

Abstract
Background: Obesity is a serious public health issue in the United States, with the CDC reporting that most adult Americans are now either overweight or obese. Little is known about the comparative acceptability of available weight management approaches in non-treatment seeking samples.
Method: This report presents preliminary survey data collected from an online sample on weight management preferences for 8 different weight management strategies including a proposed incentive-based program. Participants were 72 individuals (15 men, 55 women and 2 transgendered individuals) who self-reported being overweight or obese, or who currently self-reported a normal weight but had attempted to lose weight in the past.
Results: ANOVA and Pair-wise comparison indicated clear preferences for certain treatments over others in the full sample; most notably, the most popular option in our sample for managing weight was to diet and exercise without professional assistance. Several differences in preference between the three weight groups were also observed.
Conclusions: Dieting and exercising without any professional assistance is the most highly endorsed weight management option among all groups. Overweight and obese individuals may find self-management strategies for weight loss less attractive than normal weight individuals, but still prefer it to other alternatives. This has implications for the development and dissemination of empirically based self-management strategies for weight.
Keywords: Weight management, Treatment preferences, Obesity
Introduction
Obesity is a serious public health issue in the United States, with the Centers for Disease Control and Prevention (CDC) reporting that 73.7% of the population ages 20 and over are overweight, obese or extremely obese1. Obesity can lead to a range of serious health conditions, including Type 2 Diabetes, coronary heart disease, certain types of cancers, hypertension, stroke and respiratory problems1. While there is significant data on the effectiveness of various weight management techniques for individuals in weight loss treatment2, some research on rates of weight loss attempts in general population samples3, and some inquiry as to patient preferences for individual versus group weight loss treatment4 to our knowledge there is no research that has been conducted to assess the acceptability of specific weight management strategies that include commercial products in a general population sample.
Some evidence suggests that with regard to psychological treatment, client preference for different types of treatment improves therapy outcomes and dropout rates5. This may also translate to preference for weight loss methods, in which acceptability of a treatment could impact strategy adoption or eventual follow through. The majority of the US population is now estimated to be either overweight or obese1, and a plethora of available weight loss methods exist therefore, identifying which weight control options non-treatment seeking individuals in the general public find acceptable is an important clinical and public health question. A wide range of options exists for weight control, including commercial, medical and self-management techniques with varying degrees of effectiveness2, 3, 6. However, little is known regarding individuals’ willingness to try these different strategies.
The purpose of the present survey was to investigate preferences for eight different weight loss strategies, including seven common weight management techniques: meal replacement programs, weight loss medication, group support for weight loss, one-on-one treatment (with a dietitian, personal trainer or counselor), surgical weight loss treatments, online weight loss programs, and dieting and exercising on one’s own without additional assistance. Additionally, one proposed incentive-based weight loss program was also investigated. These preferences were assessed via an anonymous online survey with a sample of non-treatment seeking adults (i.e.- individuals recruited from the general population rather than a population actively seeking weight loss treatment), ages 18 and older.
Materials and Methods
Participants and procedures
A sample of 72 participants was analyzed for this analysis. Participants were recruited via advertisements on the websites Craigslist.org (a classified advertisement website) and Reddit.com (a social news website). These websites were chosen because their structure and policies allowing the solicitation of volunteers. Internal Review Board approved advertisements were posted weekly over the course of 5 months (July 2012-January 2013); the advertisements followed the websites’ respective terms of use policies. On Craigslist.org, the advertisement was posted for the New York Metropolitan area to recruit a diverse participant sample. The advertisements included a link to the questionnaire, which was developed and hosted using Qualtrics.com. The only inclusion criterion for the survey was that participants are 18 years or older, as indicated by self-report. The initial sample consisted of122 participants; however, some participants were eliminated from the analysis due to incomplete participation (as defined by terminating the survey before the end) or skipping target items (e.g.- height/weight and preferences for the weight loss strategies presented) (N=23). Additionally, the analyses reported in this paper targeted individuals who were overweight, obese or who were normal weight but reported a history of weight loss attempts, in an effort to capture the opinions of individuals who were most likely to eventually seek weight loss techniques. Thus, individuals not meeting these criteria (e.g., normal weight individuals who reported no history of weight management efforts) were excluded from the analysis (N=27).
