

Abstract
Background: Use of anabolic androgenic steroids (AAS) has been associated with adverse physical and psychiatric effects and it is known as rising problem among youth people. This study was conducted to evaluate anabolic steroids preventative intervention efficiency among gym users in Iran and theory of planned behaviour was applied as theoretical framework.
Methods: Overall, 120 male gym users participated in this study as intervention and control group. This was a longitudinal randomized pretest - posttest series control group design panel study to implement a behaviour modification based intervention to prevent AAS use. Cross -tabulation and t-test by using SPSS statistical package, version 13 was used for the statistical analysis.
Results: It was found significant improvements in average response for knowledge about side effects of AAS (P<0.001), attitude toward, and intention not to use AAS. Additionally after intervention, the rate of AAS and supplements use was decreased among intervention group.
Conclusion: Comprehensive implementation against AAS abuse among gym users and adolescences would be effective to improve adolescents’ healthy behaviors and intend them not to use AAS.
Keywords: Anabolic steroids, Substance abuse, Theory of planned behavior
Introduction
Recently anabolic steroids use and abuse was known as one of the high-risk behaviours among youth people. Anabolic–androgenic steroids (AAS) are synthetic substances related to the male sex hormones, which endorse growth of skeletal muscles and the development of male sexual characteristics [1].
Over the last decade a number of studies have examined the prevalence of gym users’ use of performance enhancing drugs such as anabolic steroids, clenbuterol and growth hormones [2] as well as why adolescents use these drugs. AAS are used to improve athletic performance, physical attractiveness, increase body weight, fat-free mass, muscle size, and strength when combined with strength training [3]. Numerous studies have identified risk factors for AAS use, including negative body image, younger age, knowing other AAS users, greater time spent on weight lifting, greater awareness of the effects of AAS use, and other illicit drug use [4-5].
The most common debates against AAS use begin with the arguments on side effects of AAS that threats adolescents. Many of the substances used by athletes and adolescents to enhance performance carry significant critical risks, including a risk of death [6]. Additionally; AAS use has been associated with a wide range of physical and psychiatric complications including atrial fibrillation [7], skin lesions such as severe acne and abscess at site of injection, edema, cardiac palpitations, decreased fertility, and sexual dysfunction [8], changes in lipoprotein fraction, increased triglyceride levels, increased concentrations of several clotting factors, changes in the myocardium such as increased left ventricular mass and dilated cardiomyopathy and hyperinsulinism and diminished glucose tolerance [9]. Psychiatric side effects, such as hypomania, mania, or major depression have also been associated with AASs [10]. In addition to increased aggressiveness, there have also been reports of violent behavior and there are evidences suggesting an enhanced risk of unnatural death by committing suicide or being the victim of homicide [1]. Additionally, AAS have also been linked to the abuse of alcohol, morphine, and other addictive substances [11].
The use of non-prescribed AAS spread among some athletes in the 1950s and consequently extend to adolescents and young adults who train for aesthetic reasons in the early 1980s [12-13] and poly-substance abusers [14-15]. It is estimated that one in five American athletes are using one form or another of AAS [16]. Iran is one of many countries where prevalence of AAS use is increasing, especially among youth people who desire to have muscular body by physical training. Recent studies among large samples of youth who were training as gym users and body builders in Iran reported that approximately 13% of gym population [17] and 18.8 % [18] had ever used AAS. Kashi et al [19] reported that 63.3% of athletes in Iran at least have used ASS one time in their life. In addition, study of Kargarfard et al [20] on university students in Isfahan showed that 8.3 % had used ASS in their long life.
