

Abstract
Background: According to the findings of several studies conducted on work-related musculoskeletal disorders (WMSDs) among the video display terminals (VDTs) users, Prevention of these disorders among this population is a challenge for many workplaces today. Ergonomically Improving of VDT workstations may be an effective and applicable way to decrease the risk of WMSDs. This study evaluated the effect of an ergonomics-training program on the risk of WMSDs among VDT users.
Methods: This study was conducted among a large group of computer users in SAPCO industrial company, Tehran, Iran (84 persons with 29.85±11.2 years of age and with 6.98±2.54 years of experience). An active ergonomics-training program was designed and implemented during 14 days to empower the VDT users and involve them in improving their workstations. The direct observational RULA (Rapid Upper Limb Assessment) method was used in pre and post-intervention stages to evaluate the risk of WMSDs among participants.
Results: The RULA final scores showed that 18.8 % of VDT users were at action level 2, 63.5% at action level 3 and 17.6% at action level 4 before any intervention. In addition, 8.2% of users were at action level 1, 44.7% at action level 2, 42.4% at action level 3 and 4.7% at action level 4 at the post-intervention stage. The results of Wilcoxon statistical test indicated that RULA scores ere decreased significantly after interventions (P < 0.05) and consequently, decreased risk of WMSDs.
Conclusion: Active ergonomics training programs can be used effectively to improve the VDT workstations and decrease the risk of musculoskeletal disorders among VDT users.
Keywords: VDT workstation, Ergonomics, Training, RULA, Musculoskeletal disorders
Introduction
During the last two decades, the population of VDT users has increased dramatically worldwide [1]. As the number of computer users is increasing day by day, the occurrence of musculoskeletal symptoms also is becoming considerable day by day. According to the findings of several studies conducted on work-related musculoskeletal disorders (WMSDs) among the video display terminals (VDTs) users, prevention of these disorders among this population is a challenge for many workplaces today [2].
According to the reports of Swedish Statistics Society, using the VDTs by Swedish workforce has approximately increased 30% between1989-2001[3]. Approximately 50% of workforce used VDTs in their occupation in 1999[4]. In recent years, the increased use of VDTs to doing various official and industrial tasks is one of the main challenges of human. Perhaps, ergonomics is the lost ring of technology transferring chain from industrialized countries to industrial developing countries [5]. Despite of the improving the quality and quantity of activities; some studies have indicated that continues and long-time working at poorly designed VDT workstations may be resulted in WMSDs. Higher incidence of various musculo-skeletal symptoms and disorders among VDT users compared with non-VDT users have been indicated by some studies [6]. Korhonen et al. reported 34% annual incidence of neck pain in VDT user's population of Finland [7]. Another study on VDT users reported 58% annual incidence of neck/shoulder musculoskeletal symptoms in USA [8]. In addition, the study conducted by national institute for occupational safety and health (NIOSH) indicated that upper extremity musculoskeletal disorders are considerable in VDT users [9,10]. In 2001, Brenda Lee et al. investigated the effectiveness of an active ergonomics-training program for computer users and reported the significant decreasing of risk factors exposure in higher risk groups [11]. On the other hand, several etiologic studies in this area have strongly indicated the association between ergonomic risk factors and the development of neck and upper extremity WMSDs in VDT users [12].
Based on these findings, application of ergonomics principles to improve VDT workstations is a practical approach in controlling the risk factors and decreasing these disorders. Therefore, implementing the office ergonomics training programs may be effective on decreasing the incidence of WMSDs among VDT users. The majority of studies conducted in this area have used the subjective assessment tools to evaluate the effectiveness of their training or interventional programs. In contrast with these subjective assessment tools such as musculo-skeletal symptoms questionnaire or other questionnaires, the observational and objective assessment tools such as RULA can be used directly to assess the improvements in workstations after short duration and without any interaction with workers only via scoring the body postures, repetitive movements, force exertion and etc[13]. On the other hand, the ergonomic improvements in workplaces and workstations mostly can be defined and implemented without any cost or with low costs such as simple adjustments in dimensions, clearances, and reaches, repairing or substitution of tools or arrangement and layout of work and so on.
This study was conducted to evaluate the role of an ergonomics-training program in improving the VDT workstations that may be resulted in decreased risk of causing musculoskeletal disorders. For this purpose, an observational objective assessment tool was used to evaluate the effectiveness of simple and non-cost improvements for WMSDs risk control.
