

Abstract
This is a review of the characteristic findings of inflammatory bowel disease (IBD) associated with primary sclerosing cholangitis (PSC) and their usefulness in the diagnosis of sclerosing cholangitis. PSC is a chronic inflammatory disease characterized by idiopathic fibrous obstruction and is frequently associated with IBD. IBD-associated with PSC (PSC-IBD) shows an increased incidence of pancolitis, mild symptoms, and colorectal malignancy. Although an increased incidence of pancolitis is a characteristic finding, some cases are endoscopically diagnosed as right-sided ulcerative colitis. Pathological studies have revealed that inflammation occurs more frequently in the right colon than the left colon. The frequency of rectal sparing and backwash ileitis should be investigated in a future study based on the same definition. The cholangiographic findings of immunoglobulin G4-related sclerosing cholangitis (IgG4-SC) are similar to those of PSC. The rare association between IBD and IgG4-SC and the unique characteristics of PSC-IBD are useful findings for distinguishing PSC from IgG4-SC.
Keywords: Primary sclerosing cholangitis, Primary sclerosing cholangitis, Inflammatory bowel disease, Inflammatory bowel disease-associated with primary sclerosing cholangitis, Immunoglobulin G4-related sclerosing cholangitis
Core tip: Inflammatory bowel disease (IBD)-associated with primary sclerosing cholangitis (PSC) (PSC-IBD) shows an increased incidence of pancolitis, mild symptoms, and colorectal malignancy. Although an increased incidence of pancolitis is a characteristic finding, some cases are endoscopically diagnosed as right-sided ulcerative colitis. Pathological studies have revealed that inflammation occurs more frequently in the right colon than the left colon. The cholangiographic findings of immunoglobulin G4-related sclerosing cholangitis (IgG4-SC) are similar to those of PSC. The rare association between IBD and IgG4-SC and the unique characteristics of PSC-IBD are useful findings for distinguishing PSC from IgG4-SC.
INTRODUCTION
Primary sclerosing cholangitis (PSC) is a chronic inflammatory disease characterized by idiopathic fibrous obstruction[1]. The fibrosis causes diffuse narrowing of the intrahepatic and extrahepatic bile ducts, and the resulting persistent biliary stasis leads to hepatic cirrhosis and a poor prognosis. Liver transplantation is indicated as a treatment for PSC. According to the diagnostic criteria for PSC proposed by the Mayo Clinic in 1999[1] and 2003[2], in addition to cholangiographic findings, the presence of inflammatory bowel disease (IBD) is important.
However, several related studies with contradictory results have recently been published[3,4].
IgG4-related sclerosing cholangitis (IgG4-SC) has recently been established as a new clinical entity[5]. The cholangiograms of IgG4-SC are occasionally similar to those of PSC[6]. The differential diagnosis of PSC and IgG4-SC is important because IgG4-SC patients respond well to steroid therapy[7].
In this study, we aimed to clarify the clinicopathological characteristics of PSC-IBD and the usefulness of PSC-IBD in the diagnosis of SC.
LITERATURE SEARCH
We conducted a literature search of English articles related to PSC-IBD, published between 2005 and March 2013, using the following keywords: “PSC,” “primary sclerosing cholangitis,” “PSC-IBD,” “IBD,” “immunoglobulin G4 (IgG4)-related sclerosing cholangitis (IgG4-SC),” “autoimmune pancreatitis,” and “IgG4-related disease (IgG4RD).” We connected the key words using “OR”. Pertinent articles obtained from the literature search were reviewed. All references were manually verified, and all reference lists in the retrieved articles were scrutinized to identify any additional articles that might have been missed in the PubMed search. As clinical data on PSC-IBD are limited, the authors also considered their own > 20-year clinical experience in the treatment of PSC-IBD. This study was primarily limited to adults patients, with the exception of the “frequency of PSC-IBD”section.
FREQUENCY OF PSC-IBD
PSC is strongly associated with IBD, and the prevalence of PSC-IBD is as high as 60%-80% in western countries[8]. Approximately 80% of IBD is represented by ulcerative colitis (UC), 10% by Crohn's disease (CD), and 10% by indeterminate colitis[9]. Conversely, only 2%-7.5% of IBD patients develop PSC[8].
Previous reports from Europe and the United States have indicated that IBD complicates a high proportion of PSC cases. In Japan, IBD is found in only 21%-32% of PSC cases, according to surveys conducted by the Japanese Society of Gastroenterology[10] and the Japan Society of Hepatology[11]. In a second nationwide analysis, only 125 of 388 patients (32%) had an established diagnosis of IBD, 79% of whom had UC, whereas only 6.4% were diagnosed with CD[11]. Ang et al[12] also reported a low association rate of 20% (2/10) between PSC and IBD in Singapore. The association of PSC with IBD varies depending on geographical location, with higher rates in European and American populations, and a significantly lower association in Asian patients[13]. However, the incidence of IBD in PSC patients in our series was higher (68.9%) than that already reported in Japan[14]. We speculate that this high incidence was noted because only PSC patients who had undergone total colonoscopy at clinical onset were enrolled in our study. Yamagishi et al[15] also reported a higher incidence of IBD in PSC patients (93%) examined by colonoscopy. It is possible that we overlooked the endoscopic findings, as we did not perform a careful total colonoscopy because the symptoms of IBD are mild and the endoscopic findings of the colon show only slightly abnormal changes. The second national survey in Japan also reported that the incidence of IBD in PSC patients increased to 61% when only PSC patients examined by total colonoscopy were enrolled[11]. Therefore, the frequency of PSC-IBD should be evaluated among patients undergoing careful total colonoscopy. This selection criterion might decrease the observed differences in frequency between eastern and western countries.
The age at clinical onset of IBD is controversial and has not been clarified. Loftus et al[9] reported that the mean age of IBD diagnosis was higher among PSC-IBD patients (32 years) compared with controls (28 years). In contrast, Brackmann et al[16] reported that IBD patients with PSC were significantly younger at the onset of IBD symptoms (PSC: 19 years vs no PSC: 29 years; P = 0.04), whereas the colitis-colorectal cancer interval was similar to that of IBD patients without PSC (17 years vs 20 years; P = 0.236). Joo et al[4] showed that PSC patients with UC presented with UC at a significantly earlier age (mean age: 24.5 years) compared with UC controls (mean age: 33.8 years).