The worldwide magnitude of AAS use as well as Iran indicate necessity of designing comprehensive and effective interventions to prevent AASs use and abuse among athletes and more especially among adolescents and youth population who exercise in the gym salons. In the field of drug abuse prevention research, it would be useful to know how cognitive related factors like knowledge, social norms, or beliefs are responsible to predict intention and consequently behavior [21]. In addition to sufficient information, certain psychosocial factors, such as attitude, subjective norm, and perceived behavioral control, seem to be significant factors in determining the probability of adopting or rejecting a healthy behavior. In this regard, the theories of planned behavior in numerous studies as a research theoretical framework were applied; and several studies have reported TPB variables’ predictability to explain anabolic steroid use among athletes [22-24]. This theory postulates that behavioral intention, which is the immediate predictor of AAS use, correlate to attitudes/beliefs regarding AAS use and its users, subjective norms about AAS use among peers, and perceived behavioral control to abstain AAS use [21]. (Fig. 1.)
Fig 1 .
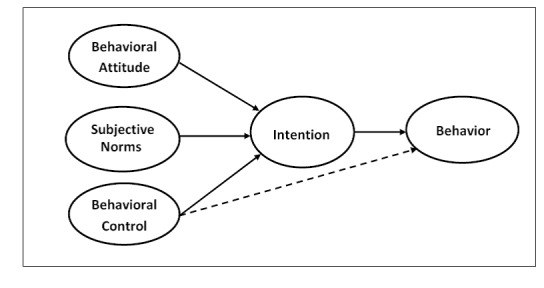
Theory of Planned Behavior
In spite of the increased prevalence of AAS use in Iran, no theoretically based preventative program against AAS use among Iranian adolescents was found in the literature. Based on the abovementioned background, the objective of this study was designing and implementing a peer based educational intervention to increase awareness about side effects of AAS components and consequently prevent and reduce anabolic-steroid use among male gym users based on theory of planned behavior.
Materials and Methods
Participants
This study was conducted among young male gym users in Hamadan city during 2008–2009. Two body building club randomly selected within all male bodybuilding cubs in Hamadan, Iran. Of the 260 gym users enrolled at the two bodybuilding clubs, 120 (46.15%) male participated in this study. Sixty participants as intervention and 60 as control groups were enrolled at the baseline survey, of who all were followed up after 2-month intervention. This study was conducted with approval from Hamadan University of Medical sciences’ institutional review board. Informed assent and consent were obtained from participants.
Measures
Prior to conducting the main project, a pilot study was carried out. Initially the relevant questionnaires were administered to 30 body builders who were similar to participants in the main study to obtain feedback about the clarity, length comprehensiveness, time of completion, and internal reliability of the measures. Moreover, participants were instructed about how to fill questioners before gathering information.
Demographics
Background data collected in this research include: age, literacy (elementary; secondary; high school; and university), marital status (single; married), having coach who use AAS (yes/no), having friends who had history of AAS use (yes/no), duration of exercises in gym saloon (per months), history of smoking (yes/no), alcohol (yes/no). In addition, the participants were asked to describe motivation to use AAS, including (to grow stronger”, “to perform better in athletics”, “to get a muscular body”, “to be attractiveness by others”).
AAS Use
The AAS Survey consisted of four questions that addressed the specific compounds used, history of AAS use, and sport supplement use (yes/no), and type of used supplement.
TPB Theoretical Variables
The items which assessed components of the TPB were modified from scales of AAS related attitudes and intention to use Housman [23]; Bering [24] for AAS use and 18 items were composed under four major constructs, 1) attitude towards AAS; 2) subjective norms about AAS; 3) perceived behavioral control; 4) behavioral intention to AAS use. Six items were designed to measure attitude toward use of AAS (e.g., “If I were to use anabolic steroid it would help me to improve sports performance”). Four items were designed to measure subjective norms toward use of AAS (e.g., “If I use of anabolic steroid my coach it will confirm”). Four items were designed to perceived behavioral control not to use of AAS (e.g., “I believe that I can manage myself against pressure to use of anabolic steroid”). Four items were designed to evaluate behavior intention to AAS use (e.g., “I intend to use anabolic steroid to improve my physical performance in the next 6 months”). In order to facilitate respondents’ responses to the items, all items were standardized to a 5-point Likert scale, ranging from 1 (strongly disagree) to 5 (strongly agree). Estimated reliability coefficients for each TPB constructs questionnaire were as follows: attitude (α = 0.82); subjective norms (α = 0.78); perceived behavior control (α = 0.73) and behavioral intention (α = 0.92). These results demonstrated that questionnaires were internally consistent.
