

Abstract
A 48-year-old male patient presented to the emergency room with a history of chest pain and breathlessness. Chest X-ray demonstrated a large radio-opaque foreign body in relation to the proximal right bronchial tree. The patient subsequently revealed a history of a misplaced denture 4 months previously. Urgent flexible bronchoscopy (FB) examination demonstrated a large partial denture impacted in the right intermediate bronchus, which was removed successfully using a flexible bronchoscope. Although rigid bronchoscopy (RB) is the procedure of choice for large-sized and impacted airway foreign bodies, the present case highlights the utility of FB in airway foreign body removal. In clinically stable patients with foreign body inhalation, FB can be employed initially as it is an outpatient and cost-effective procedure which can obviate the need for administration of general anaesthesia.
Background
Airway foreign body aspiration is common in paediatric patients but can uncommonly occur in adults.1 In rare situations, it can be associated with fatal airway obstruction if a large-sized object is aspirated.2 RB is the preferred procedure for airway foreign body removal. This is owing to the ability of the rigid bronchoscope to sustain ventilation and provide stable airway control during the procedure. FB may be employed in clinically stable patients as it enables the procedure to be accomplished on an outpatient basis. It also obviates the need for general anaesthesia in most of the situations. Undetected tracheobronchial foreign bodies can lead to the formation of granulation tissue, which can complicate the procedure of flexible bronchoscopic retrieval. Successful and uncomplicated flexible bronchoscopic extraction of a large, partially impacted airway foreign body in our patient highlights the utility of FB in airway foreign body removal.
Case presentation
A 48-year-old male patient presented to the emergency room with a history of cough, shortness of breath and sensation of heaviness on the right side of the chest of 3-day duration. The patient was a heavy smoker with a 20 pack-year smoking history. On examination, the respiratory rate was 16/min and oxygen saturation was 96% while breathing room air. The general physical examination was unremarkable. On examination of the respiratory system, a monophonic wheeze was audible over the right hemithorax which was persistent after albuterol nebulisation. The rest of the systemic examination was normal. The ECG was normal and Troponin I measurement was negative. Chest X-ray revealed a large linear lobulated radio-opacity on the right side resembling the outline of a denture in the right bronchial tree (figure 1). The patient denied any use of alcohol and sedatives, and there was no prior history of convulsions. On careful questioning, the patient revealed that 4 months previously, when he woke up 1 day he could not find the denture in his mouth. He attributed the same to having misplaced/lost it somewhere.
Figure 1.

Chest X-ray showing a large radio-opaque foreign body in the right hemithorax in relation to the right bronchial tree.
FB examination was performed (using the Olympus BF-TE2 scope having a 2.8 mm working channel) through the oral route in the bronchoscopy laboratory. Written informed consent for the procedure was obtained. Local anaesthesia was obtained using nebulised lignocaine and lignocaine spray followed by insertion of a bite block. A large foreign body with a smooth and glistening surface (partial denture) was visualised in the right intermediate bronchus (figure 2). A Snare wire loop was inserted through the working channel of the bronchoscope which was employed to encircle around the groove in the denture (Video 1). After the denture had been secured firmly within the snare loop, it was removed along with the bronchoscope (figure 3). The foreign body was a large 4 unit denture (figure 4) that had led to the formation of non-bleeding granulation tissue at the point of circumferential contact on the bronchial wall (visualised after extraction of the foreign body; figure 5). There were no procedural complications. Repeat chest X-ray was normal and the patient was discharged home 2 h later. A repeat FB examination performed a month later was normal. The patient continues to be asymptomatic until now, 5 months since the denture removal was performed.
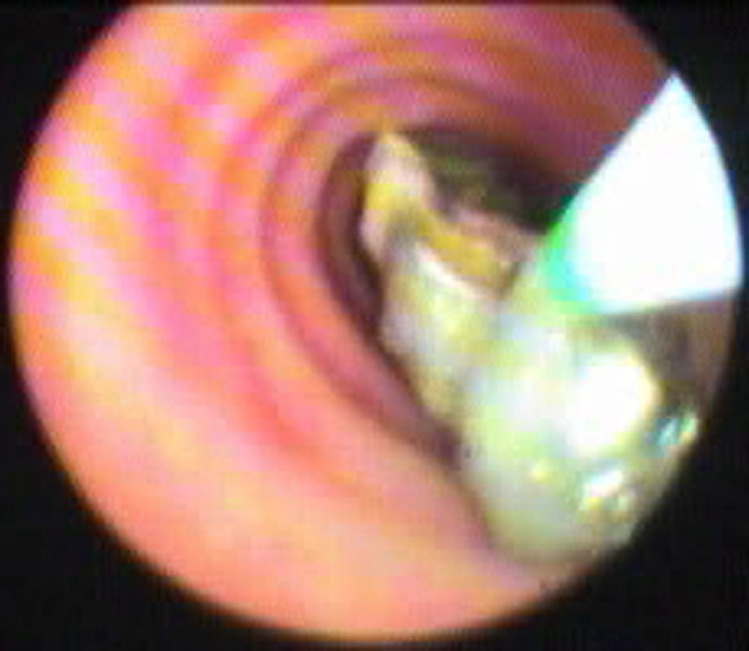
Figure 2.