Takikawa et al[10,11] discovered two peaks in the PSC age distribution, which has never been observed in other countries, and revealed that most Japanese PSC patients associated with IBD were adolescents or young adults. A recent study from Canada also reported two peaks in the PSC age distribution[17]. Our previous study also showed a two-peaked age distribution, and that patients with PSC-IBD were significantly younger than PSC patients without IBD (33.6 years vs 58.9 years, P < 0.001)[14].
Although the diagnosis of IBD precedes that of PSC in most patients, a recent study found that a shift in the timing of diagnosis of the two diseases has occurred in recent years, with PSC more often being diagnosed first. PSC was diagnosed before IBD in a recent cohort (2003-2007) when compared with a early cohort (1993-1997) (50% vs 35%, P = 0.0009)[18].
MECHANISM OF PSC-IBD PATHOGENESIS
Several important observations, coupled with the strong association between certain human leukocyte antigen (HLA) haplotypes and the frequency of concurrent extrahepatic autoimmune disorders, support the concept that PSC is an immune-mediated phenomenon[19,20]. Three UC susceptibility loci to be associated with PSC, haboring the putative candidate genes REL, IL2 and CARD9 were identified[19]. A recent study reported 12 significant genome-wide associations outside the HLA region, 9 of which were new, increasing the number of known PSC risk loci to 16. Despite comorbidity with IBD in 72% of the included cases, 6 of the 12 loci showed significantly stronger associations with PSC than with IBD, suggesting overlapping yet distinct genetic mechanisms for these two diseases[20].
The pathogenesis of PSC has been elucidated from the standpoint of PSC-IBD. Translocation of microbial flora across an inflamed, permeable gut with subsequent activation of the immune system and inflammation of the biliary tree is a hypothesized mechanism for the development of PSC. Activated intestinal lymphocytes enter the enterohepatic circulation and persist as memory cells that cause hepatic inflammation. Chemokines and adhesion molecules shared by the intestine and liver could contribute to immune cell binding at both sites[21]. The observations that PSC can develop after colectomy[22] and that IBD can develop after liver transplantation[23] have led some investigators to suggest that aberrant homing of lymphocytes between the intestine and liver could be involved in the pathogenesis of PSC[21]. Three recent studies indirectly supporting this theory have been published. Patients who received a liver transplant had lower clinical and histological IBD activity than the non-transplant group[24]. Marelli et al[25] reported that progressive PSC requiring liver transplantation is associated with a milder course of UC, including reduced disease activity and less use of steroids, azathioprine, and surgery. Navaneethan et al[26] reported that severe, progressive PSC requiring liver transplantation appeared to reduce the disease activity of UC and the need for colectomy.
However, these theories cannot explain why only 2%-7.5% of IBD patients develop PSC[8], whereas PSC is strongly associated with IBD, or why CD is less associated with PSC. It is also unclear why immunosuppression does not improve PSC.
CLINICOPATHOLOGIC CHARACTERISTICS OF PSC-IBD
Previous studies have suggested that PSC-IBD differs from IBD without PSC in several aspects. Table 1 summarizes the reports concerning PSC-IBD[3,4,9,14,24,27]. PSC-IBD has been reported to show an increased incidence of pancolitis, rectal sparing, backwash ileitis, mild symptoms, and colorectal malignancy[8]. However, these results are controversial. All of the investigators agree that inflammation involved in PSC-IBD is milder than that in typical UC without PSC. Moreover, the majority of PSC-IBD patients show no or few IBD symptoms. Moayyeri et al[28] reported that the number of hospitalizations and courses of steroid therapy decreased significantly in UC-PSC patients compared with UC controls. Our study also indicated that none of the enrolled patients had a severe clinical course, and that half of them were asymptomatic[14].
Table 1.
character of inflammatory bowel disease-associated with primary sclerosing cholangitis
| Ref./Nation | Year |
Endoscopic/histological findings |
Histological findings | ||
| Extension of IBD | Backwash-ileitis | Rectal sparing | |||
| Loftus et al[9] | 2005 | Total colitis 56/61 (92% vs CUC 54%) | 19/37 (51% vs CUC 7%) by endoscopy | 32/61 (52% vs CUC 6%) by endoscopy | |
| United States | |||||
| Joo et al[4] | 2009 | Total colitis 34/40 (85% vs CUC 45%) | 10/24 (35.7% vs 26.9%) by histology | 11/40 (27.5% vs 25%) by histology | |
| United States | |||||
| Sano et al[14] | 2010 | Total colitis 6/20 (35% vs CUC 35%) | Not studied | Not studied | Significantly higher inflammation in the right colon |
| Japan | Right-sided 11/20 (55% vs 3.3%) | ||||
| Left-sided 1/20(5% vs 31.7%) | |||||
| Jørgensen et al[24] | 2012 | Total colitis 60/110 (55%) | 11/93 (12%) by endoscopy | 73/110 (66%) by endoscopy | Significantly higher inflammation in the right colon |
| Norway | Right-sided 25/110 (23%) | 17/87 (20%) by histology | 70/107 (65%) by histology | ||
| Left-sided 3/110 (3%) | |||||
| Boonstra et al[3] | 2012 | Total colitis 207/380 (83%) | < 10% | < 10% | |
| The Netherlands | Left-sided 9/380 (4%) | ||||
| Schaeffer et al[27] | 2013 | Total colitis (IBD preceding PSC) | |||
| Canada | Right-sided (PSC following IBD) | ||||
CUC: Chronic ulcerative colitis; IBD: Inflammatory bowel disease; PSC: Primary sclerosing cholangitis.
However, varied findings concerning the extent of PSC-IBD have been reported. Although some authors have reported that pancolitis is characteristic of PSC-IBD[3,4,9], others have insisted that right-sided IBD is characteristic[14,24]. A recent report concluded that when IBD precedes PSC, pancolitis is common, whereas when PSC precedes IBD, right-sided IBD is common[27].