Knowledge about side effects of AASs
Gym users’ awareness about the AASs’ side effects was measured by an 18 items scale. Example of items included:
AASs increase probability of aggressiveness; and
Infertility is one of the side effects of AASs use.
Procedure
This was a longitudinal randomized pretest - posttest series control group design panel study to implement a health education based intervention to prevent and reduce AAS use among a sample of young male gym users recruited from two randomly selected body building club in Hamadan, Iran. After obtaining informed consent participants were enrolled in the study, a 50-item, structured questionnaire with the aforementioned measures was distributed to the athletes to complete. Prior to the self-administration of the questionnaire, study staff explained the logistics of answering different type of questions and clarified any concerns and questions that were raised by participants.
The intervention aimed to provide participants with refusal skills against AAS use. The intervention activates were tailored and implemented based on athletes educational needs, proper nutrition, and training resistance using group discussion, printed leaflet, and audio-visual CD. Additionally, the program also aimed increase participants knowledge with a focus on side effects of AAS abuse. For achieving effective preventative program, the six 1 hour-session was conducted based on health educational programs at the gym salons. Furthermore, prior to intervention four participants who were commitment to mediate AAS prevention program’s message to gym users in the intervention group, were selected as the mediator; any of them had experience in body building clubs for 4 to 11 years. Consequently, four subgroups were formed as intervention group that were coordinated by one responsible mediator.
Statistical Analysis
Analyses were conducted by using SPSS-13 and a probability level of 0.05 was used throughout. Cross -tabulation and t-test were employed to determine comparability of the intervention in compare with control group.
Results
The participants’ ages ranged from 15 to 43 years, with the mean (SD) age of all participants being 23.68(±SD:4.46) years. Of the 26.7% of participants were younger that 20 and 5.8% older than 31 years. Vast majority of participants (44.2%) were 21-25 years, and those 26-30 years (23.3%). Of all respondents, 4.2% reported using of testosterone (4.2%). Consequently, anadrol (3.3%), dianabol (1.7%), durabolin (0.8%) and oxandrolone (3.3%), methyl testosterone (3.3%), nandrolone (1.7%) were the next AAS components. Concerning average length of gym practice among participants it was ranged 11- 120 months with the mean 27.15 (±SD:2.21).
At baseline, 20% of gym users reported that they had used AAS components. Participants also reported that 53.3% of their friends ha d used AAS and about 48.3% of them reported that their coach have used AAS. Additionally Table 1 shows frequency of AAS use among participants for age, overweight, duration of gym practice, AAS use among gym users, their friends, their coach, history of alcohol use, history of smoking and use of supplements in the both intervention and control groups. Cross-tabulation analysis revealed that there were not significant differences between two Intervention and control groups before implementation of AAS prevention educational program (X2:0.653, d.f:1.p:684). These results revealed homogeneity of participants.
Table 1. Pretest Equivalency results for Intervention (n=60) and Control groups (n=60) .
| Variables | Intervention Group | Control Grou | P -value |
| Age | Mean (±SD) 24.35 (5.46) | Mean (±SD) 23.01 (3.08) | 0.102 |
| Length of gym practice (Months) | 25.85 (24.00) | 28.45 (20.22) | 0.522 |
| Overweight (kg) | 77.63 (13.19) | 81.90 (15.50) | 0.107 |
| Previous history of AASs use | n (%) 19 (31.66) | n (%) 26 (43.33) | 0.187 |
| Current AAS use | 11 (18.33) | 13 (21.66) | 0.648 |
| Having AAS user coach | 24 (40) | 34 (56.66) | 0.068 |
| Having AAS user friends | 31 (51.66) | 33 (55) | 0.714 |
| History of alcohol use | 12 (20) | 18 (30) | 0.206 |
| History of Smoking | 8 (13.33) | 10 (16.66) | 0.609 |
| Consumption of supplements | 44 (73.33) | 50 (83.33) | 0.184 |
Table 2 indicates that there are significant improvements in average response for independent variables among gym users who were under intervention. As it shown in table average response for positive attitude towards AAS was 18.25 that it was decreased to 14.36 after intervention. The same results was found for knowledge about side effects of AAS and average response was improved from 6.83 to 11.38 after implementing educational program. Additionally average response to intention to AAS use was 8.38 that it was decreased to 6.75 after intervention. However, it was not found significant improvement for score of subjective norms about AAS and Perceived behavioral control.
