

Abstract
Turner's syndrome also called as Ullrich Turner's syndrome, is a disease of unclear pathogenesis characterized by complete or partial absence of one sex chromosome, with or without cell line mosaicism in a phenotypic female with short stature. Various anomalies result in a constellation of features, of which the most disturbing is primary amenorrhea due to gonadal dysgenesis. Hormone therapy in these patients can often result in successful menstruation, and scope for subsequent pregnancy because of anatomically normal uterus and vagina. Coexisting Mullerian agenesis in these patients can jeopardize the chances of future pregnancy as they have associated structural abnormalities of the uterus and vagina. We report a rare case of middle-aged female with Turner's syndrome and Mullerian agenesis having absent secondary sexual characters and missing uterus with incompletely formed vagina.
KEY WORDS: Mullerian agenesis, mosaicism, Turner's syndrome
INTRODUCTION
Turner's syndrome is a genetic disease with a karyotype of 45, X or 46, XX/45, X (mosaicism) or other structural abnormalities of X chromosomes. It is found in about one in 2,500 female births. The most common age of presentation is between 11 and 15 years, and rarely after 20 years. These cases are characterized by streak ovaries, primary amenorrhea, short stature, and multiple congenital anomalies in a phenotypic female.[1] The development of uterus, fallopian tubes, and vagina are usually normal in Turner's syndrome. We wanted to report this case of Turner's syndrome, who presented with absent uterus and rudimentary vagina, features of Mullerian agenesis; as this association is extremely rare with only few documentations in literature.
CASE REPORT
A 35-year-old female presented with short stature and primary amenorrhea. Her height is 122 cm, weight 34 kg, and she showed fairly normal intelligence. She had a history of delayed milestones and stunted growth. She was born out of consanguineous marriage and her sibling is healthy [Figure 1]. Maternal age at the time of birth of the patient and her sibling is 19 and 25 years, respectively. Physical examination revealed a female phenotype with short stature and cubitus valgus. Her breast and pubic hair development were Tanner's stage I [Figure 2].
Figure 1.

Comparison of height with her normal sibling
Figure 2.