Two reports revealed that the degree of inflammation was stronger in the right colon than the left colon using the histological studies. The first report demonstrated severe inflammatory cell infiltration in the cecum and ascending colon of PSC-IBD patients, whereas the degree was mild in the rectum/descending colon (P = 0.0012); goblet cell disappearance was also observed more frequently in the cecum/ascending colon than in the rectum/descending colon (P < 0.05)[14]. The second report revealed that the histopathological signs of inflammation involved the right colon in 86% of patients and were purely right-sided in 23%. The frequency of inflammatory findings was higher in the right colon than the left colon (P < 0.01), but the general level of inflammatory activity was low[24]. They also reported that inflammatory findings were more frequent on histology than on endoscopy.
These discrepancies may be due to differences in the geographical location between studies or the method used to assess total colitis based on the maximal extent of colitis at any time during the study period. Fluctuations in the extent of inflammation may therefore explain the high frequency of total colitis[24,29].
The frequency of rectal sparing and backwash ileitis differs between reports, with the frequency of backwash ileitis ranging from < 10% to 51%. Jørgensen et al[24] speculated that repeated examination or different patient selection criteria account for these differing results, and also reported that the frequency of rectal sparing on histological examination (20%) was higher than that on endoscopic examination (12%). Nakazawa et al[5] speculated that the different results were due to the definition and criteria of backwash ileitis.
The frequency of rectal sparing ranges from < 10% to 66%. Loftus et al[9] reported that rectal sparing was observed in 52% of UC-PSC patients compared with only 6% of UC patients without PSC on endoscopy. Jørgensen et al[24] reported that rectal sparing was observed in 66% of patients on endoscopy and was consistent with the results of pathological examination. In their study, the patients were considered to have rectal sparing if the inflammation involved the rectum but was less severe than that of the more proximal area of the colon. Joo et al[4] reported that rectal sparing was observed in only 27.5% of patients on histologic studies. Rectal sparing was defined as predilection if all biopsies from the rectum or the entire rectal mucosa from a resection specimen showed histologically normal mucosa. Rectal sparing was considered relative if at least one biopsy from the rectum at any time period or one portion of the rectal mucosa from the colonic resection specimen showed histologic features of chronicity, but at least mild activity was present in the areas of the mucosa proximal to the rectum.
The extent of colon involvement, rectal sparing, and backwash ileitis should be defined internationally to clarify the characteristics of PSC-IBD.
In our experiences with endoscopy, inflammation was more severe on the right, and rectal sparing appeared to be present on endoscopy (Figures 1 and 2), by contrast, less inflammatory cell infiltrations was observed in the rectum on histology. These findings are very useful in the diagnosis of PSC. In the presence of multiple biliary stenoses on magnetic resonance cholangiography, inflammatory findings dominant in the right colon and rectal sparing by total colonoscopy, invasive endoscopic retrograde cholangiography can be avoided in clinical practice.
Figure 1.
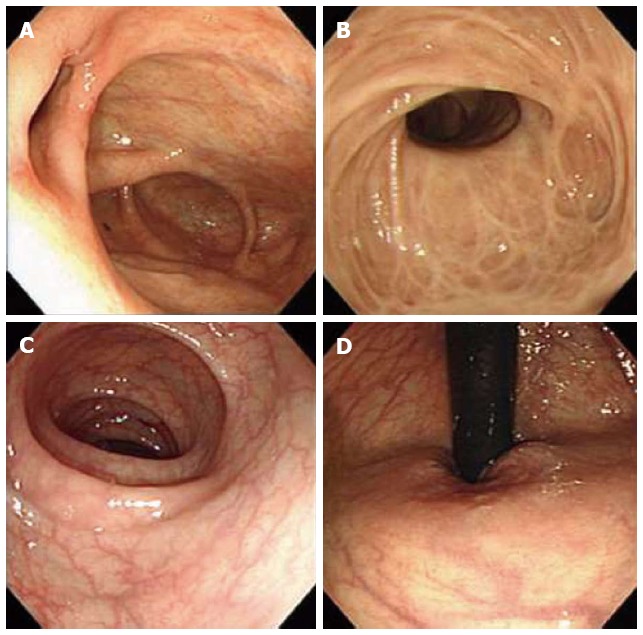
Colonoscopic findings at clinical onset. A: Cecum; B: Ascending colon; C: Sigmoid colon; D: Rectum. A 43-year-old female patient diagnosed with asymptomatic, concurrent primary sclerosing cholangitis-inflammatory bowel disease. The first colonoscopy showed multiple white scars in the ascending colon and right-sided transverse colon and no abnormal findings in the left-sided transverse colon, descending colon, sigmoid colon, or rectum.
Figure 2.
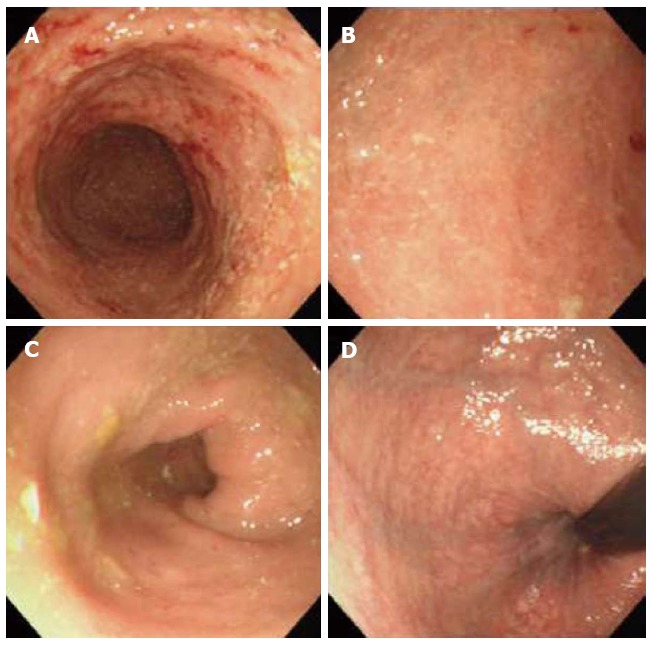
Colonoscopic findings seven months later. A: Cecum; B: Ascending colon; C: Sigmoid colon; D: Rectum. A repeat colonoscopy seven months later showing inflamed mucosa with multiple erosions and redness from the ascending colon to the right-sided transverse colon. Mucosal vessels are clearly visible in the descending colon, sigmoid colon, and rectum.