Table 2. Average Responses for TPB variables and Knowledge about side effects of AAS Before and After Educational Program.
| Independent Variables | Before Intervention Mean (±SD) | After Intervention Mean (±SD) | P -value |
| Knowledge | |||
| Intervention group | 6.83 (4.55) | 11.38 (2.88) | 0.000 |
| Control group | 7.08 (3.98) | 7.93 (3.27) | 0.045 |
| Attitude towards AAS | |||
| Intervention group | 18.35 (5.02) | 14.26 (5.06) | 0.000 |
| Control group | 18.50 (5.62) | 17.61 (3.84) | 0.014 |
| Behavioral intention to AAS use | |||
| Intervention group | 8.38 (3.92) | 6.75 (3.25) | 0.000 |
| Control group | 9.06 (4.05) | 8.96 (4.16) | 0.600 |
| Perceived behavior control | |||
| Intervention group | 15.08 (3.84) | 15.90 (2.72) | 0.005 |
| Control group | 14.53 (3.31) | 14.66 (3.77) | 0.398 |
| Subjective norms | |||
| Intervention group | 10.61 (3.85) | 10.10 (3.42) | 0.082 |
| Control group | 11.11 (3.86) | 11.56 (3.67) | 0.088 |
| Intention AAS use | |||
| Intervention group Control group | 8.83 (3.95) | 6.75(3.25) | 0.000 |
| 9.06 (4.05) | 8.96 (4.16) |
Intervention group (n=60), Control group (n=60)
To assess efficiency of AAS preventative program cross-tabulation analysis was performed. Despite the results did not show significant relation between efficiency AAS preventative educational intervention, it was found improvement in gym users’ behavior not to use AAS in the past 2 months AS it shown in Table 3 the percent of AAS use in the intervention group was 18.3% that it was decreased to 10% after intervention. Additionally, Tables 3 show supplement use before and after training in two groups.
Table 3. Anabolic Steroid Abuse and Supplement use before and after training in two groups.
| Variables | Before Intervention n (%) | After Intervention n (%) | X2 | P -value |
| AAS use | ||||
| Intervention group Control group | 11 (18.33) | 6 (10) | 1.713 | 0.191 |
| 13 (21.66) | 11 (18.33) | 0.283 | 0.648 | |
| Supplement use | ||||
| Intervention group Control group | 44 (73.33) | 41 (68.33) | 5.783 | 0.016 |
| 50 (83.33) | 52 (86.66) | 1.768 | 0.184 |
Intervention group (n=60), Control group (n=60)
Discussion
The aim of this study was to assess the effectiveness of an anabolic steroid abuse prevention program based on improving gym practices without using AAS components. The theory of planned behavior was conducted as theoretical framework to assess educational need assessment among male participants. Even though the duration of the educational intervention in this study was short, it was found significant improvements after manipulation. Analysis of the baseline and 2- months follow-up clearly demonstrated significant intervention effects on the participants’ attitude, Intention as well as their knowledge about side effects of anabolic steroid among intervention group.