Measures
The survey took approximately 15 minutes to complete. Participants were asked to provide demographic information, including age, race/ethnicity, annual household income, level of education and zip code. No other identifying information was collected in order to ensure participant anonymity. Eight weight loss strategies were assessed as part of the questionnaire: meal replacement programs (e.g.. Jenny Craig™, Nutrisystem™), weight loss medication (e.g.,Alli™), group support for weight loss(e.g. Weight Watchers™), one-on-one treatment (e.g., meeting with a dietitian, personal trainer or counselor), surgical weight loss treatments (e.g., gastric bypass and lap-band surgeries), online weight loss programs(e.g. MyFitnessPal.com), dieting and exercising on one’s own without additional assistance, and a novel incentive-based program(e.g., receiving rewards for meeting weight goals). Preferences for these strategies were assessed with the question “Please rate how likely you would be to try the following weight loss treatment strategies if you wanted to lose weight” followed by a 0-100 slide bar visual analog scale. Individuals were asked to self-report their weight in pounds and their height in feet and inches. Body Mass Index was calculated by the survey software using the formula: BMI= weight (lb.) / [height (in)] 2 x 703, which is the current standard7.Individuals were also asked if they had ever attempted to lose weight in the past (yes/no) and were provided with a text box to list their previously used strategies. National Development and Research Institute’s Internal Review Board approved all procedures and materials for this study.
Questions used to measure weight loss preferences were developed after a thorough review of the extant literature. The questions developed utilized a Visual Analog Scale method, which has been shown to be a highly acceptable method for patient’s completing health surveys6. However, this weight preferences questionnaire has not been validated outside of this pilot study.
Statistics
Data were analyzed using SPSS Version 20 statistical software. Descriptive statistics were conducted to provide information about the sample. A Within-Subjects-Repeated-Measures ANOVA was conducted to assess differences in mean preferences for the various weight treatments described in the full group sample. Pairwise comparisons were then used to assess any significant difference between individual weight loss approaches. Additionally, a One-Way ANOVA was conducted to compare differences in preference mean ratings of the different weight loss strategies between individuals falling into the three self-reported weight categories: normal weight, overweight and obese.
Results
Sample Characteristics
The target sample was 76.4% female, 20.8% male and 2.8% transgender. Racial breakdown of the sample was 68.1% white, 12.5% African American, 8.3% Asian, 16.7% Hispanic/Latino, 1.4% Native Hawaiian or Other Pacific Islander and 8.3% multiracial. With regard to annual household income, 34.7% of the sample reported a household income of less than $30,000 a year, 13.9% reported $30,000-44,000 a year, 9.7% reported $45,000-60,000 a year, 12.5% reported $60-75,000 a year, 11.1% reported making $75-100,000, 13.9% reported making $100,000 or more and 4.2% reported that they did not know their household incomes. Participant education level was as follows: high school diploma/GED- 8.3%, business/technical school- 1.4,%, some college- 34.7%, Associate degree-8.3%, Bachelor’s Degree- 37.5%, Master’s Degree- 9.7% Age of participants ranged from 18 to 70 years old, with a mean of 29.4 (S.D.= 12.16) years old. Of the sample of 72 participants, 30 (BMI ≤ 25) reported currently being normal weight, but had made past weight loss attempts, 20 reported being overweight (BMI= 25-29.9) and 22 reported being obese (BMI ≥ 30). Weight was self-reported by participants in pounds; height was reported in feet and inches.
Body Mass Index Classifications
Body Mass Index was calculated from the participants self-reported height and weight by the survey software using the formula: BMI= weight (lb.) / [height (in)] 2 x 703, which is the current standard7. Of the sample of 72 participants, 30 (BMI ≤ 25) reported currently being normal weight, but had made past weight loss attempts, 20 reported being overweight (BMI= 25-29.9) and 22 reported being obese (BMI ≥ 30). Weight was self-reported by participants in pounds; height was reported in feet and inches.