COLORECTAL NEOPLASIA IN PSC-IBD PATIENTS
PSC-IBD patients are at particularly high risk for the development of colorectal cancer. Boonstra et al[3] estimated that the colorectal cancer risk was increased 10-fold in PSC-IBD patients compared with UC controls. Claessen et al[29] have reported that patients with PSC-IBD have a high long-term risk of developing colorectal cancer, and that this risk is approximately three-fold higher than that of cholangiocarcinoma. In patients with PSC-IBD, the 10-year and 20-year risks of colorectal cancer have been reported to be 14% and 31%, respectively. Among 75 PSC-IBD patients, PSC was the only independent risk factor for the development of colorectal cancer, and the overall survival rate without liver transplantation was also reduced[30].
PSC-IBD patients tend to be younger at colorectal cancer diagnosis[31]. Colorectal cancer develops at a much younger age in these patients (39 years, range: 26-64 years) compared with IBD controls (59 years, range: 34-73) (P = 0.019)[3].
Colorectal cancer in PSC-IBD patients predominantly develops in the right colon. The tumors were located proximally to the splenic flexure in 18 (67%) patients with PSC and in 52 (36%) patients without PSC (P = 0.006)[29]. Thackeray et al[32] also reported that colorectal cancer is most prevalent in the proximal colon (65%). When such patients are diagnosed with cancer, they tend to have more advanced tumors than IBD patients without concurrent PSC. In their study, patients with PSC had significantly more tumors with an American Joint Committee on Cancer tumor stage of 3A or higher when compared with patients with IBD alone (61.5% and 38.5%, P = 0.003). The reason for the preferential right-sided location of colorectal cancer in PSC patients remains unknown, although it has been speculated that the overall increased frequency of colorectal cancer in these patients could be due to a cytotoxic effect on the colonic mucosa caused by an altered bile acid composition. The predominance of right-sided inflammation is also a predisposing factor[24]. The two reports showing that the histologic findings of inflammation were higher in the right compared to the left colon in PSC-IBD patients are consistent with the preferential right-sided location of colorectal cancer[14,24].
Previous studies have shown conflicting results regarding the course of IBD after liver transplantation in patients with PSC. Recent studies have shown that the increased risk of neoplasia is maintained after liver transplant and proctocolectomy. Hanouneh et al[33] reported that patients with PSC-IBD after liver transplantation had a similar rate of colon neoplasia compared to those without liver transplantation (34% vs 30%, P = 0.24) during a mean follow-up period of 54.7 ± 47.7 mo. Jørgensen et al[24] showed that macroscopic colonic inflammation was more frequent after liver transplantation than before transplantation. The rate of relapse after transplantation was higher than that before transplantation, and the overall clinical IBD activity was also increased. Immunosuppression affects IBD activity after liver transplantation in patients with PSC.
Early cancer detection through enrollment in surveillance programs is the only strategy available to decrease cancer risk[31]. More extensive colitis with a concurrent mild or even asymptomatic course, resulting in diagnostic delay and a lower colectomy rate, may contribute to an increased risk of colorectal cancer development[9]. With the initial diagnosis of PSC in subjects with IBD, immediate and annual surveillance colonoscopy and biopsy analysis, of the entire colon, are recommended[32,34].
The role of ursodeoxycholic acid (UDCA) as a chemopreventive agent is controversial. A meta-analysis showed no significant protective association between UDCA use and colorectal neoplasia. However, there was a significant chemopreventive effect on the risk of advanced colorectal neoplasia (OR = 0.35, 95%CI: 0.17-0.73), and low-dose UDCA use (8-15 mg/kg per day) was associated with a significantly reduced risk of colorectal neoplasia[35]. There were no significant differences in cholangiocarcinoma incidence between the high-dose UDCA (17-23 mg/kg per·day) and placebo groups[36]. A recent study showed that patients treated with high-dose UDCA had a significantly higher risk of developing colorectal neoplasia during the study compared with those who received placebo (HR = 4.4, P = 0.02)[37].
THE USEFULNESS OF PSC-IBD CHARACTERISTICS IN THE DIAGNOSIS OF SCLEROSING CHOLANGITIS
Recently, IgG4-SC has attracted much attention following the emergence of clinical characteristics that distinguish it as a new clinical entity[5]. IgG4-SC shows various cholangiographic features similar to those of pancreatic cancer, PSC, and cholangiocarcinoma[7]. The characteristic cholangiographic features of IgG4-SC can be classified into four types based on the stricture location revealed by cholangiography and differential diagnosis[6]. Type 2 IgG4-SC, in which stenosis is diffusely distributed throughout the intrahepatic and extrahepatic bile ducts, should be differentiated from PSC[38] (Figure 3).
Figure 3.
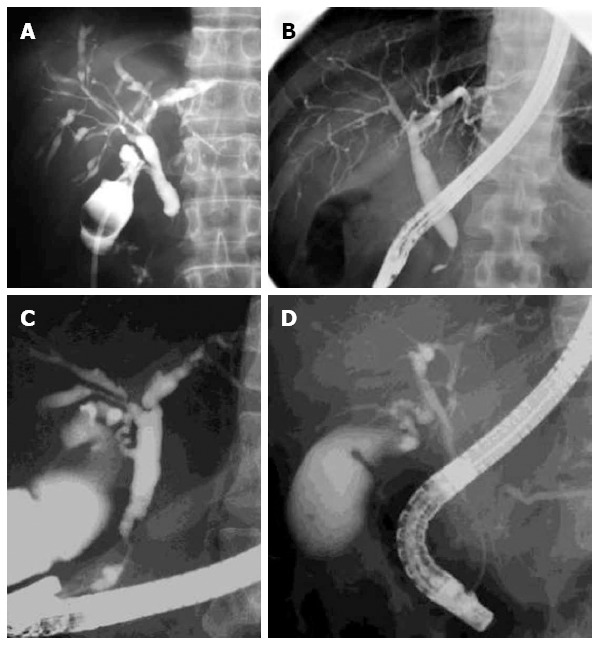
Cholangiographic examples of immunoglobulin G4-related sclerosing cholangitis and primary sclerosing cholangitis. Cholangiograms of immunoglobulin G4-related sclerosing cholangitis showing multiple stenoses in the intrahepatic ducts and stenosis in the intrapancreatic portion (A, B). Cholangiograms of primary sclerosing cholangitis showing a beaded appearance (C) and pruning of the intrahepatic ducts (C, D).