Materials and Methods
This cross-sectional and interventional study was conducted among a large group of computer users in SAPCO industrial company, Tehran, Iran in 2010. A simple designed form was used to collect demographic and some needed data about working time, job content and the user awareness about ergonomics. All of 84 persons (with 29.85±11.2 years of age and 6.98±2.54 years of experience) using a VDT at last 4 hours a day were selected to participate in this study. At first, the pre-intervention risk of WMSDs was assessed using a valid and reliable RULA (Rapid Upper Limb Assessment) method proposed for computer users [14]. In this pen-paper based observational method a coding system is used to rank or classify the risk level of WMSDs due to physical loading on the operator in 4 action level, 1( the lowest risk level ) to 4 (the highest risk level)[13]. In this technique, tow body segments are defined as group A (wrist, lower arm and upper arm) and group B (neck, trunk and leg). According to the RULA application principles, the VDT users were observed during the working shift and the most repetitive postures were selected for assessment. In order to facilitate the posture selection, a narrative job analysis method was used to determine the tasks assigned for users in their job. Then the task with the highest repetition or most duration of time was selected to complete the RULA worksheet.
The project objectives were explained for all of the users having action level 3 and 4 participated in a workshop. Meanwhile, the ergonomic principles of VDT workstations were presented in this workshop. The prepared guideline booklets of practical ergonomic rules at VDT workstations were distributed between users to read and ask any questions about workstation adjustment. This stage of training program was implemented during 14 days using guideline booklets and face-to-face training at workstations. The adjustment of workstations was accomplished by users themselves at the end of duration (self-directed intervention). these adjustments included: suitable arrangement of workstation and equipment (Fax, phone, printer), adjusting distance between monitor and user, seat height, monitor vertical and horizontal angles, copy holder situation, keyboard height, backrest angle, mouse situation, work–rest scheduling etc. Finally, after 30 days, the RULA method was used again to evaluate the behavioral working postures among users with action levels 3 and 4 at pre-intervention stage. The changes in RULA final scores, A and B group scores (per and post interventions) were analyzed with sign test.
Results
According to the primary collected data, nobody of VDT users was aware about ergonomic principles of VDT workstations. Some of the users had generally previous acquaintance with ergonomics, which was not adequate and applicable to adjust their workstations. The RULA assessment at pre-intervention stage for all of 84 users showed that 17.8 % of users were at action level 2(final score 3 or 4), 64.3% were at action level 3(final score 5 or 6) and 17.9% were at action level 4(final score 7). In other word, nobody had acceptable working situation and consequently, all of them were at WMSDs causing risk. Meanwhile, based on body segments assessment, the scores for group A were higher than those for group B were at pre-intervention stage. 82.2% of users (with action level 3 and 4) were selected to next stage (training and intervention program). As seen in Fig. 1, in post-intervention stage, 50.7% of these users were at action level 2, 49.3% at action level 3 and nobody was at action level 4. The sign statistical test showed that RULA final scores have been significantly decreased after intervention (P = 0.00). According to Fig. 2, the RULA final scores were shifted to lower levels at post-intervention stage in comparison with pre-intervention stage. The Fig. 3 shows that the RULA scores for group A were also shifted to lower levels at post- intervention stage in comparison with pre-intervention stage, however this variation was not considerable for group B (Fig. 4). The sign test showed that RULA scores for group A have been decreased significantly after intervention (P = 0.0309), but for group B this decreasing was not significant (P = 0.0693).
Fig. 1.
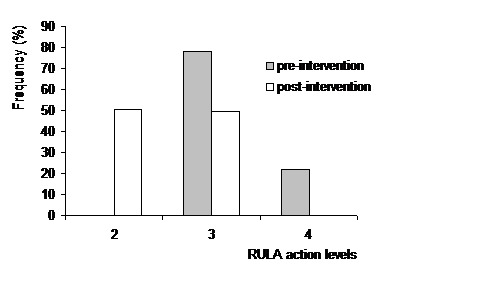
Comparison of RULA action levels between pre and post-intervention stages
Fig. 2.
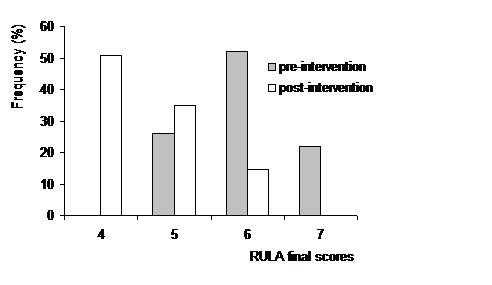
Comparison of RULA final scores between pre and post-intervention stages
Fig. 3.