Weight Loss Method Preferences
Within-Subjects Repeated-Measures ANOVA revealed statistically significant differences in preferences for the weight management strategies presented in the full sample, F (7, 65)=38.12, P<0.01. Pairwise comparison revealed that many of the strategies received statistically different mean rating scores (Table 1). The most frequently endorsed treatment, diet/exercise on one’s own, was ranked significantly higher than all of the other strategies in the full sample. One-on-one treatment with a dietitian, personal trainer or counselor, the incentive-based program, and online programs for weight management were the next most popular options and did not differ significantly from each other. Preferences for weight loss groups (e.g., Weight Watch-ers™), weight loss medications (e.g., Alli™) and meal replacement programs (e.g., Jenny Craig™) were ranked 5th, 6th and 7th respectively and were not significantly different from each other. Lastly, surgical interventions (e.g., gastric bypass and lap-band surgeries) were rated as the least preferred of all the weight loss options presented. See Fig. 1 for mean scores of weight management preferences.
Table 1. Pairwise comparisons of weight loss approach preferences, tstatistic reported (n=72) .
| Variables | X1 | X2 | X3 | X4 | X5 | X6 | X7 |
| X1. Diet and Exercise on your own | |||||||
| X2. One on One Tx | -7.44* | ||||||
| X3. Incentive Program | 9.51* | 3.19* | |||||
| X4. Online Program | -11.26* | 2.67* | .835 | ||||
| X5. GroupTx | -12.67* | 7.94* | -3.03* | -3.73* | |||
| X6.Medication | -13.86* | -6.90* | -4.35* | -4.518* | 0.78 | ||
| X7. Meal Replacements | -17.19* | -8.68* | -4.13* | -5.25* | 1.14 | 0.184 | |
| X8. Surgery | -20.05* | 11.84* | -8.27* | -8.66* | 6.91* | 5.03* | 4.99* |
*P<.05
Fig. 1.
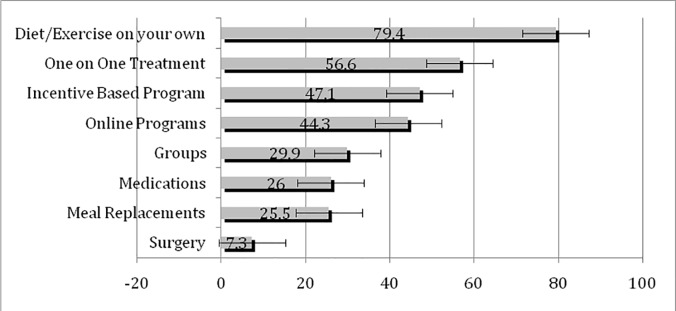
Mean Interest Scores in Weight Management Treatments (N=72)
Between Group Differences
One-way between subjects ANOVA was conducted to compare mean weight loss preferences in the three weight groups: normal weight, overweight and obese. Individuals in both the overweight and obese groups rated dieting and exercising on one’s own less favorably than the normal weight group, F (2, 69)=4.6, P=.01, whereas the obese group also rated online treatments significantly less favorably than both the overweight and normal weight groups, F (2, 69)= 3.23, P=.04. There were no other statistically significant differences between the groups with regard to weight management preference.
Discussion
These data suggest that individuals who are obese, overweight and/or have a history of weight loss attempts have significant preferences for certain weight loss treatments over others. Notably, dieting and exercising without professional or medical assistance was rated as the most favorable and likely to be utilized weight loss option among all three groups assessed (normal, overweight, and obese). While there is some evidence that structured weight management programs produce better weight loss results than self help8 and that group programs produce better results than individual treatment4, it is not realistic to expect that all individuals interested in losing weight would take part in such a program due to personal preferences, cost and program availability. This finding is congruent with research in other areas of behavioral health management. For example, despite advances in smoking cessation treatments, most individuals who quit smoking report preferring to do so on their own9. In light of this finding, a focus on the dissemination of empirically supported self-help weight loss methods may be most helpful for the widest range of people. For example, primary care physicians could proactively provide practical, scientifically sound advice and techniques to help individuals manage their weight on their own, even if weight is not the primary focus of their medical visit.
