

Abstract
Objective:
To develop evidence-based recommendations for complementary and alternative medicine (CAM) in multiple sclerosis (MS).
Methods:
We searched the literature (1970–March 2011; March 2011−September 2013 MEDLINE search), classified articles, and linked recommendations to evidence.
Results and recommendations:
Clinicians might offer oral cannabis extract for spasticity symptoms and pain (excluding central neuropathic pain) (Level A). Clinicians might offer tetrahydrocannabinol for spasticity symptoms and pain (excluding central neuropathic pain) (Level B). Clinicians should counsel patients that these agents are probably ineffective for objective spasticity (short-term)/tremor (Level B) and possibly effective for spasticity and pain (long-term) (Level C). Clinicians might offer Sativex oromucosal cannabinoid spray (nabiximols) for spasticity symptoms, pain, and urinary frequency (Level B). Clinicians should counsel patients that these agents are probably ineffective for objective spasticity/urinary incontinence (Level B). Clinicians might choose not to offer these agents for tremor (Level C). Clinicians might counsel patients that magnetic therapy is probably effective for fatigue and probably ineffective for depression (Level B); fish oil is probably ineffective for relapses, disability, fatigue, MRI lesions, and quality of life (QOL) (Level B); ginkgo biloba is ineffective for cognition (Level A) and possibly effective for fatigue (Level C); reflexology is possibly effective for paresthesia (Level C); Cari Loder regimen is possibly ineffective for disability, symptoms, depression, and fatigue (Level C); and bee sting therapy is possibly ineffective for relapses, disability, fatigue, lesion burden/volume, and health-related QOL (Level C). Cannabinoids may cause adverse effects. Clinicians should exercise caution regarding standardized vs nonstandardized cannabis extracts and overall CAM quality control/nonregulation. Safety/efficacy of other CAM/CAM interaction with MS disease-modifying therapies is unknown.
Complementary and alternative medicine (CAM) therapies are nonconventional therapies used in addition to or instead of physician-recommended therapies. CAM use is prevalent in 33%–80% of patients with MS,1–10 particularly among those who are female, have higher education levels, and report poorer health.1–4,11 This document summarizes extensive information provided in the complete guideline, available as a data supplement on the Neurology® Web site at Neurology.org. Tables e-1 through e-3 and appendices e-1 through e-6, cited in the full guideline (data supplement), as well as references e1–e84, cited in this summary, are available at Neurology.org.
This guideline addresses the following questions: In patients with MS,
do CAM therapies reduce specific symptoms and prevent relapses or disability?
can CAM use worsen MS or cause serious adverse effects (SAEs)?
can CAM use interfere with MS disease-modifying therapies?
DESCRIPTION OF THE ANALYTIC PROCESS