Although there are many factors that affect on human behavior our findings indicated that improving knowledge about side effects of AAS had effective role to reduce rate of AAS use among intervention group. Allahverdipour et al declared that knowledge about side effects of drugs and improving resistance skills can protect adolescents against drug abuse [25]. Additionally, along knowledge, changing beliefs about AAS components and knowing what kinds of beliefs might be effective factor to implementing AAS prevention program would be important to promote healthy behaviors. Our findings showed that the applied AAS prevention program had significant effect to modify participants’ beliefs against AAS components and AAS use. Despite theoretical frame work of TPB, which attitude, subjective norms and perceived behavioral control affect on behavioral intention, our findings showed that education program could not improve average response for participants’ subjective norms against AAS and their perceived behavioral control. While, participants average response for behavioral intention not to use AAS components significantly increased after intervention. It seems more study are needed about predictability of subjective norms and perceived behavioral control on behavioral intention in different cultures and populations.
Concerning efficiency of intervention, in spite of decreasing the rate of AAS use after intervention it was not found significant differences between intervention and control groups and these outcomes is not consistent with similar studies [26-29]. Non significant reduction in AAS use after intervention between both intervention and control groups could be because of low sample size, limitation of resource to design comprehensive educational program, and peer pressure to continue AAS use.
Nilsson et al indicated that designing strategy to reduce the use of ASS among youth is a difficult issue [28] and even some studies have shown that the misuse of AAS increased after educational programs [30,31]. Evidences from other researches confirm our findings about applying health education programs to prevent AAS use among adolescents and gym users [26-29]. In consistent to objectives of this study, numerous studies [32,33] reported that low awareness and inappropriate beliefs are important reasons for using substances.
Conclusion
Overall, findings of the current study supported that implementing AAS abuse preventative program among gym users and adolescences would be effective to improve resistance skills not to use AAS. Although the present study has several strengths, such as theory driven, interventional study, psychometrically sound measures and high response rate of the study participants, the study are limited due to the homogenous sample and self-reported questionnaires (there is a possibility of misreporting). Future studies in this context may also support our findings by sampling female gym users and diverse population.
Acknowledgments
This research was supported by the Deputy of Research and Research Center for Drug Dependency and Behavioral Disorders of Hamadan University of Medical Sciences, Iran. The authors declare that there is no conflict of interests.
References
- [1].Lundholm L, Käll K, Wallin S, Thiblin I. Use of anabolic androgenic steroids in substance abusers arrested for crime. Drug Alcohol Depend. 2010;111(3):222–26. doi: 10.1016/j.drugalcdep.2010.04.020. [DOI] [PubMed] [Google Scholar]
- [2].Wiefferink CH, Detmar SB, Coumans B, Vogels T, Paulussen TG. Social psychological determinants of the use of performance-enhancing drugs by gym users. Health Educ Res. 2008;23(1):70–80. doi: 10.1093/her/cym004. [DOI] [PubMed] [Google Scholar]