Interest in a novel incentive-based strategy received a statistically similar mean level of preference as both one-on-one professional assistance and online weight management programs; these three strategies were the most popular options after dieting and exercising on one’s own. This suggests that an incentive-based strategy may be an acceptable option for those individuals interested in assisted weight loss programs. Similar incentive-based programs for weight loss have been studied and there is evidence to suggest that this technique is effective at initiating weight loss10; however, as with most weight loss interventions, long-term sustainability of weight loss has been more challenging
Commercially available weight loss strategies, including group treatments such as Weight Watchers, meal replacements such as Jenny Craig, and diet medications/-supplements such as Alli, ranked 5th, 6th and 7th, respectively and thus were among the least popular options for this sample. Despite a lack of research on the true effectiveness of these approaches11, Marketdata Enterprises Inc., an independent market research publisher, reported that revenues for the weight loss industry in the US were 60.9 billion dollars in 201012. However, this same report stated that slower than anticipated growth in the commercial weight loss industry may be due to the current economic recession. The current economic climate may also have impacted this survey's finding, that more individuals endorsed dieting and exercising on one’s own as the most attractive option, which can be accomplished with minimal financial costs. This may be especially relevant to the current sample, considering that about one third of participants reported an annual household income of less than $30,000.
Surgical treatment was the least endorsed option in this sample. That surgical options would be ranked as the least popular option in this sample is not surprising in light of 1) the current recommendation that bariatric surgery be reserved for individuals in the “extremely obese” category (BMI ≥40) or have a BMI ≥ 35 with serious health problems related to their weight status, such as Type 2 Diabetes 2) the significant financial cost and 3) the potentially serious side effects13. In this sample, only six individuals had a self-reported BMI equal to or greater than 35, which may have contributed to the low endorsement of surgical procedures.
While rank order of preferences did not differ among the three weight groups, individuals ranked level of interest in "diet/exercise on one’s own" significantly less favorably if they were in the self-reported obesity group (although it was still the most popular option among this group). Similarly, individuals in both the overweight and obese groups ranked online programs less favorably than the normal weight group. This suggests the possibility of different perceived treatment needs and that a more tailored approach to weight management treatments may be most palatable for individuals of different weight statuses.
A limitation of this study is the self-reported nature of the participants’ weight; however, there is evidence that self-reported weight can be a sufficient estimate of actual weight14 and the anonymous nature of the survey may have decreased motivation to falsify reports. This sample was also limited to individuals in the New York City metropolitan area, and replication elsewhere could strengthen the generalizability of the findings. Moreover related to this sample is the possibility that factors such as gender, age, socioeconomic status and/or comorbid health conditions may affect weight loss approach choice, however, that analysis and discussion is beyond the scope of this article. Additionally, this sample had a disproportionate number of female respondents. Targeting men interested in weight loss options may yield gender differences and should be a topic of future investigation. Furthermore, the issue of sustained long-term weight loss, arguably the most crucial and difficult part of weight management15, was not assessed in this survey. An additional qualitative investigation of individuals’ reasons for preferring one weight loss method to another could help elucidate this issue and provide important feedback for the development of new weight loss methods that produce long-term benefits.
Conclusion
Despite these limitations, the current findings are an important first step in developing a more comprehensive understanding of weight management preferences, with the aim of translating the findings into tailored outreach programs. Thus far, the majority of the research on weight management options has been limited to those individuals seeking professionally guided weight management treatments. Research that focuses on the acceptability of various weights loss strategies in the general public is critical to understanding what a society wide issue is increasingly.
Acknowledgements
The first author on this paper is supported by a NIH/NIDA Ruth L. Kirchstein National Research Service Award (T32 DA007233). The funding source had no other involvement other than salary support. All authors contributed in a significant way to the manuscript and all authors have read and approved the final manuscript. No conflicts of interest declared for any of the authors involved with this manuscript.
Citation: Barry VB, Raiff BR. Weight Management Preferences in a Non-Treatment Seeking Sample. Health Promot Perspect 2013; 3(2): 147-153.