This guideline was developed in accordance with the 2004 American Academy of Neurology (AAN) process manual.12 After review of conflict of interest statements, the AAN selected a panel of experts. A medical research librarian helped perform a comprehensive literature search, and the authors selected articles. At least 2 authors independently rated each article (AAN therapeutic classification scheme). We linked recommendation strength to the evidence quality. With regard to cannabis for pain, we reviewed studies evaluating pain associated with spasticity separately from those evaluating pain specified to be of central neuropathic origin and made separate recommendations. We performed Bonferroni correction for multiple comparisons when necessary.
ANALYSIS OF EVIDENCE
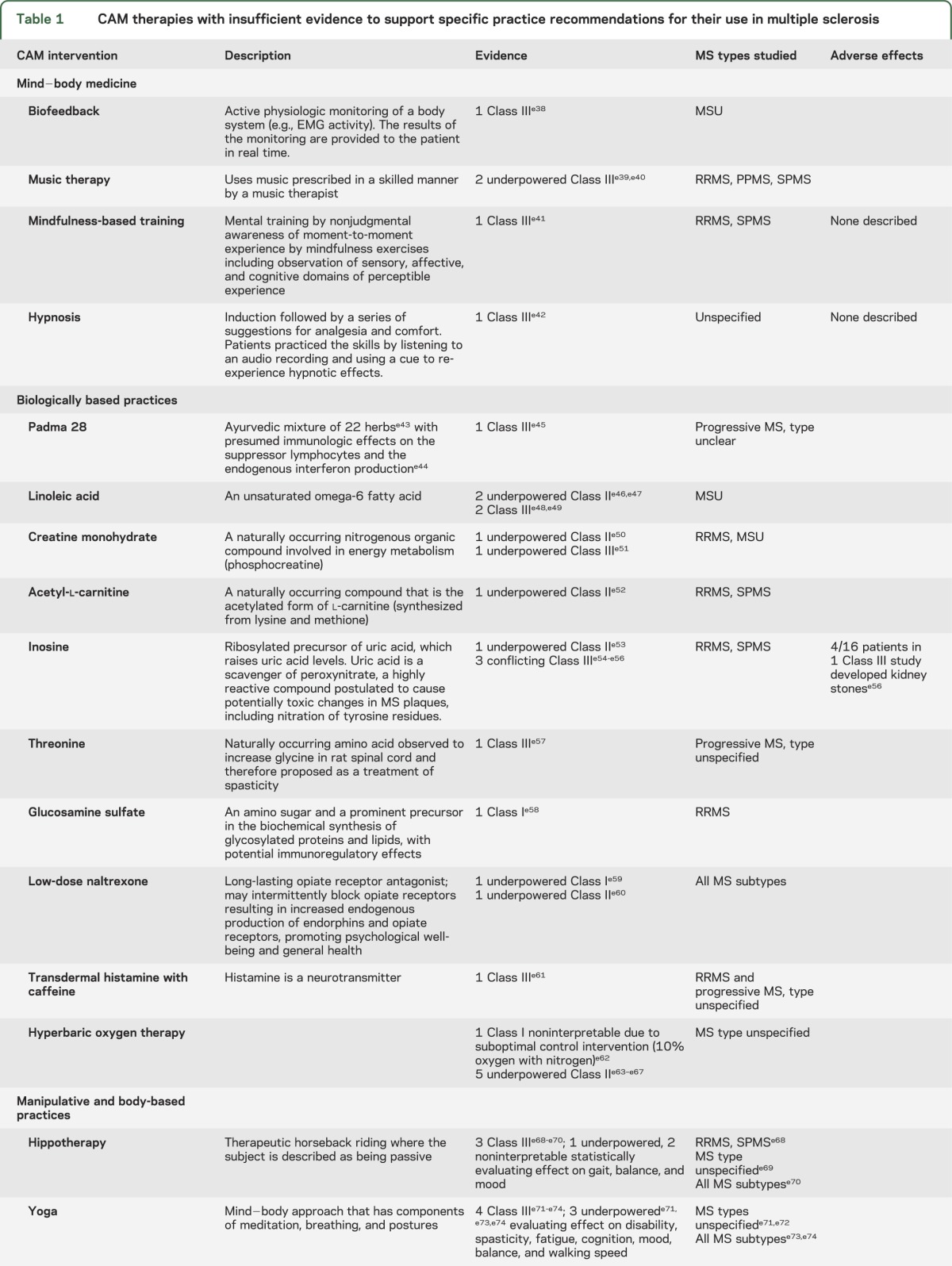
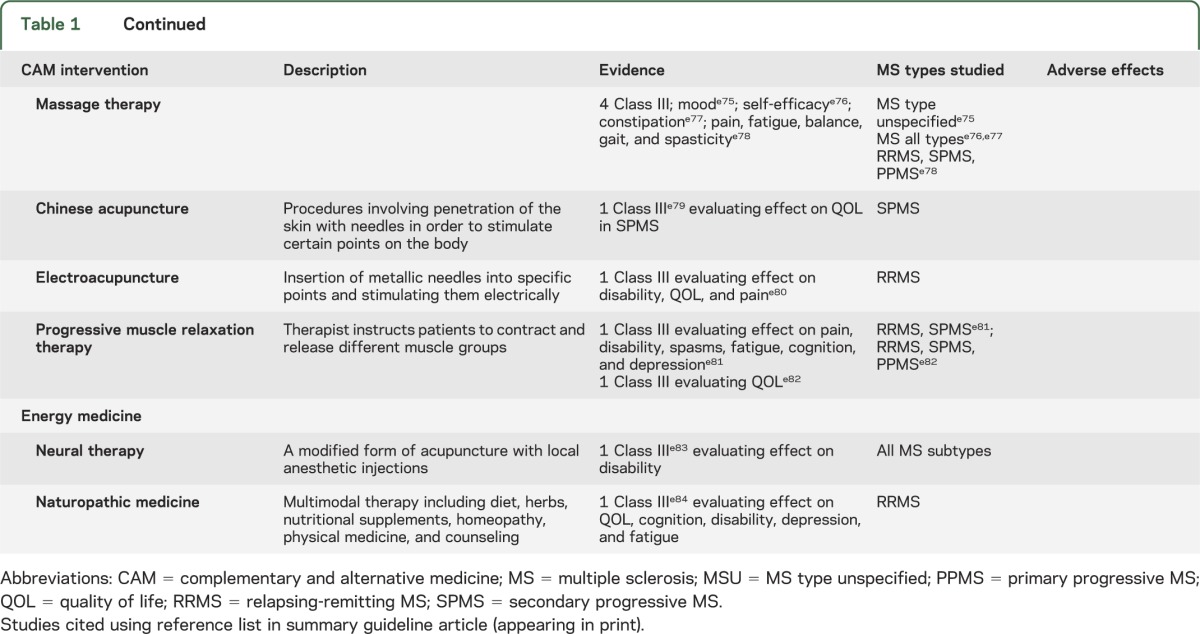
Because studies were unavailable or, where available, had a high risk of bias, were in conflict, or lacked statistical precision, we found the evidence insufficient to support or refute the effectiveness of the following therapies in MS (table 1): acetyl-l-carnitine, acupuncture, biofeedback, carnitine, chelation therapy, Chinese medicine, chiropractic medicine, creatine monohydrate, dental amalgam replacement, glucosamine sulfate, hippotherapy, hyperbaric oxygen, inosine, linoleic acid, low-dose naltrexone, massage therapy, mindfulness training, music therapy, naturopathic medicine, neural therapy, Padma 28, progressive muscle relaxation therapy, tai chi, threonine, transdermal histamine, and yoga. Data also were insufficient to determine whether any CAM therapies worsen MS or interfere with disease-modifying therapies.
Table 1.
CAM therapies with insufficient evidence to support specific practice recommendations for their use in multiple sclerosis
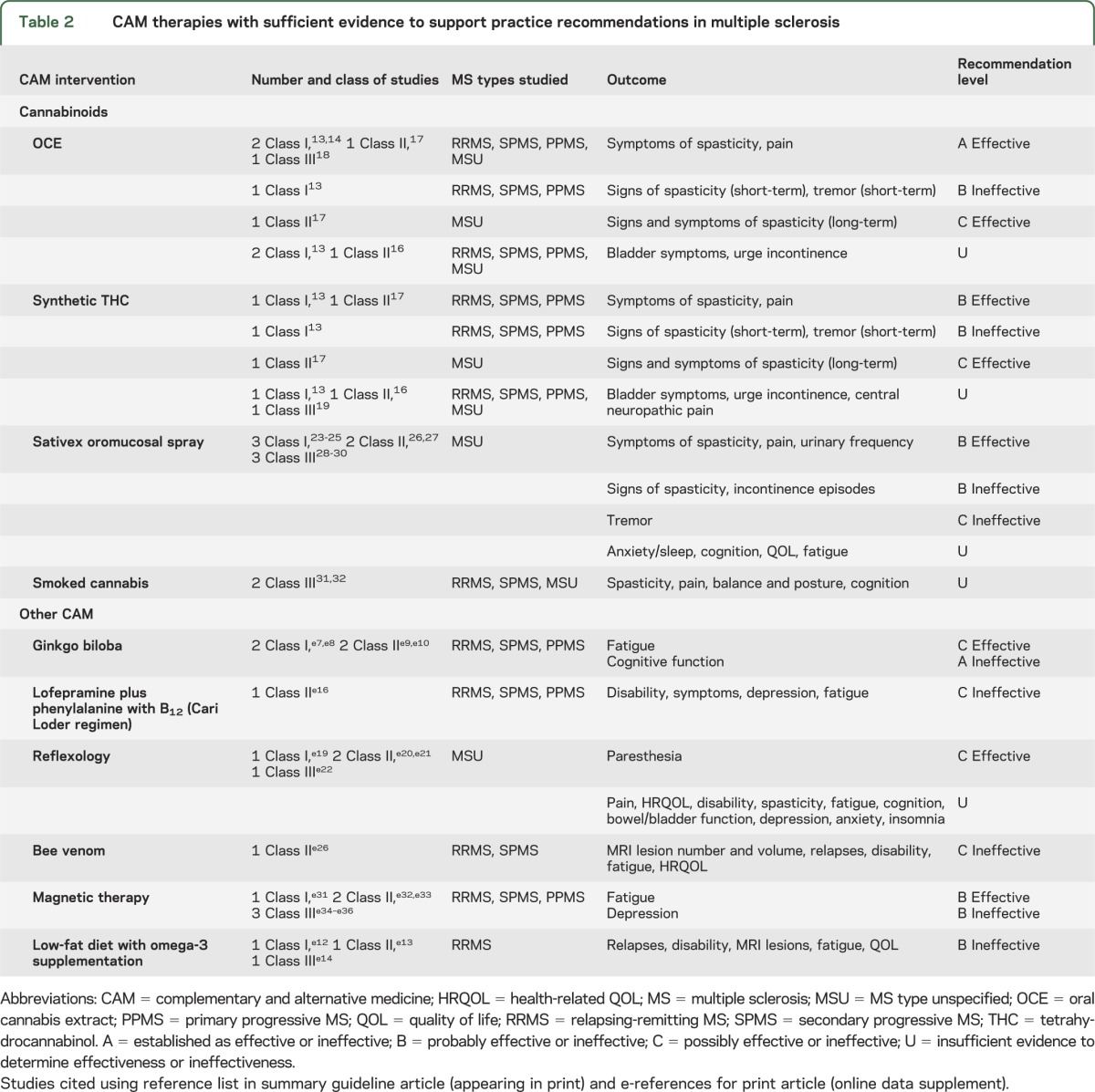
Evidence was available to develop practice recommendations for use of bee venom therapy, cannabinoids, ginkgo biloba (GB), lofepramine plus phenylalanine with B12 (Cari Loder regimen), low-fat diet with omega-3 supplementation, magnetic therapy, and reflexology (table 2). This evidence is discussed herein and includes only the studies that inform the conclusions and recommendations. We selected the final level of obligation for compliance with a recommendation (might/may, should, or must) after taking into consideration the quality of evidence (Level A, B, or C) and other factors (e.g., limited generalizability of the studies, safety/side effect concerns, availability of alternative treatments).
Table 2.
CAM therapies with sufficient evidence to support practice recommendations in multiple sclerosis
Cannabinoids.
Cannabinoids are a group of compounds with psychoactive properties. Tetrahydrocannabinol (THC) and cannabidiol (CBD) are the major cannabinoids of cannabis. Synthetic cannabinoids are chemically related to THC. Orally administered cannabinoids (cannabis extract, synthetic THC), mucosally delivered cannabinoids (cannabis extract oral spray, nabiximols [trade name Sativex]), and smoked cannabis have all been studied for therapeutic effects in MS.
Oral cannabinoids (cannabis extract and THC).
The search identified 9 studies (3 Class I,13–15 2 Class II,16,17 and 4 Class III18–21).
A large Class I study13 (N = 630; patients with relapsing-remitting MS [RRMS], primary progressive MS [PPMS], and secondary progressive MS [SPMS]; 15 weeks) found that neither oral cannabis extract (OCE, THC with CBD) nor synthetic THC (Marinol) had greater effect than placebo on the primary outcome measure of spasticity as measured by total Ashworth scale22 change from baseline (mean change ± SD: OCE: 1.24 [6.60], THC: 1.86 [7.95], placebo: 0.92 [6.56], p = 0.40). However, in this same study,13 significantly more patients reported reduced spasticity symptoms in the treatment groups (secondary outcomes spasticity/pain: OCE [52/46%], THC [51/50%], placebo [37/30%]). Sleep and muscle spasms also improved in the treatment groups.