The differential diagnosis of PSC and IgG4-SC is important because patients with IgG4-SC show a good response to steroid therapy. We previously reported the differences between IgG4-SC and PSC[7]. The age at clinical onset was significantly higher for IgG4-SC patients. Among the chief complaints in IgG4-SC, obstructive jaundice, reflecting marked concentric stenosis of the large bile duct, was most frequently observed. An elevated serum IgG4 level is a characteristic feature of IgG4-SC[39]. An elevated serum IgG4 level and the association with type 1 autoimmune pancreatitis (AIP) are the most useful findings for discriminating between IgG4-SC and PSC[6]. However, elevation of the serum IgG4 level alone is not useful because some PSC cases also show increased IgG4 levels. In addition, some IgG4-SC cases are not associated with AIP[40]. Mendes et al[41] measured the serum IgG4 levels in 127 patients with PSC and found that it was elevated in 12 patients (9%). Björnsson et al[42] reported elevated serum IgG4 levels in 12% of 285 patients with classic PSC. We performed a multicenter study in Japan to establish a cutoff value to differentiate IgG4-SC from controls[43]. Serum IgG4 levels were compared between 56 patients with type 2 IgG4-SC and 110 patients with PSC. The serum IgG4 levels of the IgG4-SC patients were significantly higher than those of the PSC patients (799 ± 800 mg/dL vs 68.7 ± 86.0 mg/dL, respectively, P < 0.001). When we set the IgG4 cutoff value at 135 mg/dL, the sensitivity, specificity, and accuracy were 94.5%, 85.0%, and 90.5%, respectively. We also identified 13 of the 110 PSC patients (11.8%) with IgG4 values higher than the cutoff value of 135 mg/dL[43] Further studies are expected to clarify the differences between IgG4-SC and PSC patients with high serum IgG4 levels.
In contrast, the diagnosis of PSC is difficult because there are no useful markers of PSC. As such, an association with IBD is a very useful finding in the diagnosis of PSC. The frequencies of IBD associated with IgG4-SC are summarized in Table 2[5,41,44-46]. No association between IBD and IgG4-SC has been reported, which is in contrast to the strong association between IBD and PSC (60%-80%)[5,44-46]. One study reported that 6% of IgG4-SC cases were associated with IBD[46], as IBD is common in western countries. We are unable to describe the details of IBD-associated IgG4-SC, although we speculate that the unique characteristics of PSC-IBD can be used to distinguish PSC from IgG4-SC.
Table 2.
Inflammatory bowel disease association in sclerosing cholangitis n (%)
| Ref. | IgG4-SC | PSC | |
| Nishino et al[44] | 0/24 (0) | 15/24 (62.5) | P < 0.0001 |
| Zen et al[45] | 0/17 (0) | 5/5 (100) | P < 0.0001 |
| Ghazale et al[46] | 3/53 (6) | 70% | |
| Mendes et al[41] | NA | Elevated group (n = 12) | |
| 6/12 (50) | |||
| Normal group (n = 115) | |||
| 97/115 (90) | |||
| Nakazawa et al[5] | 0/62 (0) | 21/31 (68) | P < 0.0001 |
IgG4-SC: Immunoglobulin G4-related sclerosing cholangitis; PSC: Primary sclerosing cholangitis.
IgG4-SC is frequently associated with type 1 AIP[5]. Type 1 AIP is a different clinical entity from type 2 AIP, which is closely associated with IBD. Type 2 AIP is not associated with IgG4-related diseases, including IgG4-SC, and elevated serum IgG4 levels are not observed[47]. Clinically diagnosed IBD is incorporated in the diagnostic criteria for type 2 AIP in international consensus diagnostic criteria for autoimmune pancreatitis[47]. These complicated associations are illustrated in Figure 4. There are no reports concerning the characteristics of IBD associated with type 2 AIP. If IBD associated with type 2 AIP shows characteristic findings, they might be useful not only in discriminating type2 AIP from type1 AIP, but also in elucidating the mechanism of sclerosing cholangitis.
Figure 4.
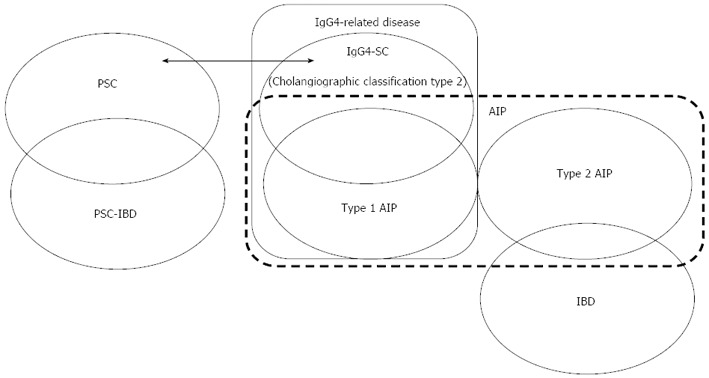
Correlation between inflammatory bowel disease and screrosing cholangitis. PSC is frequently associated with characteristic PSC-IBD, whereas IgG4-SC is not associated with IBD. IgG4-SC is frequently associated with type 1 AIP, whereas type 2 AIP is frequently associated with IBD. PSC: Primary sclerosing cholangitis; PSC-IBD: IBD-associated with PSC; IBD: Inflammatory bowel disease; IgG4-SC: Immunoglobulin G4-related sclerosing cholangitis; AIP: Autoimmune pancreatitis.