References
- 1. Centers for Disease Control and Prevention. Obesity and Overweight for Professionals: Data and Statistics: U.S. Obesity Trends | DNPAO | CDC [Internet]. [Cited 2011 Oct 17]. Available from: http://www.cdc.gov/obesity/data/trends.html
- 2.Berkel LA, Carlos Poston WS, Reeves RS, Foreyt JP. Behavioral Interventions for Obesity. J Am Diet Assoc. 2005;105((5 Suppl 1)):S35–43. doi: 10.1016/j.jada.2005.02.031. [DOI] [PubMed] [Google Scholar]
- 3.Williamson DF, Serdula MK, Anda RF, Levy A, Byers T. Weight loss attempts in adults: goals, duration, and rate of weight loss. Am J Public Health. 1992 Sep;82(9):1251–7. doi: 10.2105/ajph.82.9.1251. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Renjilian DA, Perri MG, Nezu AM, McKelvey WF, Shermer RL, Anton SD. Individual versus group therapy for obesity: Effects of matching participants to their treatment preferences. J Consult Clin Psychol. 2001;69(4):717–21. [PubMed] [Google Scholar]
- 5.Swift JK, Callahan JL. The impact of client treatment preferences on outcome: a meta-analysis. J Clin Psychol. 2009;65(4):368–81. doi: 10.1002/jclp.20553. [DOI] [PubMed] [Google Scholar]
- 6.Lenert LA, Sturley AE. Acceptability of computerized visual analog scale, time trade-off and standard gamble rating methods in patients and the public. Proc AMIA Symp. 2001:364–8. [PMC free article] [PubMed] [Google Scholar]
- 7. Centers for Disease Control and Prevention. Healthy Weight: Assessing Your Weight: BMI: About Adult BMI | DNPAO | CDC [Internet]. 2013 [cited 2013 Jan 2]. Available from: http://www.cdc.gov/healthyweight/assessing/bmi/adult_bmi/index.html#Interpreted
- 8.Heshka S, Anderson JW, Atkinson RL, Greenway FL, Hill JO, Phinney SD. et al. Weight loss with self-help compared with a structured commercial program: A randomized trial. JAMA . 2003;289(14):1792–8. doi: 10.1001/jama.289.14.1792. [DOI] [PubMed] [Google Scholar]
- 9.Zhu S-H, Melcer T, Sun J, Rosbrook B, Pierce JP. Smoking cessation with and without assistance: A population-based analysis. Am J Prev Med. 2000 May;18(4):305–11. doi: 10.1016/s0749-3797(00)00124-0. [DOI] [PubMed] [Google Scholar]
- 10.Volpp KG, John LK, Troxel AB, Norton L, Fassbender J, Loewenstein G. Financial Incentive–Based Approaches for Weight Loss. JAMA . 2008;300(22):2631–2637. doi: 10.1001/jama.2008.804. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Tsai AG, Wadden TA. Systematic Review: An Evaluation of Major Commercial Weight Loss Programs in the United States. Ann Intern Med. 2005;142(1):56–66. doi: 10.7326/0003-4819-142-1-200501040-00012. [DOI] [PubMed] [Google Scholar]
- 12. PRweb.com. U.S. Weight Loss Market Worth $60.9 Billion [Internet]. 16:28:13 [cited 2013 Jan 2]. Available from: http://www.prweb.com/releases/2011/5/prweb8393658.htm
- 13. WIN - Publication - Bariatric Surgery for Severe Obesity [Internet]. 16:38:34 [cited 2013 Jan 2]. Available from: http://win.niddk.nih.gov/publications/gastric.htm
- 14.Stunkard AJ, Albaum JM. The accuracy of self-reported weights. Am J ClinNutr 1981 Aug. 1;34(8):1593–9. doi: 10.1093/ajcn/34.8.1593. [DOI] [PubMed] [Google Scholar]
- 15.Klem ML, Wing RR, McGuire MT, Seagle HM, Hill JO. A descriptive study of individuals successful at long-term maintenance of substantial weight loss. Am J Clin Nutr . 1997 Aug 1;66(2):239–46. doi: 10.1093/ajcn/66.2.239. [DOI] [PubMed] [Google Scholar]