In a second Class I study14 (N = 249; “stable MS,” type unspecified; 12 weeks) the proportion of patients achieving relief of muscle stiffness was 29.4% in the OCE group compared with 15.7% in the placebo group (odds ratio 2.26, 95% confidence interval [CI] CI 1.24–4.13). Secondary outcomes (muscle stiffness and spasms, pain, sleep) also improved in the cannabis group.
A third Class I study15 (N = 57; RRMS, SPMS, PPMS), insufficiently powered, found no significant difference in objective spasticity (Ashworth scale) or patient-reported spasm frequency.
In both adequately powered Class I studies,13,14 significantly more patients treated with cannabinoids reported reduced pain, whereas disability measures and health questionnaire results were not significantly different between groups. One Class I study13 assessed tremor and bladder symptoms and noted no significant difference in outcomes between patients treated with cannabinoids and placebo.
Conclusions.
OCE is established as effective for reducing patient-reported spasticity symptoms and pain (12–15 weeks; 2 Class I,13,14 1 Class III18). This subjective benefit is possibly maintained for 1 year (1 Class II17).
THC is probably effective for reducing patient-reported symptoms of spasticity and pain (15 weeks, 1 Class I13). This subjective benefit is possibly maintained for 1 year (1 Class II17).
OCE and THC are probably ineffective for reducing both objective spasticity measures and MS-related tremor symptoms (15 weeks, 1 Class I13). OCE and THC are possibly effective for reducing symptoms and objective measures of spasticity over 1 year (1 Class II17).
Sativex oromucosal cannabinoid spray.
The search identified 3 Class I,23–25 2 Class II,26,27 and 3 Class III28–30 studies in patients with MS, type unspecified.
A Class I study, a randomized controlled trial (RCT)23 (N = 160, 6 weeks), evaluated the effect of Sativex spray (GW Pharmaceuticals, Salisbury, UK) delivering THC 2.7 mg and CBD 2.5 mg. Spasticity visual analog scale (VAS) was the only outcome measure on which scores improved significantly after Bonferroni correction (active −31.2, placebo −8.4, difference −22.79, 95% CI −35.52 to −10.07, p = 0.001). Scores on physician-evaluated spasticity measures (Ashworth) did not change between groups.
A Class I RCT24 (N = 66, MS type unspecified, 5 weeks) in MS-related central neuropathic pain found that oromucosal cannabinoids were superior for reducing mean pain intensity (number needed to treat to reduce pain by 50%: 3.7 [95% CI 2.2–13]). Another Class I RCT25 (N = 135, 10 weeks, MS type unspecified) did not find improvement in the number of incontinence episodes with Sativex. However, the daily number of bladder voids (change from baseline: treatment −1.95, placebo −0.9; p = 0.049) decreased significantly.25 A Class II RCT (N = 337, all MS types, 15 weeks)26 observed that tremor did not improve with Sativex.
Conclusions.
Sativex oromucosal cannabinoid spray is probably effective for improving subjective spasticity symptoms (6 weeks, 1 Class I23), pain (5 weeks, 1 Class I24), and urinary frequency (10 weeks, 1 Class I25).
