

Case Report
A 32-year-old male presented with a history of large swelling on the scalp since 8 months, patient also complained of pain since 8 months. He gives past history of a similar swelling in the same region for which he underwent excision elsewhere and on histopathology, was found to be a trichilemmal cyst. The lesion recurred within 4 months of excision and increased to the present size in 8 months with rapid increase in size in the last 2 months.
Fig. 7.

One year postoperative image showing healed scar
On examination, scalp showed a large swelling measuring 15 × 12 cm, skin over it was stretched non-pinchable with a scar of the previous surgery, (Fig. 1). It was tender and firm in consistency. There was no regional lymphadenopathy. X-ray skull showed no bone involvement.
Fig. 1.

Right posterior auricular swelling with a healed curvilinear scar (thin arrow) over the scalp; Note another irregular healed scar at the right parieto-occipital region (thick arrow)
A wide excision of the mass was done under general anesthesia with a 2 cms clearance all around. A transposition flap from the neck was used to cover the defect.
Grossly, the excised specimen consisted of a well-circumscribed skin covered tissue measuring 13 × 8.5 cms, (Fig. 2), cut surface showed two gray white solid nodules measuring 6 × 4 cms and 4 × 3 cms respectively (Fig. 3).
Fig. 2.

ᅟ
Fig. 3.

ᅟ
Microscopy showed cellular tumor arising from dermis and infiltrating subcutaneous tissue, tumor cells were arranged in islands, lobular and diffuse infiltrating patterns (Fig. 4). Lobules showed abrupt keratinization without interposed granular layer (trichelemmal type) and keratin pearls (Fig. 5). Tumor cells were oval to polygonal with abundant cytoplasm, few areas cells showed high nucleo-cytoplasmic ratio, nuclear hyperchromasia and pleomorphism, mitotic figures were also noted, stroma was desmoplastic (Fig. 6). Skin and resected margins were free of tumor.
Fig. 4.

Skin with tumour islands in the dermis arranged in lobular and diffuse pattern (H and E, 20×)
Fig. 5.
a Tumour cells arranged in lobules with a few showing keratinization (H and E, 40×); b Individual tumour cells are polygonal with some showing clearing of cytoplasm and keratinization (H and E × 40); c Islands of clear tumour cells showing nuclear pleomorphism and mitotic activity (H and E, 100×); d Neoplastic cells show abrupt keratin production (H and E, 40×)
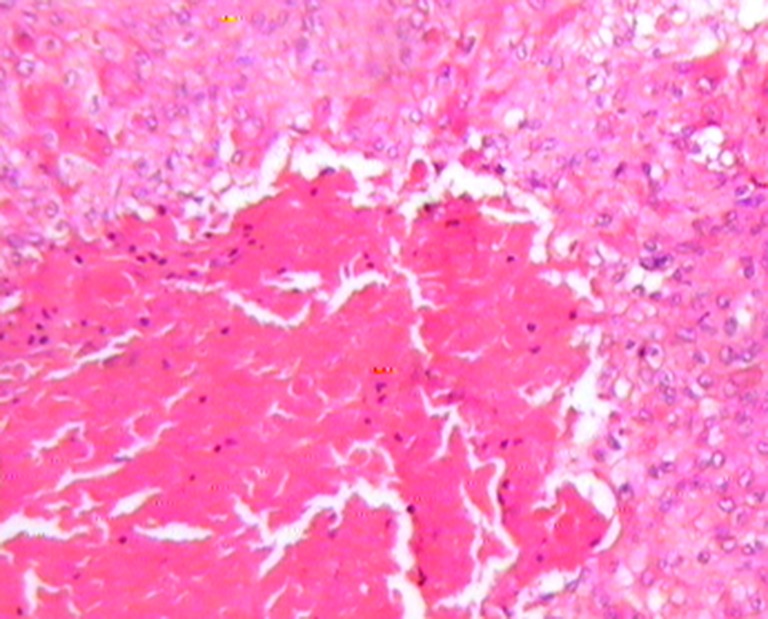
Fig. 6.

