surgery, oncology, upper extremity surgery, surgery, acrometastasis
Introduction
Bone metastases are frequently seen in patients with malignancies.1 But only 0.007% to 0.3% of these metastases are located in the hand or foot. In 16%, the metastasis is the first manifestation of a malignancy.2 These acrometases have a poor prognosis with a median survival of 6 months.3 This prognosis increases the importance of a timely diagnosis so that appropriate treatment can be started. Delay in appropriate treatment can adversely affect the quality of life in these often preterminal patients. This case report could contribute to a (more) rapid recognition of acrometastases as patients with acrometastases are often presented to specialists who do not frequently deal with cancer.
Case Report
An 83-year-old woman was seen with pain and swelling of the right middle finger. These symptoms occurred after opening a jar 3 months earlier. The patient has always been a housewife and smoked 1 pack of tobacco a week together with an unknown number of cigarettes. For the last few months, the patient felt to be more tired and was coughing up clear sputum without blood. The cough pattern was not changed. There were no altered bowel habits, no abnormal vaginal discharge, and the patient had not fallen. Other bones and/or joints were not painful. The history mentioned chronic obstructive pulmonary disease, diverticulosis, and colon polyps with a radical resection of a colonic polyp with infiltrating adenocarcinoma in 1993. This was followed by colonoscopic surveillance, the last taken place in August 2012, without any other malignancies to be found. On physical examination, a painful swelling of the third digit was seen without signs of infection. A radiograph showed a pathological fracture through a lytic process in the proximal phalanx of the third digit with significant soft tissue expansion, whereas an expansive tumor in the third digit with complete destruction of the proximal phalanx was seen on a magnetic resonance imaging (Figures 1 –3). A metastasis, primary bone tumor, or osteomyelitis was considered. Extensive blood tests were performed, including paraprotein and carcinoembryonic antigen (CEA). Also, a bone scan was made. Blood tests revealed an elevated CEA of 82 ng/mL (normal value <5 ng/mL) The bone scan revealed a strongly increased activity of the proximal phalanx of the affected finger and some activity in the skull and left femur. A metastatic disease was still of concern. Therefore, a conventional radiograph of the left femur was made, where a lytic lesion was seen, which made metastasis a probable cause of the patient’s symptoms. Additionally, a liver ultrasound and chest radiograph were conducted. The radiograph showed 2 spots suspicious for malignancy. The liver ultrasound showed no abnormalities. Computed tomography scan of thorax and abdomen showed 2 (primary) pulmonary tumors with mesenteric metastases. The lung tumors were classified as T2bN3M1b and T1NxMx. More analyses to diagnose the primary tumor would be desirable.
Figure 1.

The radiograph showed a pathological fracture through a lytic process in the proximal phalanx of the third digit with significant soft tissue expansion.
Figure 2.

Coronal magnetic resonance imaging (MRI) showed an expansive tumor in the third digit with complete destruction of the proximal phalanx.
Figure 3.
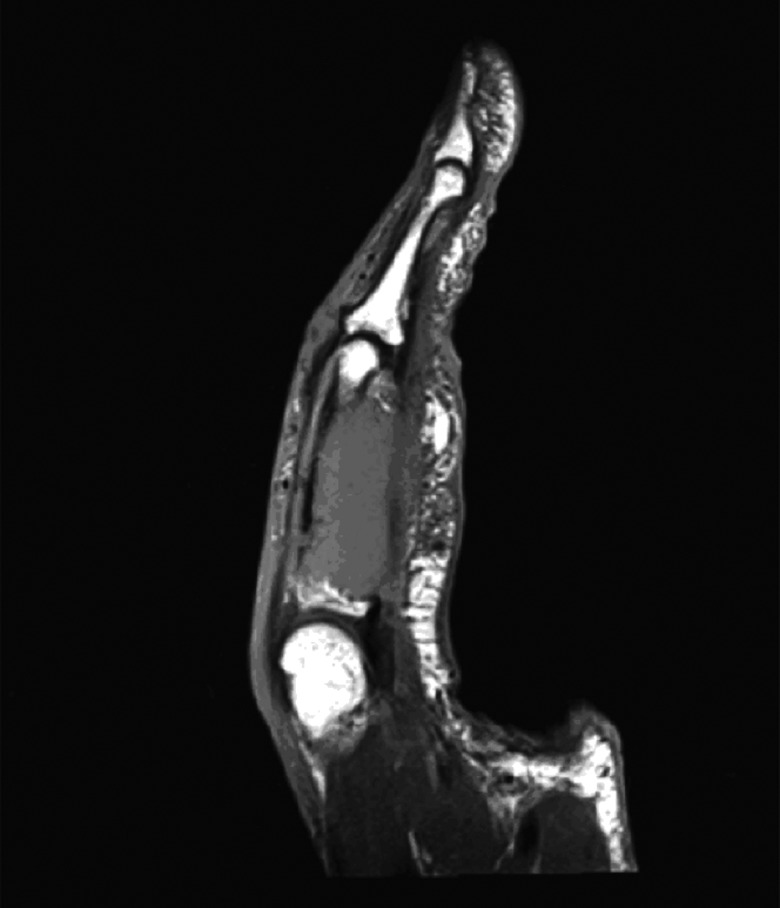
Sagittal magnetic resonance imaging (MRI) showed an expansive tumor in the third digit with complete destruction of the proximal phalanx.