Sativex oromucosal cannabinoid spray is probably ineffective for reducing objective spasticity measures over 6 weeks (1 Class I23) or bladder incontinence episodes over 10 weeks (1 Class I25).
Sativex oromucosal spray is possibly ineffective for reducing MS-related tremor over 15 weeks (1 Class II26).
Smoked cannabis.
We reviewed 2 Class III studies.31,32
One Class III crossover study31 (37 patients, RRMS and SPMS, 2 weeks), reported spasticity reduction (modified Ashworth scale) in the cannabis group (standardized effect size 2.74, 2.2–3.14). Pain, the secondary outcome measure, also improved. After cannabis treatment, the subjects consistently showed reduced cognitive performance (Paced Auditory Serial Addition Test).33
A second Class III study32 (N = 20, MS type unspecified) found that both normal subjects and patients with MS fared worse on measures of posture and balance 10 minutes after smoking 1 marijuana cigarette. After Bonferroni correction, the effect was significant only for patients with MS (p = 0.018).
Conclusions.
Data are inadequate to determine the safety or efficacy of smoked cannabis used for spasticity/pain (1 Class III31), balance/posture (1 Class III32), and cognition (1 Class III31).
Cannabinoid practice recommendations.
Clinicians might offer OCE to patients with MS to reduce patient-reported symptoms of spasticity and pain (excluding central neuropathic pain) (Level A) and might counsel patients that this symptomatic benefit is possibly maintained for 1 year (Level C), although OCE is probably ineffective for improving objective spasticity measures (short-term) or tremor (Level B).
Clinicians might offer THC to patients with MS to reduce patient-reported symptoms of spasticity and pain (excluding central neuropathic pain) (Level B). Clinicians might counsel patients that this symptomatic benefit is possibly maintained for 1 year (Level C), although THC is probably ineffective for improving objective spasticity measures (short-term) or tremor (Level B).
Clinicians might offer Sativex oromucosal cannabinoid spray (nabiximols), where available, to reduce symptoms of spasticity, pain, or urinary frequency, although it is probably ineffective for improving objective spasticity measures or number of urinary incontinence episodes (Level B).
Clinicians might choose not to offer Sativex oromucosal cannabinoid spray to reduce MS-related tremor (Level C).
Data are inadequate to support or refute use of the following in MS (Level U):
OCE/THC for bladder urge incontinence and overall symptoms
Synthetic THC (Marinol) for central neuropathic pain
Sativex oromucosal cannabinoid spray for overall bladder symptoms, anxiety symptoms/sleep problems, cognitive symptoms, quality of life (QOL), and fatigue
Smoked cannabis for spasticity, pain, balance/posture, and cognition
Data are inadequate to determine the abuse potential or effect on psychopathologic symptoms of Sativex cannabinoid spray (Level U).
Clinical context.
The cannabinoid studies have limitations that physicians and patients must be aware of. Most studies were of short duration (6–15 weeks). Another limitation was the potential for central side effects to unmask patients to treatment assignment—a concern with regard to all masked trials involving treatments with prominent side effects. It is also important to recognize that the Ashworth scale used for objective measurement may be insensitive to spasticity changes. These factors may contribute to the discordant effects of cannabinoids on subjective and objective spasticity measures.
Adverse effects.
Cannabinoids were generally well tolerated, although some SAEs were reported. Few studies reported deaths in the cannabinoid-treated groups (1 due to pneumonia,13 1 to seizure-related aspiration pneumonia, and 2 to cancer, presumed unrelated16). Mild/moderate adverse effects (AEs) were common (approximately 50%–80% of subjects) and appeared to be equally prevalent in subjects receiving cannabinoids or placebo. No significant laboratory, hematologic, urologic, or cardiac changes, or differences in vital signs, were noted. CNS AEs (e.g., dizziness, somnolence, drowsiness, lightheadedness, memory disturbance, difficulty concentrating) were more common in subjects receiving cannabinoids vs placebo. Dizziness was most common (15%–50% of subjects).13,15,17,20,21,24–26,28,30 Gastrointestinal AEs, including increased appetite, nausea, vomiting, constipation, and dry/sore mouth, occurred in about 10% of subjects receiving cannabinoids15 and were more common in those receiving cannabinoids than placebo. Other less common AEs included myalgia, increased spasticity, seizures (4/137 subjects had seizures),23 lower limb weakness, hemorrhagic cystitis, dehydration, temporary psychosis (1 rated as severe),21 hallucinations,24 and oral ulceration.23
Because cannabinoids have known psychoactive properties, their potential for psychopathologic and neurocognitive AEs is a concern, especially in a patient population that may be vulnerable due to underlying disorders. Depression and predisposal to psychosis have been reported with long-term cannabis exposure.34–36 Development of marijuana addiction is controversial; however, long-term heavy marijuana use has been associated with tolerance and dependence.37–39 Evidence is also available, albeit inconsistent, for impairments in memory, concentration, and executive functions in chronic cannabis users, although it remains unclear how long these deficits persist after abstinence and whether there is permanent neurotoxicity.40,e1-e3 In 1 study, patients with MS and prolonged use of “street” cannabis had cognitive function impairments relative to patients with MS who did not use cannabis.e4 Patients with MS who smoked cannabis regularly had more extensive cognitive abnormalities and were more likely to meet criteria for a lifetime DSM-IV psychiatric diagnosis.e5 Although not generalizable to medical cannabis, the associations from these studies of street cannabis raise concerns. A substudy of the large Class I study reviewed here,13 available only in abstract form, reported a significant reduction in verbal learning and memory in patients with MS receiving cannabis extracts vs those receiving placebo.e6 Several of the reviewed studies assessed psychopathology and cognition as secondary outcomes without significant AEs; however, these studies were short-term and inadequately powered to exclude an effect.15,21,24,28
Clinicians should therefore counsel patients about the potential for psychopathologic/cognitive and other AEs associated with cannabinoids. Sativex oromucosal cannabinoid spray is not US Food and Drug Administration (FDA) approved and is unavailable in the United States. In the United States, caution should be exercised with regard to extrapolation of results of trials of standardized OCEs (which are unavailable commercially) to other nonstandardized, nonregulated cannabis extracts (which may be commercially available in states with medical marijuana laws).
Ginkgo biloba.