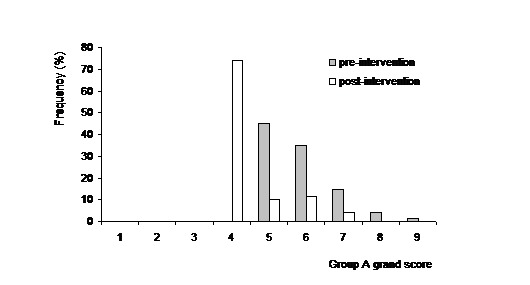
Comparison of group A scores between pre and post-intervention stages
Fig. 4.
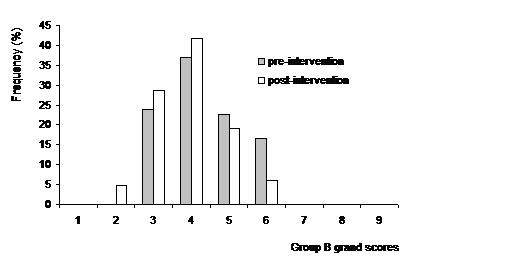
Comparison of group B scores between pre and post-intervention stages
Discussion
The obtained results in pre-intervention stage indicated that all of the VDT users are exposed to WMSDs causing risk at different levels and consequently, ergonomic improvements are needed. As elicited from figures 3 and 4, the obtained risk scores for group A were higher than those for group B were at pre-intervention stage. It means that the body segments wrist, forearm, and upper arm were exposed to more WMSDs causing risk than body segments neck, trunk, and legs. In other word, the group A body segments were impacted with higher physical loading from external load factors or risk factors such as awkward postures, repetitive motions, static muscular use than those in group B. The unadjusted parameters of workstations affecting group A postures such as seat height, keyboard height and mouse position can be resulted in this situation. In addition, the detailed analysis of group B scores showed the more contribution of neck scores to final group B scores, so the more physical load on neck segment.
Based on these results, the training program focused on ergonomic adjustment of the seat height, keyboard height, mouse height and positioning, monitor height, distance and vertical\horizontal angles. The obtained results at post-intervention stage showed the significant reduction in RULA final scores due to positive changes at VDT workstations following the effective and successful ergonomics-training program. Similar results have been reported by other studies [2,12]. The significant decreasing of RULA final scores after interventions indicated the considerable attention of participants to the trained adjustments. In addition, the detailed analysis of RULA scores in this stage showed considerable decreasing of arm; wrist and neck risk levels in comparison with other body segments. This means that, effective adjustments on seat height, keyboard, mouse and monitor height and positioning have been conducted by users.
It should be noted that, However, there was not meaningful decreasing in group B scores, but that is eligible. The obtained results in this area showed that only in 12% of users, the group B grand score was constant or slightly changed, while in other users the scores significantly decreased. From ergonomic point of view, decreasing even one score of RULA scores is important and effective on the risk of causing musculo-skeletal disorders regardless its statistical significance, because that is a result of an improvement in a VDT workstation. Therefore, the decreasing in RULA scores for group B are valuable, notwithstanding these changes are not statistically significant.
In addition, this study indicated that RULA, as a direct observational risk assessment method, is a sensitive method to changes in workstations and can be used for evaluating the effectiveness of ergonomic interventional programs. This result of current study supported the findings of previous studies in this area [2,14]. The use of questionnaires rather than direct observation to evaluate workstation setup and posture is also a potential limitation that R.J. Lewis et al expressed because of their study on VDTs [12]. In some studies, the self-report assessment method via questionnaires is used as a long-time assessment tool to evaluate the effectiveness of training programs. Beside of its advantages, some limitations have been pointed by research groups using this method. For instance, due to lack of a participant group not receiving the training program, the improvements observed in workstations, working postures and WMSDs symptoms could not be directly attributed to the training program. In addition, the application of the self-report questionnaires has another potential limitation, although it is a very widely used method of eliciting musculoskeletal symptoms from a population. Katz et al. noted that there is often only a modest correlation between observed health status and self-reported pain [15].
However, using observational methods eliminates many of these limitations; these methods themselves have some limitations such as accurate selecting most repetitive posture, validity and inter observer and intra-observer reliability of the selected method. Therefore, further long-term studies using direct measurement methods should be conducted to determine the variations in occurrence of WMSDs symptoms.