However, the patient refrained from further analysis and treatment of the lung tumors. Because of severe pain in the third digit, which did not improve after conservative therapy, a palliative amputation of the finger was executed. Pathological examination of the finger showed an adenocarcinoma, most likely to be a metastasis of lung cancer.
Discussion
Metastases are the most common malignant tumors of the bone.1 Osseous metastases are seen, particularly in breast, lung, and prostate cancer.1 The axial skeleton is most likely to be affected.1 Metastases in the hand and foot are rare, only 0.007% to 0.3% of all bonemetastases.3 However, for a considerable percentage of patients, the acrometastasis will be the first manifestation of a malignancy. Metastases in the hand arise mainly from lung (47%), kidney (13%), and breast cancer (12%).4 Metastasis in the foot are usually caused by genitourinary and colorectal malignancies.5 Acrometastases are twice more common in the hand than in foot and more frequently occur in men.4 This may be explained by the higher incidence of lung carcinomas in men.4 Metastases of the hand are usually unilateral, with a preference for the dominant hand.3 This latter is probably caused by the hematogenous distribution of the metastases and the increased circulation in the dominant hand.3 The metastasis affects most frequently the middle finger (28%) and the thumb (21%).6
The median survival after presentation of a metastasis in the hand or foot is believed to be 6 months.6 However, recent data concerning survival rates are not available. It is possible that survival rates have improved. Still, given the assumed poor prognosis, early diagnosis is important. Delay of appropriate treatment can adversely affect the quality of life in this often preterminal phase. Treatment is usually palliative and consists of radiation or amputation, and analgesia by opiates can also be considered.2 In this case, because of the high CEA level and lytic lesion in the femur shown on the bone scan, a metastatic process was considered. The carcinoembryonic antigen is a tumor marker that is often used in the follow-up of a colonic cancer. However, other causes can be responsible for an increase in CEA. Smokers often have a slightly elevated (<10 ng/mL) CEA (normal value <5 ng/mL).7 Benign conditions like colitis ulcerosa or hepatitis may also cause a slight increase in CEA levels.8 In addition to colon cancer, CEA can also be increased in other malignancies. This concerns in particular breast, pancreatic, and lung cancer.7 If the CEA is increased because of lung cancer, often an adenocarcinoma is responsible as in this case report.9
Conclusion
Acrometastases are rare. A metastasis in the hand may be the first manifestation of malignancy. Early recognition and timely diagnosis are important to offer adequate treatment and enhance quality of life in these preterminal patients.
Footnotes
Declaration of Conflicting Interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding: The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
- 1. Coleman RE. Metastatic bone disease: clinical features, pathophysiology and treatment strategies. Cancer Treat Rev. 2001;27(3):165–176 [DOI] [PubMed] [Google Scholar]
- 2. Hsu CS, Hentz VR, Yao J. Tumours of the hand. Lancet Oncol. 2007;8(2):157–166 [DOI] [PubMed] [Google Scholar]
- 3. Healy JH, Turnbull AD, Miedema B, Lana JM. Acrometastases A study of twenty-nine patients with osseous involvement of hands and feet. J Bone Joint Surg Am. 1986;68(5):743–746 [PubMed] [Google Scholar]
- 4. Libson E, Bloom RA, Husband JE. Metastatic tumours of bones of the hand and foot A comparative review and report of 43 additional cases. Skeletal Radiol. 1987;16(5):387–392 [DOI] [PubMed] [Google Scholar]
- 5. Lamarca A, Hindi N, Belda-Iniesta C, de Castro J. Foot pain: uncommon presentation of lung cancer. BMJ Case Rep. 2012;2012. doi:10.1136/bcr.12.2011.5360 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Flynn CJ, Danjoux C, Wong J, et al. Two cases of acrometastasis to the hands and review of the literature. Curr Oncol. 2008;15(5):51–58 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Vermorke JB, Schrijvers DLAL, Weysler L, et al. Diagnostiek in de oncologie. In: Van de Velde (ed.), In: Oncologie. 7th ed Houten, the Netherlands: Bohn Stafleu van Loghum, 2005:114 [Google Scholar]
- 8. Van Mil AHM, Beijer C, Jonkers GJPM. Hoge concentratie van carcino-embryonaal antigeen bij een vrouw met hypothyreoïdie. Ned Tijdschr Geneeskd. 2001;145(22):1071–1074 [PubMed] [Google Scholar]
- 9. Oncoline: Richtlijn Niet-kleincellig longcarcinoom. Versie: 2.0 Verantwoording: Landelijke Werkgroep Longtumoren; Type: Landelijke richtlijn; May 22, 2011 [Google Scholar]