We reviewed 4 studies (2 Class I,e7,e8 2 Class IIe9,e10). A Class I RCT evaluating cognitive function (N = 39; RRMS, SPMS, PPMS) found that subjects taking GB 120 mg twice a day for 12 weeks had a 4.5-second greater (95% CI −7.6–0.9, p = 0.015, nonsignificant [p < 0.008 significant per authors] after Bonferroni correction) improvement in the Stroop Color Word test than those taking placebo.e7 A second Class I study (N = 121; RRMS, PPMS, SPMS, relapsing-progressive MS; 12 weeks) also found no difference in cognition measures with GB 120-mg administration twice a day compared with placebo, confirming the pilot study results.e8
The Class II study (N = 22, all MS types) found significantly greater fatigue reduction with GB 240 mg/day for 4 weeks relative to placebo (Modified Fatigue Impact Scale [MFIS]e11 baseline: GB 37.8 ± 14.7, placebo 39.8 ± 15.1; postintervention: GB 35.5 ± 13.9, placebo 42.4 ± 15.6; p = 0.024).e9 A Class II follow-up analysise10 of the data from this study did not reveal a difference between the GB and placebo groups on visual−spatial memory and attention/concentration.
GB was well tolerated in all studies. No hemorrhagic AEs were reported.
Conclusions.
GB is established as ineffective for improving cognitive function in MS (12 weeks, 2 Class Ie7,e8).
GB is possibly effective over 4 weeks for reducing fatigue in MS (1 Class IIe9).
GB practice recommendations.
Clinicians might counsel patients with MS that GB is established as ineffective for improving cognitive function (Level A).
Clinicians might counsel patients with MS that GB is possibly effective for reducing fatigue (Level C).
Clinical context.
GB and other supplements are not FDA regulated. Their quality control may play a role in their effectiveness and AE risk. Moreover, interactions of supplements with other medications, especially disease-modifying therapies for MS, are a clinical concern.
Low-fat diet with omega-3 fatty acid supplementation (omega-3).
We reviewed 3 studies (1 Class I,e12 1 Class II,e13 and 1 Class IIIe14). The Class I study (RRMS, N = 92) of omega-3 fatty acids (1,350 mg eicosapentaenoic acid and 850 mg docosahexaenoic acid daily) revealed no difference in the cumulative number of gadolinium-enhancing MRI lesions at 6 months, relapse rates at 6 and 24 months, disability progression, fatigue, or QOL.e12
The Class II study (1-year underpowered RCT, N = 27, RRMS)e13 evaluated a low-fat diet supplemented with either omega-3 fatty acid (fish oil) or olive oil. There was no significant difference in health-related QOL (HRQOL), relapse rates, or disability.e13
Conclusion.
A low-fat diet with fish oil supplementation is probably ineffective for reducing MS-related relapse, disability, or MRI lesions, or for improving fatigue or QOL (RRMS, 1 Class I).e12
Omega-3 practice recommendation.
Clinicians might counsel patients that a low-fat diet with fish oil supplementation is probably ineffective for reducing relapses, disability, or MRI lesions, or for improving fatigue or QOL in MS (Level B).
Lofepramine.
Lofepramine (a tricyclic antidepressant structurally related to imipramine and desipramine) combined with l-phenylalanine and IM vitamin B12 is known as the Cari Loder regimen.e15 One 24-week Class II RCT (N = 138, all MS subtypes) compared the Cari Loder regimen with placebo pills and IM vitamin B12 (1 mg weekly).e16 The primary outcome measures of disability did not change significantly (Guy's Neurological Disability Scale [GNDS]e17 −1.16 [95% CI −2.75 to 0.43], Expanded Disability Status Scale [EDSS]e18 −0.17 [95% CI −0.39 to 0.05]). There was a small improvement in fatigue and symptoms, nonsignificant with Bonferroni correction. Depression did not improve.
Conclusion.
The Cari Loder regimen is possibly ineffective for reducing MS-related disability, symptoms, depression, or fatigue (all MS subtypes, 1 Class IIe16).
Lofepramine practice recommendation.
Clinicians might counsel patients with MS that lofepramine plus l-phenylalanine with vitamin B12 (Cari Loder regimen) is possibly ineffective for treating disability, symptoms, depression, or fatigue (Level C).
Reflexology.
Reflexology involves applying manual pressure to points on the feet. We evaluated 4 studies (1 Class I,e19 2 Class II,e20,e21 and 1 Class IIIe22).
The Class I study (underpowered RCT; N = 71; RRMS, SPMS, PPMS) compared 10 weekly 45-minute sessions of sham reflexology (foot massages) with precision reflexology.e19 Both groups showed reductions in pain (VAS), disability (Roland Morris Disability Questionnairee23), spasticity (VAS), fatigue (Multiple Sclerosis Impact Scale [MSIS],e24 Fatigue Severity Scale [FSS], MFIS), and depression (Beck Depression Inventorye25). Differences between groups were nonsignificant.e19
One Class II RCT (MS type unspecified, N = 71) found significantly greater reductions in paresthesia, urinary symptoms, and spasticity (Ashworth Scale) with 11 weekly reflexology treatments plus calf massage relative to calf massage alone.e20 After Bonferroni correction, only the difference in paresthesia reduction remained significant (mean ± SD difference pre-/posttreatment in treated group −1.49 ± 2.1, controls 0.16 ± 2.1; p = 0.04).
Another Class II RCT (underpowered; SPMS, PPMS; N = 20; 16 weeks) of reflexology compared with sham treatments did not reveal improvement in the primary outcome of HRQOL (change in MSIS: 17; 95% CI −4.121 to 40.21, p = 0.112). Secondary outcomes of pain, spasticity, sleep, mood, and bowel/bladder function also did not change.e21
Conclusions.
Reflexology is possibly effective for reducing MS-associated paresthesia over 11 weeks (MS type unspecified, 1 Class IIe20).
Data are inadequate to support or refute the use of reflexology for pain, HRQOL, disability, spasticity, fatigue, cognition, bowel/bladder function, depression, anxiety, or insomnia in MS.
Reflexology practice recommendation.
Clinicians might counsel patients with MS that reflexology is possibly effective for reducing paresthesia (Level C).
Bee venom.
One Class II crossover studye26 of bee venom (20 stings from live bees 3 times weekly for 24 weeks) (N = 26; RRMS, SPMS) found no significant effect on the number of new gadolinium-enhancing lesions on MRI, volume of enhancing lesions, total lesion volume, relapses, disability (EDSS, Multiple Sclerosis Functional Composite,e27 GNDS), fatigue (Shortened Fatigue Questionnaire,e28 Fatigue Impact Scalee29), or HRQOL (Short Form-36e30). AEs included tenderness, swelling, and redness at the sting sites; itching (4 subjects); and flu-like symptoms (5 subjects).e26
Conclusion.