Flexible bronchoscopic image showing a partially impacted denture in the right intermediate bronchus.
Figure 3.
Flexible bronchoscopic extraction of the denture being performed using the snare wire.
Figure 4.

Image showing the extracted denture unit.
Figure 5.
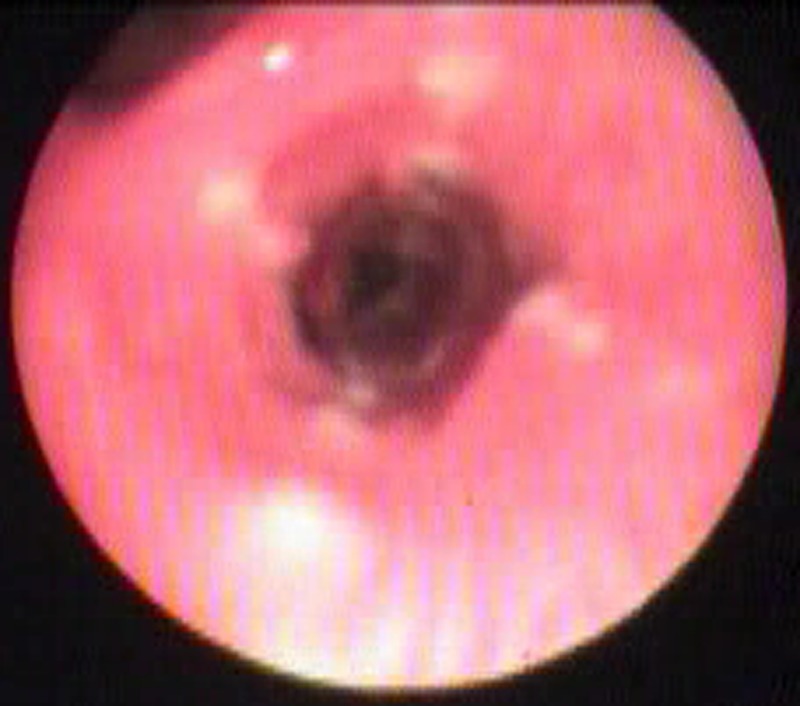
Flexible bronchoscopy image showing circumferential linear granulation tissue formation at the original site of foreign body impaction.
Video demonstrating the flexible bronchoscopic denture removal. A snare loop (Olympus, SD-7C1 snare) is employed to encircle around the groove in the denture and once in position, the loop is tightened. Following that, the denture is removed along with the bronchoscope.
Discussion
Timely bronchoscopic removal of aspirated airway foreign bodies is a must. Delayed diagnosis can be associated with a number of complications. These include infective postobstructive complications such as pneumonia and lung abscess. Recurrent infections distal to the obstructed segments can be complicated by bronchiectasis. Excessive granulation tissue formation can also occur due to the irritant effects of the foreign body, and the same can often cover the surface of the foreign body, making bronchoscopic recognition and removal difficult. This appearance can often mimic lung cancer.3 The right bronchial tree is the usual site of foreign body impaction owing to its linearity with the tracheal lumen and its larger diameter. Important risk factors for adult airway foreign body aspiration include conditions leading to impairment of cough reflex and poor sensorium due to the effects of drugs, alcohol or neurological dysfunction. Uncommonly, the initial event of foreign body aspiration in adults may remain unrecognised as in our patient.4 Rarely, fatal upper airway obstruction can also occur in adults due to aspiration of food material. The same may mimic an episode of acute coronary syndrome (therefore described as cafe coronary).5
Airway aspiration or swallowing of dental prosthetics represents an important problem.6 Aspiration of intact tooth or dentures during maxillofacial trauma has also been described.7 Recognition of aspirated dentures made of radiolucent material can be extremely challenging. Bronchoscopic airway examination is mandatory in all suspected cases of foreign body aspiration. RB provides excellent airway control during invasive interventional procedures in the airways.8 RB under general anaesthesia is a preferred technique particularly in patients with a large-sized foreign body or patients who are in respiratory failure following the episode. The rigid steel forceps allow for better grasping and the chances of migration of the foreign body distally or into the contralateral lung is less likely. FB is preferable in mechanically ventilated patients, distally impacted foreign bodies and in patients in whom excessive spine manipulation that may occur during RB is contraindicated (like patients with spinal fractures).