- [3].Amsterdam JV, Opperhuizen A, Hartgens F. Adverse health effects of anabolic–androgenic steroids. Regul Toxicol Pharmacol. 2010;57(1):117–23. doi: 10.1016/j.yrtph.2010.02.001. [DOI] [PubMed] [Google Scholar]
- [4].Brower KJ, Blow FC, Hill EM. Risk factors for anabolic-androgenic steroid use in men. J Psychiatr Res. 1994;28(4):369–80. doi: 10.1016/0022-3956(94)90019-1. [DOI] [PubMed] [Google Scholar]
- [5].Bahrke MS, Yesalis CE, Kopstein AN, Stephens JA. Risk factors associated with anabolic-androgenic steroid use among adolescents. Sports Med. 2000;29(6):397–405. doi: 10.2165/00007256-200029060-00003. [DOI] [PubMed] [Google Scholar]
- [6].Kious BM. Philosophy on steroids: why the anti-doping position could use a little enhancement. Theor Med Bioeth. 2008;29(4):213–34. doi: 10.1007/s11017-008-9078-9. [DOI] [PubMed] [Google Scholar]
- [7].Liu T, Shehata M, Li G, Wang X. Androgens and atrial fibrillation: Friends or foes? Int J Cardiol. 2010;142(1):8–14. doi: 10.1016/j.ijcard.2010.02.039. [DOI] [PubMed] [Google Scholar]
- [8].Quaglio G, Fornasiero A, Mezzelani P, Moreschini S, Lugoboni F, Lechi A. Anabolic steroids: dependence and complications of chronic use. Intern Emerg Med. 2009;4(4):289–96. doi: 10.1007/s11739-009-0260-5. [DOI] [PubMed] [Google Scholar]
- [9].Bahrke MS, Yesalis CE. Abuse of anabolic androgenic steroids and related substances in sport and exercise. Curr Opin Pharmacol. 2004;4(6):614–20. doi: 10.1016/j.coph.2004.05.006. [DOI] [PubMed] [Google Scholar]
- [10].Thiblin I, Parlklo T. Anabolic androgenic steroids and violence. Acta Psychiatr Scand Suppl. 2002;(412):125–28. doi: 10.1034/j.1600-0447.106.s412.27.x. [DOI] [PubMed] [Google Scholar]
- [11].Lovestakken K, Peterson L, Homer AL. Risk factors for anabolic steroid use in college students and the role of expectancy. Addict Behav. 1999;24(3):425–30. doi: 10.1016/s0306-4603(98)00060-4. [DOI] [PubMed] [Google Scholar]
- [12].Nilsson S, Spak F, Marklund B, Baigi A, Allebeck P. Attitudes and behaviors with regards to androgenic anabolic steroids among male adolescents in a county of Sweden. Subst Use Misuse. 2005;40(1):1–12. doi: 10.1081/ja-200030485. [DOI] [PubMed] [Google Scholar]
- [13].Parkinson AB, Evans NA. Anabolic androgenic steroids: a survey of 500 users. Med Sci Sports Exerc. 2006;38(4):644–51. doi: 10.1249/01.mss.0000210194.56834.5d. [DOI] [PubMed] [Google Scholar]
- [14].Kanayama G, Hudson JI, Pope Jr HG. Features of men with anabolic- androgenic steroid dependence: a comparison with nondependent AAS users and with AAS nonusers. Drug Alcohol Depend. 2009;102(1):130–37. doi: 10.1016/j.drugalcdep.2009.02.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [15].Skarberg K, Nyberg F, Engstrom I. Multisubstance use as a feature of addiction to anabolic-androgenic steroids. Eur Addict Res. 2009;15(2):99–106. doi: 10.1159/000199045. [DOI] [PubMed] [Google Scholar]
- [16].Hall RC, Hall RC. Abuse of supraphysiologic doses of anabolic steroids. South Med J. 2005;98(5):550–55. doi: 10.1097/01.SMJ.0000157531.04472.B2. [DOI] [PubMed] [Google Scholar]
- [17].Nojoumi M, Behravan V. Study of Anabolic Steroids and the Awareness of their Complications in Bodybuilding Athletes in Karaj. Journal of Iran University of Medical Sciences. 2005;11(44):1057–63. (Persian). [Google Scholar]
- [18].Sepehri GH, Moosavifar M. The frequency of anabolic steroid abuse in bodybuilder athletes in Kerman city. Journal of Rafsanjan University of Medical Sciences. 2003;2(3):213–21. [PMC free article] [PubMed] [Google Scholar]
- [19].Kashi A, Kargarfard M, Moulavi H. Ergogenic substance in body building athletes: prevalence, cognitive and awareness of about their side effects. Olympic. 2006;14(2):73–86. [Google Scholar]
- [20].Kargarfard M, Ghias M, Karim-Zadegan AR, Kashi A. Assumption of Anabolic-androgenic Steroids among Isfahan University Students: Prevalence and Awareness about Their Side Effects. The Quarterly Journal of Fundamentals of Mental Health. 2006;8(31&32):73–80. (Persian). [Google Scholar]