Bee sting therapy is possibly ineffective for reducing MS-related relapses, disability, fatigue, total MRI lesion burden, new gadolinium-enhancing lesion volume, or HRQOL (RRMS, SPMS; 1 Class II).e26
Bee venom practice recommendation.
Clinicians might counsel patients with MS that bee sting therapy is possibly ineffective for reducing relapses, disability, fatigue, total MRI lesion burden, new gadolinium-enhancing lesion volume, or HRQOL (Level C).
Clinical context.
Bee stings can be associated with anaphylactic reaction and possible death.
Magnetic therapy.
The search identified 6 studies (1 Class I,e31 2 Class II,e32,e33 and 3 Class IIIe34-e36).
The Class I 12-week RCT (N = 41, RRMS) reported significantly less fatigue (MFIS) with low-frequency pulsed electromagnetic field therapy (bio-electromagnetic-energy-regulation device, in the form of a metal mat upon which subjects lay for 8 minutes twice a day) (active 26.84 ± SE 12.061, placebo 36.67 ± 13.253; p = 0.024). Fatigue, measured by FSS, a secondary outcome measure, also decreased in the treated group (FSS mean [SD]: placebo 4.7 [1.6], treatment 3.5 [1.3], t = −2.53; p = 0.016). There was no change in depression or disability (EDSS).e31 However, an EDSS change may not have been detected because of the study's short duration (EDSS may be insensitive to change in short-term disability).
A Class II underpowered RCTe32 (N = 30, RRMS/progressive MS) found no significant change after Bonferroni correction in disability (EDSS) or patient-reported performance scale related to bladder control, cognition, fatigue, mobility, sensation, spasticity, vision, total performance, or hand function between subjects wearing wristwatch-size magnetic pulsing devices (Enermed device) (10–24 hours/day for 2 months) or inactive devices.
Another Class II underpowered RCT (N = 50; RRMS, SPMS, PPMS) found no significant difference in fatigue (MFIS, FSS) with low-frequency magnetic stimulation 3 sessions per week for 8 weeks (intensity 37.5 mT and a sequence of pulses at 4–7 Hz).e33 Magnetic therapy was generally well tolerated; most studies reported no AEs.e34,e36 One study reported headache, spasms, and burning sensation.e32
Conclusions.
Magnetic therapy is probably effective for reducing fatigue in RRMS (1 Class I,e31 1 Class IIIe34) and probably ineffective for reducing depression in RRMS over 15 weeks (1 Class Ie31).
Data are inadequate to support or refute the effect of magnetic therapy on reducing MS-related disability (1 Class Ie31 with insensitive outcome measure; 1 underpowered Class IIe32), bladder control problems, or spasticity, or on improving cognition, mobility, sensation, or vision (1 underpowered Class II,e32 3 underpowered/inconsistent Class IIIe34-e36).
Magnetic therapy practice recommendation.
Clinicians might counsel patients with MS that magnetic therapy is probably effective for reducing fatigue (Level B) and probably ineffective for reducing depression (Level B).
Other CAM therapies practice recommendation.
Clinicians should counsel patients with MS that the safety and efficacy of other reviewed CAM, or the interaction of CAM with disease-modifying therapies for MS, are unknown Level U).
LIMITATIONS
This review has several limitations. Because the search strategy is limited only to MS, some potentially important AEs (e.g., bleeding risk with GB)e37 of the reviewed therapies noted when they were evaluated in other diseases were not apparent in the MS population. Therapies that have received much press attention (e.g., dental amalgam removal, transdermal histamine) have little evidence to support recommendations.
Supplementary Material
GLOSSARY
- AAN
American Academy of Neurology
- AE
adverse effect
- CAM
complementary and alternative medicine
- CBD
cannabidiol
- CI
confidence interval
- DSM-IV
Diagnostic and Statistical Manual of Mental Disorders, 4th edition
- EDSS
Expanded Disability Status Scale
- FDA
US Food and Drug Administration
- FSS
Fatigue Severity Scale
- GB
ginkgo biloba
- GNDS
Guy's Neurological Disability Scale
- HRQOL
health-related QOL
- MFIS
Modified Fatigue Impact Scale
- MS
multiple sclerosis
- MSIS
Multiple Sclerosis Impact Scale
- OCE
oral cannabis extract
- PPMS
primary progressive MS
- QOL
quality of life
- RCT
randomized controlled trial
- RRMS
relapsing-remitting MS
- SAE
serious adverse effect
- SPMS
secondary progressive MS
- THC
tetrahydrocannabinol
- VAS
visual analog scale
Footnotes
Supplemental data at Neurology.org
AUTHOR CONTRIBUTIONS
Vijayshree Yadav: study concept and design, acquisition of data, analysis or interpretation of data, drafting/revising the manuscript, critical revision of the manuscript for important intellectual content, study supervision. Christopher Bever, Jr.: study concept and design, acquisition of the data, analysis and interpretation of the data, review of the manuscript for important intellectual content. James Bowen: study concept and design, analysis or interpretation of data, critical revision of the manuscript for important intellectual content. Allen Bowling: study concept and design, analysis or interpretation of data, critical revision of the manuscript for important intellectual content. Bianca Weinstock-Guttman: study concept and design, analysis or interpretation of data, critical revision of the manuscript for important intellectual content. Michelle Cameron: analysis or interpretation of data, critical revision of the manuscript for important intellectual content. Dennis Bourdette: study concept and design, acquisition of data, analysis or interpretation of data, critical revision of the manuscript for important intellectual content, study supervision. Gary Gronseth: study concept and design, acquisition of data, analysis or interpretation of data, drafting/revising the manuscript, critical revision of the manuscript for important intellectual content, study supervision. Pushpa Narayanaswami: study concept and design, acquisition of data, analysis or interpretation of data, drafting/revising the manuscript, critical revision of the manuscript for important intellectual content, study supervision.
STUDY FUNDING
This guideline was developed with financial support from the American Academy of Neurology. None of the authors received reimbursement, honoraria, or stipends for their participation in development of this guideline.