Flexible bronchoscopes have the capacity to remove almost any type of foreign body in adults because of the availability of several ancillary instruments.9 We routinely perform FB for initial assessment in all patients with airway foreign body aspiration at our institution. Most foreign bodies are removed successfully using a flexible bronchoscope itself.
However, it should be noted that if the patient is in respiratory failure or haemodynamically unstable, FB if required should be performed through the lumen of the rigid bronchoscope to provide airway control. Complications can often be encountered during FB retrieval of foreign bodies or tumours like loss of control over the foreign body leading to migration of the foreign body contralaterally or distally.10 The narrow subglottic space and vocal cords are the sites where loss of control over the foreign body is most likely. Foreign body impaction at this site may lead to acute upper airway obstruction. In case of such an occurrence, the foreign body should be pushed back down into either one of the lungs to ensure adequate ventilation. If the foreign body displacement occurs during extraction and the patient develops signs of respiratory distress, an immediate RB is usually warranted. RB should always be available on standby just in case any complications occur during FB. Bronchoscopic removal can fail in a few cases and surgical removal may be required.
Learning points.
In few cases, airway foreign body aspiration may go unrecognised due to the absence of acute symptoms at the time of aspiration.
Flexible bronchoscopy is a useful procedure which can allow removal of nearly all types of airway foreign bodies with the aid of a variety of ancillary instruments.
Rigid bronchoscopy is the procedure of choice in the removal of large, impacted foreign bodies and should be the definitive procedure in clinically unstable or hypoxic patients.
Acknowledgments
The authors would like to acknowledge the support from Dr Praveen Aggarwal (Professor and Head, Department of Emergency Medicine, AIIMS, New Delhi, India).
Footnotes
Contributors: KM conducted flexible bronchoscopy. NJ and KM were involved in patient management and follow-up. KM, NJ, ME and RG were involved in the preparation of the manuscript.
Competing interests: None.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Baharloo F, Veyckemans F, Francis C, et al. Tracheobronchial foreign bodies: presentation and management in children and adults. Chest 1999;115:1357–62 [DOI] [PubMed] [Google Scholar]
- 2.Aissaoui A, Salem NH, Chadly A. Unusual foreign body aspiration as a cause of asphyxia in adults: an autopsy case report. Am J Forensic Med Pathol 2012;33:284–5 [DOI] [PubMed] [Google Scholar]
- 3.Nigam BK. Bronchial foreign body masquerading as a lung carcinoma. Indian J Chest Dis Allied Sci 1990;32:43–7 [PubMed] [Google Scholar]
- 4.Boyd M, Chatterjee A, Chiles C, et al. Tracheobronchial foreign body aspiration in adults. South Med J 2009;102:171–4 [DOI] [PubMed] [Google Scholar]
- 5.Mittleman RE, Wetli CV. The fatal cafe coronary. Foreign-body airway obstruction. JAMA 1982;247:1285–8 [PubMed] [Google Scholar]
- 6.Umesan UK, Chua KL, Balakrishnan P. Prevention and management of accidental foreign body ingestion and aspiration in orthodontic practice. Ther Clin Risk Manag 2012;8:245–52 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Madan K, Aggarwal AN, Bhagat H, et al. Acute respiratory failure following traumatic tooth aspiration. BMJ Case Rep 2013;2013:pii: bcr2012008393. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Vishwanath G, Madan K, Bal A, et al. Rigid bronchoscopy and mechanical debulking in the management of central airway tumors: an Indian experience. J Bronchology Interv Pulmonol 2013;20:127–33 [DOI] [PubMed] [Google Scholar]
- 9.Limper AH, Prakash UB. Tracheobronchial foreign bodies in adults. Ann Intern Med 1990;112:604–9 [DOI] [PubMed] [Google Scholar]
- 10.Madan K, Agarwal R, Bal A, et al. Bronchoscopic management of a rare benign endobronchial tumor. Rev Port Pneumol 2012;18:251–4 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Video demonstrating the flexible bronchoscopic denture removal. A snare loop (Olympus, SD-7C1 snare) is employed to encircle around the groove in the denture and once in position, the loop is tightened. Following that, the denture is removed along with the bronchoscope.