Tumour nests showing basophilic areas of calcification (H and E, 100×); Inset shows islands of pleomorphic tumour cells with many mitotic figures, a few of which appear atypical (H and E, 200×)
Based on these findings, a diagnosis suggestive of malignant proliferating trichilemmal tumour (MPTT) low grade was made on histopathology and was advised Immunohistochemistry for confirmation.
Immunohistochemistry was done elsewhere which showed tumor cells positive for CD34 and calretinin consistent with MPTT. The postoperative course was uneventful and the patient is doing well on follow-up.
Discussion
Tumours arising from the outer root sheath of hair follicles comprises of 0.1 % of skin tumors, Saida et al. in 1983 defined three stages of trichilemmal tumors - trichilemmal cyst, (adenomatous stage); proliferating trichilemmal tumor, (epitheliomatous stage) and malignant PTT, (carcinomatous stage) [1, 2]. These tumors usually occuring in the scalp of elderly women and show characteristic trichilemmal keratinisation. A trichilemmal cyst is by far the most common of these [3].
Proliferating trichilemmal tumour is a benign neoplasm, it can rarely undergo malignant transformation in a step-wise manner starting with trichilemmal cyst to PTT evolving into MPTT [4]. Clinically sudden enlargement of longstanding nodular scalp lesions and histological evidence of significant abnormal mitosis, marked cellular pleomorphism, infiltrating margins reflect malignant transformation. Our case possibly represents the event of malignant transformation in a proliferating trichilemmal tumour.
Ye et al. proposed a stratification of proliferating pilar tumors into the following 3 groups:
(Benign)- Well circumscribed lesion with pushing margins; mild nuclear atypia, absence of mitoses, necrosis, and neurovascular invasion.
(Malignant Low grade)- Similar to group 1 but manifest as irregular, locally invasive silhouettes with involvement of the deep dermis and subcutis.
(Malignant High grade)- Invasive growth patterns, marked nuclear atypia, pathologic mitotic forms, and necrosis, with or without neurovascular invasion [5].
Proliferation markers like Ki67 and p53 can assist in the three-tier classification as suggested by Ye et al. [6].
A close differential diagnosis for MPTT is squamous cell carcinoma. Histological evidence of trichilemmal keratinization, lobular pattern and the lack of a precursor epidermal lesion such an actinic keratosis differentiates MPTT from squamous cell carcinoma [7]. Various IHC markers have been used to highlight the outer sheath differentiation including CD34 and calretinin may distinguish a malignant proliferating pilar tumor from a squamous cell carcinoma [8, 9].
Wide local excision with a 1-cm margin of normal tissue is the preferred treatment for MPTT. In addition to surgery, chemotherapy and radiotherapy have been used by some authors to prevent recurrence in MPTT [7]. No adjuvant therapy was given to our patient post surgery. However, the patient has been is under regular follow-up.
References
- 1.Ye J, Nappi O, Swanson PE, Patterson JW, Wick MR. Proliferating pilar tumors: A clinicopathologic study of 76 cases with a proposal for definition of benign and malignant variants. Am J Clin Pathol. 2004;122(4):566–74. doi: 10.1309/0XLEGFQ64XYJU4G6. [DOI] [PubMed] [Google Scholar]
- 2.Siddha M, Budrukkar A, Shet T, Deshpande M, Basu A, Patil N, et al. Malignant pilar tumor of the scalp: A case report and review of literature. J Cancer Res Ther. 2007;3:240–3. doi: 10.4103/0973-1482.39001. [DOI] [PubMed] [Google Scholar]
- 3.Saida T, Ooharo K, Hori Y, Tsuchiya S. Development of a malignant proliferating trichilemmal cyst in a patient with multiple trichilemmal cysts. Dermatologica. 1983;166:203–8. doi: 10.1159/000249868. [DOI] [PubMed] [Google Scholar]
- 4.Folpe AL, Reisenauer AK, Mentzel T, Rütten A, Solomon AR. Proliferating trichilemmal tumors: Clinicopathologic evaluation is a guide to biologic behavior. J Cutan Pathol. 2003;30:492–498. doi: 10.1034/j.1600-0560.2003.00041.x. [DOI] [PubMed] [Google Scholar]
- 5.Trabelsi A, Stita W, Gharbi O, Kanani N, Sriha B, Korbi S. Malignant proliferating trichilemmal tumor of the scalp: A case report. Dermatol Online J. 2008;14:11. [PubMed] [Google Scholar]
- 6.Yotsuyanagi T, Urushidate S, Yokoi K, Sawada Y. A malignant proliferating trichilemmal tumor simulating a squamous cell carcinoma. Eur J Plast Surg. 1997;20:320–2. doi: 10.1007/BF01387863. [DOI] [Google Scholar]
- 7.Satyaprakash AK, Sheehan DJ, Sangueza OP. Proliferating trichilemmal tumors: a review of literature. Dermatol Surg. 2007;33:1102–8. doi: 10.1111/j.1524-4725.2007.33225.x. [DOI] [PubMed] [Google Scholar]
- 8.Chaichamnan K, Satayasoontorn K, Puttanupaab S, Attainsee A. Malignant proliferating trichilemmal tumors with CD34 expression. J Med Assoc Thai. 2010;93(Suppl 6):S28–34. [PubMed] [Google Scholar]
- 9.Gonzalez-Guerra E, Requena L, Kutzner H. Immunohistochemical study with calretenin in normal Hair follicles and tumors with Follicular differentiation. Actas Dermosifiliogr. 2008;99:456–63. doi: 10.1016/S0001-7310(08)74716-1. [DOI] [PubMed] [Google Scholar]