DISCLOSURE
V. Yadav serves as a section editor for Current Neurology and Neuroscience Reports, served as consultant for Bayer Healthcare Pharmaceutical and Biogen Idec, is on the speakers' bureau of Novartis, and receives research support from the McDougall Foundation, National Multiple Sclerosis Society (NMSS) Foundation, Nancy Davis Center Without Walls Foundation, and Biogen Idec. C. Bever received travel funding from the American Academy of Neurology (unrelated to this guideline), the University of Maryland School of Medicine, and the Department of Veterans Affairs; has a patent held or pending for use of hematogenous stem cells in neuronal replacement therapy and gene delivery; has received funding for merit grants from the US Department of Veterans Affairs and a pilot grant from the NMSS; and has received license fee payments and royalty payments (or has contractual rights for receipt of future royalty payments) related to the patent disclosed above. Dr. Bever's spouse has received publishing royalties from Ambulatory Medicine, Barker et al. J. Bowen reports no relevant disclosures. A. Bowling has received funding for travel and honoraria from the Consortium of Multiple Sclerosis Centers, the NMSS, the Multiple Sclerosis Foundation, ProCE, the Center for Disability Services, and the Mandell Center for MS; has received research support from Biogen Idec and Novartis; has consulted for Questcor; and serves on the speakers' bureaus of Acorda, Bayer, Biogen Idec, EMD Serono, Genzyme, Novartis, Pfizer, and Teva Neurosciences. B. Weinstock-Guttman has served on speakers' bureaus and as a consultant for Biogen Idec, Teva Neurosciences, EMD Serono, Pfizer, Novartis, Genzyme, Sanofi, Mylan, and Acorda; and has received grant/research support from the agencies listed above as well as from Questcor and Shire. M. Cameron has received research support from the US Department of Veterans Affairs, the NMSS, the Collins Foundation, Acorda Therapeutics, and the Multiple Sclerosis International Federation and funding for travel and honoraria from the Consortium of Multiple Sclerosis Centers. D. Bourdette has received speaker honoraria and consulting fees from Biogen Idec and Teva Neurosciences, consulting fees from Elan Pharmaceuticals, speaker honoraria from Genzyme, and research grants from the US Department of Veterans Affairs, National Institutes of Health, and NMSS. G. Gronseth and P. Narayanaswami report no relevant disclosures. Go to Neurology.org for full disclosures.
DISCLAIMER
This statement is provided as an educational service of the American Academy of Neurology. It is based on an assessment of current scientific and clinical information. It is not intended to include all possible proper methods of care for a particular neurologic problem or all legitimate criteria for choosing to use a specific procedure. Neither is it intended to exclude any reasonable alternative methodologies. The AAN recognizes that specific patient care decisions are the prerogative of the patient and the physician caring for the patient, based on all of the circumstances involved. The clinical context section is made available in order to place the evidence-based guideline(s) into perspective with current practice habits and challenges. Formal practice recommendations are not intended to replace clinical judgment.
CONFLICT OF INTEREST
The American Academy of Neurology is committed to producing independent, critical and truthful clinical practice guidelines (CPGs). Significant efforts are made to minimize the potential for conflicts of interest to influence the recommendations of this CPG. To the extent possible, the AAN keeps separate those who have a financial stake in the success or failure of the products appraised in the CPGs and the developers of the guidelines. Conflict of interest forms were obtained from all authors and reviewed by an oversight committee prior to project initiation. AAN limits the participation of authors with substantial conflicts of interest. The AAN forbids commercial participation in, or funding of, guideline projects. Drafts of the guideline have been reviewed by at least 3 AAN committees, a network of neurologists, Neurology peer reviewers and representatives from related fields. The AAN Guideline Author Conflict of Interest Policy can be viewed at www.aan.com. For complete information on this process, access the 2004 AAN process manual.12
REFERENCES
- 1.Berkman CS, Pignotti MG, Pamela FC. Use of alternative treatments by people with multiple sclerosis. Neurorehab Neural Re 1999;13:243–254 [Google Scholar]
- 2.Schwartz CE, Laitin E, Brotman S, LaRocca N. Utilization of unconventional treatments by persons with MS: is it alternative or complementary? Neurology 1999;52:626–629 [DOI] [PubMed] [Google Scholar]
- 3.Marrie RA, Hadjmichael O, Vollmer T. Predictors of alternative medicine use by multiple sclerosis patients. Mult Scler 2003;9:461–466 [DOI] [PubMed] [Google Scholar]
- 4.Nayak S, Matheis RJ, Schoenberger NE, Shiflett SC. Use of unconventional therapies by individuals with multiple sclerosis. Clin Rehab 2003;17:181–191 [DOI] [PubMed] [Google Scholar]
- 5.Stuifbergen AK, Harrison TC. Complementary and alternative therapy use in persons with multiple sclerosis. Rehab Nurs 2003;28:141–147 [DOI] [PubMed] [Google Scholar]
- 6.Apel A, Greim B, Zettl UK. How frequently do patients with multiple sclerosis use complementary and alternative medicine? Complement Therapies Med 2005;13:258–263 [DOI] [PubMed] [Google Scholar]
- 7.Apel A, Greim B, Konig N, Zettl UK. Frequency of current utilisation of complementary and alternative medicine by patients with multiple sclerosis. J Neurol 2005;253:1331–1336 [DOI] [PubMed] [Google Scholar]
- 8.Yadav V, Shinto L, Morris C. Use and self reported benefit of complementary and alternative (CAM) therapies among multiple sclerosis patients. Int J MS Care 2006;8:5–10 [Google Scholar]
- 9.Schwarz S, Knorr C, Geiger H. Complementary and alternative medicine for multiple sclerosis. Mult Scler 2008;14:1113–1119 [DOI] [PubMed] [Google Scholar]
- 10.Leong EM, Semple SJ, Angley M, Siebert W, Petkov J, McKinnon RA. Complementary and alternative medicines and dietary interventions in multiple sclerosis: what is being used in South Australia and why? Complement Ther Med 2009;17:216–223 [DOI] [PubMed] [Google Scholar]