- [21].MacKinnon DP, Goldberg L, Clarke GN, Elliot DL, Cheong JW, Lapin A. et al. Mediating Mechanisms in a Program to Reduce Intentions to Use Anabolic Steroids and Improve Exercise Self-Efficacy and Dietary Behavior. Prev Sci. 2001;2(1):15–28. doi: 10.1023/a:1010082828000. [DOI] [PubMed] [Google Scholar]
- [22].Dodge T, Jaccard JJ. Is abstinence an alternative? Predicting adolescent athletes' intentions to use performance enhancing substances. J Health Psychol. 2008;13(5):703–11. doi: 10.1177/1359105307082460. [DOI] [PubMed] [Google Scholar]
- [23]. Housman JM. Understanding female collegiate athletes' intentions to consume sport supplements: an application of the theory of planned behavior. Submitted to the Office of Graduate Studies of Texas A&M University in partial fulfillment of the requirements for the degree of doctor of philosophy in health education. Available at: http://repository.tamu.edu/bitstream/handle/1969.1/5808/etd-tamu-2006A-HEED-Housman.pdf?sequence=1
- [24]. Berning JM. Characteristics, attitu-des, and normative factors of anabolic steroid use among college-aged males and females: An applic-ation of the theory of reasoned action. Presented to the Faculty of the gradate college at the university of Nebraska in partial fulfillment of requirements for the degree of doctor of philosophy. Available at: http://digitalcommons.unl.edu/dissertations/2003/AAI3092528
- [25].Allahverdipour H, Bazargan M, Farhadinasab A, Hidarnia A, Bashir-ian S. Effectiveness of skill-based substance abuse intervention among male adolescents in an Islamic coun-try case of the republic of Iran. J Drug Education. 2009;39(2):211–22. doi: 10.2190/DE.39.2.g. [DOI] [PubMed] [Google Scholar]
- [26].Goldberg L, Elliot D, Clarke GN, MacKinnon DP, Moe E. et al. Effects of a multidimensional anabolic steroid prevention intervention: The Adolescents Training and Learning to Avoid Steroids (ATLAS) program. JAMA. 1996;276(19):1555–62. [PubMed] [Google Scholar]
- [27].Ranby KW, Aiken LS, MacKinnon DP, Elliot DL, Moe EL. et al. Mediation Analysis of the ATHENA Intervention for Female Athletes: Prevention of Athletic-Enhancing Substance Use and Unhealthy Weight Loss Behaviors. J Pediatr Psychol. 2006;34(10):1069–83. doi: 10.1093/jpepsy/jsp025. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [28].Nilsson S, Allebeck P, Marklund B, Baigiand A, Fridlund B. Evaluation of a health promotion program to prevent the misuse of androgenic anabolic steroids among Swedish adolescents. Health Promot Int. 2004;19(1):61–67. doi: 10.1093/heapro/dah108. [DOI] [PubMed] [Google Scholar]
- [29].Rahimi MA, Siabani H, Siabani S, Rezaei M, Abbasi MR. Effect of Education on Performance-enhancing Drug Abuse by Bodybuilders. Behbood, the Scientific Quarterly. 2006;14(1):26–37. (Persian). [Google Scholar]
- [30].Goldberg L, Bents RT, Bosworth EE, Trevisan L, Elliot DL. Effect of an anabolic steroid education program on knowledge and attitudes of high school football players. J Adolesc Health Care. 1990;11(3):210–14. doi: 10.1016/0197-0070(90)90350-b. [DOI] [PubMed] [Google Scholar]
- [31].Goldberg L, Bosworth EE, Bents RT, Trevisan L. Anabolic steroid education and adolescents: do scare tactics work? Journal of Pediatrics. 1991;87(3):283–86. [PubMed] [Google Scholar]
- [32].Laure P, Binsinger C, Lecerf T. General practitioners and doping in sports: attitude and experience . Br J Sports Med. 2003;37(4):335–38. doi: 10.1136/bjsm.37.4.335. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [33].Randall RW, Grage M, Rodrigo A. Anabolic steroids and pre adolescent athletic: Prevalence, knowledge and attitude. The Sport Journal. 2002;5(3):1–11. [Google Scholar]