In summary, PSC-IBD is associated with an increased incidence of pancolitis, mild symptoms and colorectal malignancy. Although an increased incidence of pancolitis is also a characteristic finding, some cases are endoscopically diagnosed as right-sided UC. Pathological studies have revealed that the findings of inflammation were more prevalent in the right colon than the left colon. The frequency of rectal sparing and backwash ileitis should be investigated in a future study based on the same definition. The rare association between IBD and IgG4-SC and the unique characteristics of PSC-IBD are useful for discriminating between PSC and IgG4-SC. In particular, when IBD is characterized by right-sided UC, rectal sparing, and backwash ileitis, the possible diagnosis of PSC-IBD should be considered. In the presence of multiple biliary stenoses on magnetic resonance cholangiography, inflammatory findings dominant in the right colon and rectal sparing by total colonoscopy, invasive endoscopic retrograde cholangiography can be avoided in clinical practice.
Footnotes
P- Reviewers: Invernizzi P, Kawa S, Maggiore G, Mulder CJJ, Neuberger J, Roeb E S- Editor: Ma YJ L- Editor: A E- Editor: Zhang DN
References
- 1.Lazaridis KN, Wiesner RH, Porayko MK, Ludwig J, LaRusso NF. Primary sclerosing cholangitis. In: Schiff ER, Sorrel MF, Maddrey WC, editors. Schiff’s disease of the liver. English Edition. Philadelphia: Lippincott-Raven; 1999. pp. 649–678. [Google Scholar]
- 2.Lindor KD, LaRusso NF. Primary sclerosing cholangitis. In: Schiff L, Schiff ER, editors. Schiff’s disease of the liver. 9 ed. Philadelphia: JB Lippincott; 2003. pp. 673–684. [Google Scholar]
- 3.Boonstra K, van Erpecum KJ, van Nieuwkerk KM, Drenth JP, Poen AC, Witteman BJ, Tuynman HA, Beuers U, Ponsioen CY. Primary sclerosing cholangitis is associated with a distinct phenotype of inflammatory bowel disease. Inflamm Bowel Dis. 2012;18:2270–2276. doi: 10.1002/ibd.22938. [DOI] [PubMed] [Google Scholar]
- 4.Joo M, Abreu-e-Lima P, Farraye F, Smith T, Swaroop P, Gardner L, Lauwers GY, Odze RD. Pathologic features of ulcerative colitis in patients with primary sclerosing cholangitis: a case-control study. Am J Surg Pathol. 2009;33:854–862. doi: 10.1097/PAS.0b013e318196d018. [DOI] [PubMed] [Google Scholar]
- 5.Nakazawa T, Naitoh I, Hayashi K, Okumura F, Miyabe K, Yoshida M, Yamashita H, Ohara H, Joh T. Diagnostic criteria for IgG4-related sclerosing cholangitis based on cholangiographic classification. J Gastroenterol. 2012;47:79–87. doi: 10.1007/s00535-011-0465-z. [DOI] [PubMed] [Google Scholar]
- 6.Nakazawa T, Ohara H, Sano H, Ando T, Joh T. Schematic classification of sclerosing cholangitis with autoimmune pancreatitis by cholangiography. Pancreas. 2006;32:229. doi: 10.1097/01.mpa.0000202941.85955.07. [DOI] [PubMed] [Google Scholar]
- 7.Nakazawa T, Ohara H, Sano H, Ando T, Aoki S, Kobayashi S, Okamoto T, Nomura T, Joh T, Itoh M. Clinical differences between primary sclerosing cholangitis and sclerosing cholangitis with autoimmune pancreatitis. Pancreas. 2005;30:20–25. [PubMed] [Google Scholar]
- 8.Eaton JE, Talwalkar JA, Lazaridis KN, Gores GJ, Lindor KD. Pathogenesis of primary sclerosing cholangitis and advances in diagnosis and management. Gastroenterology. 2013;145:521–536. doi: 10.1053/j.gastro.2013.06.052. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Loftus EV, Harewood GC, Loftus CG, Tremaine WJ, Harmsen WS, Zinsmeister AR, Jewell DA, Sandborn WJ. PSC-IBD: a unique form of inflammatory bowel disease associated with primary sclerosing cholangitis. Gut. 2005;54:91–96. doi: 10.1136/gut.2004.046615. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Takikawa H, Manabe T. Primary sclerosing cholangitis in Japan--analysis of 192 cases. J Gastroenterol. 1997;32:134–137. doi: 10.1007/BF01213311. [DOI] [PubMed] [Google Scholar]
- 11.Takikawa H, Takamori Y, Tanaka A, Kurihara H, Nakanuma Y. Analysis of 388 cases of primary sclerosing cholangitis in Japan; Presence of a subgroup without pancreatic involvement in older patients. Hepatol Res. 2004;29:153–159. doi: 10.1016/j.hepres.2004.03.006. [DOI] [PubMed] [Google Scholar]
- 12.Ang TL, Fock KM, Ng TM, Teo EK, Chua TS, Tan JY. Clinical profile of primary sclerosing cholangitis in Singapore. J Gastroenterol Hepatol. 2002;17:908–913. doi: 10.1046/j.1440-1746.2002.02835.x. [DOI] [PubMed] [Google Scholar]
- 13.Shorbagi A, Bayraktar Y. Primary sclerosing cholangitis--what is the difference between east and west? World J Gastroenterol. 2008;14:3974–3981. doi: 10.3748/wjg.14.3974. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Sano H, Nakazawa T, Ando T, Hayashi K, Naitoh I, Okumura F, Miyabe K, Yoshida M, Takahashi S, Ohara H, et al. Clinical characteristics of inflammatory bowel disease associated with primary sclerosing cholangitis. J Hepatobiliary Pancreat Sci. 2011;18:154–161. doi: 10.1007/s00534-010-0319-8. [DOI] [PubMed] [Google Scholar]
- 15.Yamagishi N, Iizuka B. Ulcerative colitis and primary sclerosing cholangitis: colonoscopic features of concomitant colitis with primary sclerosing cholangitis (in Japanese) Kan Tan Sui. 2004;49:221–228. [Google Scholar]