Turner's syndrome patient with short stature, cubitus valgus, and absence of secondary sexual characters
Examination of the cardiovascular, respiratory, and neurological systems is normal. Gynecological examination revealed short vaginal canal with no visible cervix. She was admitted with a provisional diagnosis of Turners's syndrome.
Laboratory investigations revealed normal hematological and biochemical parameters except that her thyroid profile showed low triiodothyronine (T3), thyroxine (T4), and thyroid-stimulating hormone (TSH), suggestive of primary hypothyroidism. Magnetic resonance imaging (MRI) brain revealed normal brain parenchyma and pituitary. Two-dimensional (2D) echocardiography was normal. Her buccal smear was negative for sex chromatin (Barr body). Her pelvic ultrasound revealed absent ovaries, uterus, and cervix. Other organs like kidneys, pancreas, liver, and adrenals were normal. These findings were confirmed by MRI of the pelvis. Even though laparoscopy is the best confirmatory test, it could not be done due to denial of consent. Karyotyping was done which showed 45 chromosomes with one X chromosome missing (45, X) [Figure 3].
Figure 3.
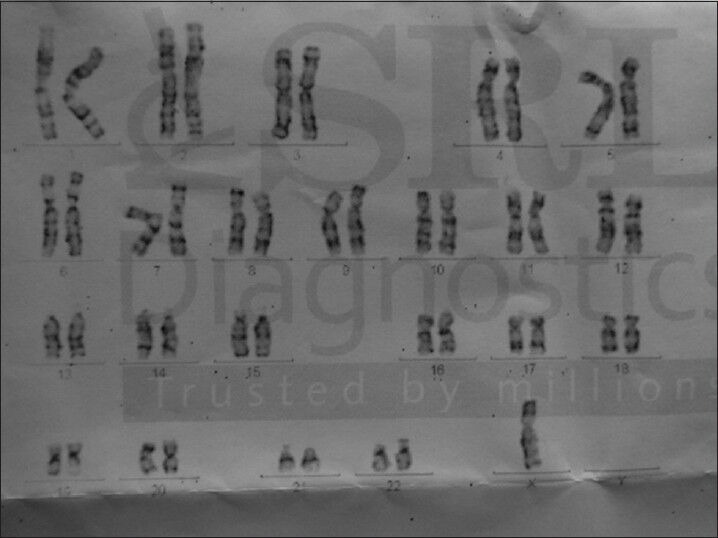
Karyotype of the patient showing single X chromosome (45, XO), that is, monosomy
This karyotype was found in all cells examined, thus confirming the diagnosis of Turner's syndrome.
DISCUSSION
Turner's syndrome is one among the most common causes of primary amenorrhea.[2] Turner's syndrome patients usually present with short stature and have streak or immature ovaries. Other features classically described include cubitus valgus, webbed neck, nail dysplasia, shield-like chest, broadly placed nipples, lymphedema of hands and feet, low set ears, genu valgum, etc., There is no clear association with any established risk factors, maternal age, or familial inheritance pattern. Many cases are associated with renal abnormalities like horseshoe kidney, cardiac abnormalities like coarctation of the aorta, and bicuspid aortic valve.[3] Loss or reduction of germ cells with increased connective tissue in the ovaries often results in severe depletion of sex hormones, leading to primary or secondary amenorrhea. Estrogen therapy in these patients can help in sexual development and bone maturation. In vitro fertilization using donor oocytes has been successfully employed with good pregnancy outcomes. Mullerian agenesis on the other hand presents with normal secondary sexual characters and developmental anomalies of female genital tract including absent/malformed uterus and vagina (Mayer-Rokitansky-Kuster-Hauser syndrome). They have normal female genotype 46, XX and they ovulate normally. They usually present with primary amenorrhea or hypomenorrhea, and pelvic pain due to structural abnormality of female genital tract. With appropriate reconstructive surgeries, these patients can have normal sexual life, but pregnancy is unlikely, unless the uterus is structurally compatible. It is difficult to postulate a common theory for coexistence of these two anomalies in the same patient. It is possible that activating mutation of anti-Mullerian hormone (AMH) gene located on q13 on chromosome 12 might be contributory for the regression of Mullerian duct derivatives like fallopian tubes, uterus, cervix, and upper two-third of vagina in this patient, who is a Turner's phenotype. This combination is a double blow to the patient with very poor chances of conception. In these patients, estrogen therapy can result in the development of breasts and bone growth, but induction of menstruation and subsequent pregnancy is extremely unlikely.
CONCLUSIONS
It is important to consider Turner's syndrome in all cases with short stature and primary amenorrhea. Early diagnosis of the condition might help in sensitizing the caregivers in understanding the importance of instituting hormonal therapy for feminization and bone health during adult life to improve the quality of life. It is also advisable to monitor all individuals with Turner's syndrome for auditory disturbances, thyroid dysfunction, hypertension, diabetes, and dyslipidemia.[4] Very late presentation and unusual combination of Turner's and Mullerian agenesis make this case an interesting one, with cases seldom reported in the literature.[5]
ACKNOWLEDGMENT
We thank the patient and her family for their consent to publish this article.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Achermann, John C. By J. Larry Jameson. 18th ed. Vol. 2. New York: McGraw-Hill, Medical; 2012. “Disorders of Sex Developement.” Harrison's Principles of Internal Medicine; pp. 3046–055. [Google Scholar]
- 2.Bhuyan AK, Sarma D, Saikia UK. Contemporary issues in primary amenorrhea: An experience from a Tertiary Care Center. Indian J Endocrinol Metab. 2012;16:S387–8. doi: 10.4103/2230-8210.104103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Bondy C, Bakalov V, Cheng C, Olivieri L, Rosing D, Arai A. Bicuspid aortic valve and aortic coarctation are linked to deletion of the X chromosome short arm in Turner syndrome. J Med Genet. 2013;50:662. doi: 10.1136/jmedgenet-2013-101720. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Bondy CA. Turner Syndrome Study Group. Care of girls and women with Turner syndrome: A guideline of the Turner Syndrome Study Group. J Clin Endocrinol Metab. 2007;92:10–25. doi: 10.1210/jc.2006-1374. [DOI] [PubMed] [Google Scholar]
- 5.De Leon FD, Hersh JH, Sanfilippo JS, Schikler KN, Yen FF. Gonadal and müllerian duct agenesis in a girl with 46, X, i (Xq) Obstet Gynecol. 1984;63(3 Suppl):81–3S. [PubMed] [Google Scholar]