- 11.Shinto L, Yadav V, Morris C. Demographic and health-related factors associated with complementary and alternative medicine (CAM) use in multiple sclerosis. Mult Scler 2006;12:94–100 [DOI] [PubMed] [Google Scholar]
- 12.AAN (American Academy of Neurology) Clinical Practice Guideline Process Manual, St Paul, MN: The American Academy of Neurology; 2004 [Google Scholar]
- 13.Zajicek J, Fox P, Sanders H, et al. Cannabinoids for treatment of spasticity and other symptoms related to multiple sclerosis (CAMS study): multicentre randomised placebo-controlled trial. Lancet 2003;362:1517–1526 [DOI] [PubMed] [Google Scholar]
- 14.Zajicek JP, Hobart JC, Slade A, Barnes D, Mattison PG; for MUSEC Research Group Multiple Sclerosis and Extract of Cannabis: results of the MUSEC trial. J Neurol Neurosurg Psychiatry 2012;83:1125–1132 [DOI] [PubMed] [Google Scholar]
- 15.Vaney C, Heinzel-Gutenbrenner M, Jobin P, et al. Efficacy, safety and tolerability of an orally administered cannabis extract in the treatment of spasticity in patients with multiple sclerosis: a randomized, double-blind, placebo-controlled, crossover study. Mult Scler 2004;10:417–424 [DOI] [PubMed] [Google Scholar]
- 16.Freeman RM, Adekanmi O, Waterfield MR, et al. The effect of cannabis on urge incontinence in patients with multiple sclerosis: a multicentre, randomised placebo-controlled trial (CAMS-LUTS). Int Urogynecol J Pelvic Floor Dysfunct 2006;17:636–641 [DOI] [PubMed] [Google Scholar]
- 17.Zajicek JP, Sanders HP, Wright DE, et al. Cannabinoids in multiple sclerosis (CAMS) study: safety and efficacy data for 12 months follow up. J Neurol Neurosurg Psychiatry 2005;76:1664–1669 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Ungerleider JT, Andrysiak T, Fairbanks L, Ellison GW, Myers LW. Delta-9-THC in the treatment of spasticity associated with multiple sclerosis. Adv Alcohol Substance Abuse 1987;7:39–50 [DOI] [PubMed] [Google Scholar]
- 19.Svendsen KB, Jensen TS, Bach FW. Does the cannabinoid dronabinol reduce central pain in multiple sclerosis? Randomised double blind placebo controlled crossover trial. BMJ 2004;329:253. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Fox P, Bain PG, Glickman S, Carroll C, Zajicek J. The effect of cannabis on tremor in patients with multiple sclerosis. Neurology 2004;62:1105–1109 [DOI] [PubMed] [Google Scholar]
- 21.Killestein J, Hoogervorst ELJ, Reif M, et al. Safety, tolerability, and efficacy of orally administered cannabinoids in MS. Neurology 2002;58:1404–1407 [DOI] [PubMed] [Google Scholar]
- 22.Bohannon R, Smith M. Interrater reliability of a modified Ashworth scale of muscle spasticity. Phys Ther 1987;67:206. [DOI] [PubMed] [Google Scholar]
- 23.Wade DT, Makela P, Robson P, House H, Bateman C. Do cannabis-based medicinal extracts have general or specific effects on symptoms in multiple sclerosis? A double-blind, randomized, placebo-controlled study on 160 patients. Mult Scler 2004;10:434–441 [DOI] [PubMed] [Google Scholar]
- 24.Rog DJ, Nurmikko TJ, Friede T, Young CA. Randomized, controlled trial of cannabis-based medicine in central pain in multiple sclerosis. Neurology 2005;65:812–819 [DOI] [PubMed] [Google Scholar]
- 25.Kavia RB, De Ridder D, Constantinescu CS, Stott CG, Fowler CJ. Randomized controlled trial of Sativex to treat detrusor overactivity in multiple sclerosis. Mult Scler 2010;11:1349–1359 [DOI] [PubMed] [Google Scholar]
- 26.Collin C, Davies P, Mutiboko IK, Ratcliffe S; Sativex Spasticity in MS Study Group Randomized controlled trial of cannabis-based medicine in spasticity caused by multiple sclerosis. Eur J Neurol 2007;14:290–296 [DOI] [PubMed] [Google Scholar]
- 27.Collin C, Ehler E, Waberzinek G, et al. A double-blind, randomized, placebo-controlled, parallel-group study of Sativex, in subjects with symptoms of spasticity due to multiple sclerosis. Neurol Res 2010;32:451–459 [DOI] [PubMed] [Google Scholar]
- 28.Wade DT, Makela PM, House H, Bateman C, Robson P. Long-term use of a cannabis-based medicine in the treatment of spasticity and other symptoms in multiple sclerosis. Mult Scler 2006;12:639–645 [DOI] [PubMed] [Google Scholar]
- 29.Aragona M, Onesti E, Tomassini V, et al. Psychopathological and cognitive effects of therapeutic cannabinoids in multiple sclerosis: a double-blind, placebo controlled, crossover study. Clin Neuropharmacol 2009;32:41–47 [DOI] [PubMed] [Google Scholar]
- 30.Centonze D, Mori F, Koch G, et al. Lack of effect of cannabis-based treatment on clinical and laboratory measures in multiple sclerosis. Neurol Sci 2009;30:531–534 [DOI] [PubMed] [Google Scholar]
- 31.Corey-Bloom J, Wolfson T, Gamst A, et al. Smoked cannabis for spasticity in multiple sclerosis: a randomized, placebo-controlled trial. CMAJ 2012;184:1143–1150 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Greenberg HS, Werness SA, Pugh JE, Andrus RO, Anderson DJ, Domino EF. Short-term effects of smoking marijuana on balance in patients with multiple sclerosis and normal volunteers. Clin Pharmacol Ther 1994;55:324–328 [DOI] [PubMed] [Google Scholar]
- 33.Gronwall DM. Paced auditory serial-addition task a measure of recovery from concussion. Percept Mot Skills 1977;44:367–373 [DOI] [PubMed] [Google Scholar]
- 34.Bovasso GB. Cannabis abuse as a risk factor for depressive symptoms. Am J Psychiatry 2001;158:2033–2037 [DOI] [PubMed] [Google Scholar]
- 35.Johns A. Psychiatric effects of cannabis. Br J Psychiatry 2001;178:116–122 [DOI] [PubMed] [Google Scholar]
- 36.Nunez LA, Gurpegui M. Cannabis-induced psychosis: a cross-sectional comparison with acute schizophrenia. Acta Psychiatry Scand 2002;10:173–178 [DOI] [PubMed] [Google Scholar]
- 37.Iversen L. Cannabis and the brain. Brain 2003;126:1252–1270 [DOI] [PubMed] [Google Scholar]
- 38.Budney AJ, Hughes JR, Moore BA, et al. Review of the validity and significance of cannabis withdrawal syndrome. Am J Psychiatry 2004;161:1967–1977 [DOI] [PubMed] [Google Scholar]
- 39.Budney AJ, Hughes JR. The cannabis withdrawal syndrome. Curr Opin Psychiatry 2006;19:233–238 [DOI] [PubMed] [Google Scholar]
- 40.Pope HG, Jr, Gruber AJ, Hudson JI, et al. Neuropsychological performance in long-term cannabis users. Arch Gen Psychiatry 2001;58:909–915 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.