- 16.Brackmann S, Andersen SN, Aamodt G, Langmark F, Clausen OP, Aadland E, Fausa O, Rydning A, Vatn MH. Relationship between clinical parameters and the colitis-colorectal cancer interval in a cohort of patients with colorectal cancer in inflammatory bowel disease. Scand J Gastroenterol. 2009;44:46–55. doi: 10.1080/00365520801977568. [DOI] [PubMed] [Google Scholar]
- 17.Kaplan GG, Laupland KB, Butzner D, Urbanski SJ, Lee SS. The burden of large and small duct primary sclerosing cholangitis in adults and children: a population-based analysis. Am J Gastroenterol. 2007;102:1042–1049. doi: 10.1111/j.1572-0241.2007.01103.x. [DOI] [PubMed] [Google Scholar]
- 18.Sinakos E, Samuel S, Enders F, Loftus EV, Sandborn WJ, Lindor KD. Inflammatory bowel disease in primary sclerosing cholangitis: a robust yet changing relationship. Inflamm Bowel Dis. 2013;19:1004–1009. doi: 10.1097/MIB.0b013e3182802893. [DOI] [PubMed] [Google Scholar]
- 19.Janse M, Lamberts LE, Franke L, Raychaudhuri S, Ellinghaus E, Muri Boberg K, Melum E, Folseraas T, Schrumpf E, Bergquist A, et al. Three ulcerative colitis susceptibility loci are associated with primary sclerosing cholangitis and indicate a role for IL2, REL, and CARD9. Hepatology. 2011;53:1977–1985. doi: 10.1002/hep.24307. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Liu JZ, Hov JR, Folseraas T, Ellinghaus E, Rushbrook SM, Doncheva NT, Andreassen OA, Weersma RK, Weismüller TJ, Eksteen B, et al. Dense genotyping of immune-related disease regions identifies nine new risk loci for primary sclerosing cholangitis. Nat Genet. 2013;45:670–675. doi: 10.1038/ng.2616. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Grant AJ, Lalor PF, Salmi M, Jalkanen S, Adams DH. Homing of mucosal lymphocytes to the liver in the pathogenesis of hepatic complications of inflammatory bowel disease. Lancet. 2002;359:150–157. doi: 10.1016/S0140-6736(02)07374-9. [DOI] [PubMed] [Google Scholar]
- 22.Cangemi JR, Wiesner RH, Beaver SJ, Ludwig J, MacCarty RL, Dozois RR, Zinsmeister AR, LaRusso NF. Effect of proctocolectomy for chronic ulcerative colitis on the natural history of primary sclerosing cholangitis. Gastroenterology. 1989;96:790–794. [PubMed] [Google Scholar]
- 23.Singh S, Loftus EV, Talwalkar JA. Inflammatory bowel disease after liver transplantation for primary sclerosing cholangitis. Am J Gastroenterol. 2013;108:1417–1425. doi: 10.1038/ajg.2013.163. [DOI] [PubMed] [Google Scholar]
- 24.Jørgensen KK, Grzyb K, Lundin KE, Clausen OP, Aamodt G, Schrumpf E, Vatn MH, Boberg KM. Inflammatory bowel disease in patients with primary sclerosing cholangitis: clinical characterization in liver transplanted and nontransplanted patients. Inflamm Bowel Dis. 2012;18:536–545. doi: 10.1002/ibd.21699. [DOI] [PubMed] [Google Scholar]
- 25.Marelli L, Xirouchakis E, Kalambokis G, Cholongitas E, Hamilton MI, Burroughs AK. Does the severity of primary sclerosing cholangitis influence the clinical course of associated ulcerative colitis? Gut. 2011;60:1224–1228. doi: 10.1136/gut.2010.235408. [DOI] [PubMed] [Google Scholar]
- 26.Navaneethan U, Venkatesh PG, Mukewar S, Lashner BA, Remzi FH, McCullough AJ, Kiran RP, Shen B, Fung JJ. Progressive primary sclerosing cholangitis requiring liver transplantation is associated with reduced need for colectomy in patients with ulcerative colitis. Clin Gastroenterol Hepatol. 2012;10:540–546. doi: 10.1016/j.cgh.2012.01.006. [DOI] [PubMed] [Google Scholar]
- 27.Schaeffer DF, Win LL, Hafezi-Bakhtiari S, Cino M, Hirschfield GM, El-Zimaity H. The phenotypic expression of inflammatory bowel disease in patients with primary sclerosing cholangitis differs in the distribution of colitis. Dig Dis Sci. 2013;58:2608–2614. doi: 10.1007/s10620-013-2697-7. [DOI] [PubMed] [Google Scholar]
- 28.Moayyeri A, Daryani NE, Bahrami H, Haghpanah B, Nayyer-Habibi A, Sadatsafavi M. Clinical course of ulcerative colitis in patients with and without primary sclerosing cholangitis. J Gastroenterol Hepatol. 2005;20:366–370. doi: 10.1111/j.1440-1746.2005.03727.x. [DOI] [PubMed] [Google Scholar]
- 29.Claessen MM, Lutgens MW, van Buuren HR, Oldenburg B, Stokkers PC, van der Woude CJ, Hommes DW, de Jong DJ, Dijkstra G, van Bodegraven AA, et al. More right-sided IBD-associated colorectal cancer in patients with primary sclerosing cholangitis. Inflamm Bowel Dis. 2009;15:1331–1336. doi: 10.1002/ibd.20886. [DOI] [PubMed] [Google Scholar]
- 30.Sokol H, Cosnes J, Chazouilleres O, Beaugerie L, Tiret E, Poupon R, Seksik P. Disease activity and cancer risk in inflammatory bowel disease associated with primary sclerosing cholangitis. World J Gastroenterol. 2008;14:3497–3503. doi: 10.3748/wjg.14.3497. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Torres J, Pineton de Chambrun G, Itzkowitz S, Sachar DB, Colombel JF. Review article: colorectal neoplasia in patients with primary sclerosing cholangitis and inflammatory bowel disease. Aliment Pharmacol Ther. 2011;34:497–508. doi: 10.1111/j.1365-2036.2011.04753.x. [DOI] [PubMed] [Google Scholar]