In conclusion, the findings shows that the VDT users are exposed to considerably high levels of WMSDs causing risk and consequently, the ergonomic improvements are needed. The significantly decreased RULA scores after interventions indicate the considerable attention of participants to the trained adjustments. As a main finding, this study suggests that ergonomics training programs can be effectively used to improve VDT workstations and decrease the WMSDs causing risks, which may be resulted in reduced musculoskeletal symptoms. In addition, the sensitivity of RULA as an observational assessment method is enough to evaluate the effectiveness of the ergonomics interventional programs at VDT workstations.
Acknowledgments
This study was conducted in a Company Supplying material and automotive parts and complexes to IK group. The authors wish to acknowledge the support provided by this company management and the good coordination and collaboration of VDT users participated in this study. The authors declare that there is no conflict of interests.
References
- [1]. Wahlstrom J. Ergonomics, musculoskeletal disorders, and computer work. Occup med (lond) 2005; 55:168–176. Available from http://occmed.oxfordjournals.org/content/55/3.toc [DOI] [PubMed]
- [2]. Greene LB. Effectiveness of an active ergonomics training program for computer users. PhD dissertation, University of Georgia; 2001.
- [3]. Statistics Society of Sweden. The working environment. Report No. AM68SM0201; 2002.
- [4].Amick BC, Swanson NG, Chang H. Office technology and musculoskeletal disorders: Building an ecological model. Occup Med. 1999;14(1):97–112. [PubMed] [Google Scholar]
- [5].Shahnavaz H. Transfer of Technology to industrial Developing Countries and Human Factors Considerations Center for Ergonomics of Developing Countries. Lulea University. 1991:50–51. [Google Scholar]
- [6].El-Bestar SF, El-Mitwalli AA, Khashaba EO. Neck-upper extremity musculoskeletal disorders among workers in the telecommunications company at Mansoura City. Int J Occup Saf Ergon. 2011;17(2):195–205. doi: 10.1080/10803548.2011.11076879. [DOI] [PubMed] [Google Scholar]
- [7].Korhonen T, Ketola R, Toivonen R, Luukkonen R, Hakkanen M, Viikari JE. Work related and individual predictors for incident neck pain among office employees working with video display units. Occup Environ Med. 2003;60:475–482. doi: 10.1136/oem.60.7.475. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [8].Gerr F, Marcus M, Ensor C, Kleinbaum D, Cohen S, Edwards A, Gentry E, Ortiz DJ, Monteilh C. A prospective study of computer users: Study design and incidence of musculoskeletal symptoms and disorders. Am J Ind Med. 2002;41:221–235. doi: 10.1002/ajim.10066. [DOI] [PubMed] [Google Scholar]
- [9].Hales TR, Sauter SL, Peterson MR, Fine LJ, Putz-Anderson V, Schleifer LR, Ochs TT, Bernard BP. Musculoskeletal disorders among visual display terminal users in a telecommunications company. Ergonomics. 1994;37:1603–21. doi: 10.1080/00140139408964940. [DOI] [PubMed] [Google Scholar]
- [10]. Sauter SL, Swanson NG. An ecological model of musculoskeletal disorders in office work, Beyond Biomechanics: Psychosocial Aspects of Musculoskeletal Disorders in Office Work. 2nd ed. Taylor & Francis press. London; 1996; pp. 3-21.
- [11].Greene BL, DeJoy DM, Olejnik S. Effects of an active ergonomics-training program on risk exposure, worker beliefs and symptoms in computer users. Work Reading Mass. 2005;24(1):41–52. [PubMed] [Google Scholar]
- [12].Lewis RJ, Fogleman M, Deeb J, Crandall E, Agopsowicz D. Effectiveness of a VDT ergonomics training program. Int J Ind Ergonomics. 2001;27(2):119–131. [Google Scholar]
- [13].McAtamney McAtamney, L L, Corlett EN. RULA: A survey Method for the Investigation of Work-Related Upper Limb Disorders. Applied Ergonomics. 1993;24(2):91–99. doi: 10.1016/0003-6870(93)90080-s. [DOI] [PubMed] [Google Scholar]
- [14]. Lueder R. A Proposed RULA for Computer Users. Proceeding of the ergonomics Summer Workshop, UC Berkeley Center for Occupational & Environmental Health continuing education Program, San Francisco; 1996.
- [15].Katz JN, Punnett L, Simmons BP, Fossel AH, Mooney N, Keller RB. Workers' compensation recipients with carpal tunnel syndrome: the validity of self-reported health measures. Am J Publ Health. 1996;86:52–56. doi: 10.2105/ajph.86.1.52. [DOI] [PMC free article] [PubMed] [Google Scholar]