- 32.Thackeray EW, Charatcharoenwitthaya P, Elfaki D, Sinakos E, Lindor KD. Colon neoplasms develop early in the course of inflammatory bowel disease and primary sclerosing cholangitis. Clin Gastroenterol Hepatol. 2011;9:52–56. doi: 10.1016/j.cgh.2010.09.020. [DOI] [PubMed] [Google Scholar]
- 33.Hanouneh IA, Macaron C, Lopez R, Zein NN, Lashner BA. Risk of colonic neoplasia after liver transplantation for primary sclerosing cholangitis. Inflamm Bowel Dis. 2012;18:269–274. doi: 10.1002/ibd.21692. [DOI] [PubMed] [Google Scholar]
- 34.Razumilava N, Gores GJ, Lindor KD. Cancer surveillance in patients with primary sclerosing cholangitis. Hepatology. 2011;54:1842–1852. doi: 10.1002/hep.24570. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Singh S, Khanna S, Pardi DS, Loftus EV, Talwalkar JA. Effect of ursodeoxycholic acid use on the risk of colorectal neoplasia in patients with primary sclerosing cholangitis and inflammatory bowel disease: a systematic review and meta-analysis. Inflamm Bowel Dis. 2013;19:1631–1638. doi: 10.1097/MIB.0b013e318286fa61. [DOI] [PubMed] [Google Scholar]
- 36.Olsson R, Boberg KM, de Muckadell OS, Lindgren S, Hultcrantz R, Folvik G, Bell H, Gangsøy-Kristiansen M, Matre J, Rydning A, et al. High-dose ursodeoxycholic acid in primary sclerosing cholangitis: a 5-year multicenter, randomized, controlled study. Gastroenterology. 2005;129:1464–1472. doi: 10.1053/j.gastro.2005.08.017. [DOI] [PubMed] [Google Scholar]
- 37.Eaton JE, Silveira MG, Pardi DS, Sinakos E, Kowdley KV, Luketic VA, Harrison ME, McCashland T, Befeler AS, Harnois D, et al. High-dose ursodeoxycholic acid is associated with the development of colorectal neoplasia in patients with ulcerative colitis and primary sclerosing cholangitis. Am J Gastroenterol. 2011;106:1638–1645. doi: 10.1038/ajg.2011.156. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Nakazawa T, Ohara H, Sano H, Aoki S, Kobayashi S, Okamoto T, Imai H, Nomura T, Joh T, Itoh M. Cholangiography can discriminate sclerosing cholangitis with autoimmune pancreatitis from primary sclerosing cholangitis. Gastrointest Endosc. 2004;60:937–944. doi: 10.1016/s0016-5107(04)02229-1. [DOI] [PubMed] [Google Scholar]
- 39.Hamano H, Kawa S, Horiuchi A, Unno H, Furuya N, Akamatsu T, Fukushima M, Nikaido T, Nakayama K, Usuda N, et al. High serum IgG4 concentrations in patients with sclerosing pancreatitis. N Engl J Med. 2001;344:732–738. doi: 10.1056/NEJM200103083441005. [DOI] [PubMed] [Google Scholar]
- 40.Hamano H, Kawa S, Uehara T, Ochi Y, Takayama M, Komatsu K, Muraki T, Umino J, Kiyosawa K, Miyagawa S. Immunoglobulin G4-related lymphoplasmacytic sclerosing cholangitis that mimics infiltrating hilar cholangiocarcinoma: part of a spectrum of autoimmune pancreatitis? Gastrointest Endosc. 2005;62:152–157. doi: 10.1016/s0016-5107(05)00561-4. [DOI] [PubMed] [Google Scholar]
- 41.Mendes FD, Jorgensen R, Keach J, Katzmann JA, Smyrk T, Donlinger J, Chari S, Lindor KD. Elevated serum IgG4 concentration in patients with primary sclerosing cholangitis. Am J Gastroenterol. 2006;101:2070–2075. doi: 10.1111/j.1572-0241.2006.00772.x. [DOI] [PubMed] [Google Scholar]
- 42.Björnsson E, Chari S, Silveira M, Gossard A, Takahashi N, Smyrk T, Lindor K. Primary sclerosing cholangitis associated with elevated immunoglobulin G4: clinical characteristics and response to therapy. Am J Ther. 2011;18:198–205. doi: 10.1097/MJT.0b013e3181c9dac6. [DOI] [PubMed] [Google Scholar]
- 43.Ohara H, Nakazawa T, Kawa S, Kamisawa T, Shimosegawa T, Uchida K, Hirano K, Nishino T, Hamano H, Kanno A, et al. Establishment of a serum IgG4 cut-off value for the differential diagnosis of IgG4-related sclerosing cholangitis: a Japanese cohort. J Gastroenterol Hepatol. 2013;28:1247–1251. doi: 10.1111/jgh.12248. [DOI] [PubMed] [Google Scholar]
- 44.Nishino T, Oyama H, Hashimoto E, Toki F, Oi I, Kobayashi M, Shiratori K. Clinicopathological differentiation between sclerosing cholangitis with autoimmune pancreatitis and primary sclerosing cholangitis. J Gastroenterol. 2007;42:550–559. doi: 10.1007/s00535-007-2038-8. [DOI] [PubMed] [Google Scholar]
- 45.Zen Y, Harada K, Sasaki M, Sato Y, Tsuneyama K, Haratake J, Kurumaya H, Katayanagi K, Masuda S, Niwa H, et al. IgG4-related sclerosing cholangitis with and without hepatic inflammatory pseudotumor, and sclerosing pancreatitis-associated sclerosing cholangitis: do they belong to a spectrum of sclerosing pancreatitis? Am J Surg Pathol. 2004;28:1193–1203. doi: 10.1097/01.pas.0000136449.37936.6c. [DOI] [PubMed] [Google Scholar]
- 46.Ghazale A, Chari ST, Zhang L, Smyrk TC, Takahashi N, Levy MJ, Topazian MD, Clain JE, Pearson RK, Petersen BT, et al. Immunoglobulin G4-associated cholangitis: clinical profile and response to therapy. Gastroenterology. 2008;134:706–715. doi: 10.1053/j.gastro.2007.12.009. [DOI] [PubMed] [Google Scholar]
- 47.Shimosegawa T, Chari ST, Frulloni L, Kamisawa T, Kawa S, Mino-Kenudson M, Kim MH, Klöppel G, Lerch MM, Löhr M, et al. International consensus diagnostic criteria for autoimmune pancreatitis: guidelines of the International Association of Pancreatology. Pancreas. 2011;40:352–358. doi: 10.1097/MPA.0b013e3182142fd2. [DOI] [PubMed] [Google Scholar]