

Abstract
Objective. To investigate the moral development of pharmacy students over their first academic year of study at a university in the United Kingdom.
Methods. Pharmacy students completed Defining Issues Test (DIT) at the start of their first year (phase 1) and again at the end of their first year (phase 2) of the program.
Results. Pharmacy students (N=116) had significantly higher moral reasoning at the beginning of their first year than by the end of it. Scores differed by students’ gender and age; however, these findings differed between phase 1 and phase 2.
Conclusion. First-year pharmacy students in the United Kingdom scored lower on moral reasoning than did pharmacy students in the United States and Canada.
Keywords: moral development, pharmacy students, moral reasoning
INTRODUCTION
Professionalism among health professions students is an important issue. An integral component of professionalism relates to moral development.1,2 Latif reported that health professions students, including pharmacy students, who scored higher on measures of moral development behaved more professionally in clinical decision-making situations.3 Therefore, it is important for pharmacy educators to understand the moral development of their students. Higher scores in measures of moral development increase the probability of adhering to a profession’s code of ethics and increase the quality of patient care.3,4 Kohlberg introduced a theory that described the stages of cognitive moral development. Moral reasoning is concerned with the processes individuals go through to arrive at decisions. Although it is not about being morally right or wrong, Kohlbergian theory is hierarchical. There are 3 broad levels of moral development through which individuals advance in their moral reasoning: preconventional, conventional, and postconventional.5 The focus at the preconventional level is on the self and actions are viewed in light of their impact on the self. At the conventional level, individuals strive to uphold the norms and rules of authority because such actions conform to the norms of society. The focus at this level is on relationships. Postconventional-level individuals believe that universal moral principles should guide decision-making. They also understand and usually accept the laws and agreements of society.
The Defining Issues Test (DIT), developed by Rest,6 is the most popular instrument used to measure moral development. In particular, the DIT has been widely used with samples of undergraduate students to investigate a broad range of moral issues.7 In their review of 172 studies that have used the DIT on undergraduate students, King and Mayhew found that going to college is beneficial to moral judgement.7 Previous research has also found that female students and older students exhibit stronger ethical attitudes than male students and younger students.8-10 Other studies have suggested that students experience moral development during education differently. Self and colleagues11 found that medical students’ moral reasoning did not develop significantly during their 4 years of medical school to the same extent as that of students in other formal education programs. Patenaude and colleagues suggested that there may be a hidden curriculum within medical education that “inhibits rather than facilitates the development of moral reasoning.”12(p840) Self and colleagues11 suggested that it is the structure of medical education and the medical education environment that inhibits such development.
Latif and colleagues conducted numerous research projects on the moral development of pharmacists and pharmacy students in the United States. Latif and Berger found US pharmacy students are less morally developed than US students in other health professions.13 In another study, Latif found Canadian students scored significantly higher on the DIT than their US counterparts, which may be a result of the different admissions standards in the 2 countries.14 Pharmacy students in the United States scored lower than other healthcare students; however, female pharmacy students scored significantly higher than their male counterparts.8 There were no significant improvements in the moral reasoning abilities and skills of pharmacy students as they progressed through their education, suggesting as Self and colleagues11 did with the medical school curriculum, that pharmacy education may not foster the ethical development of students.
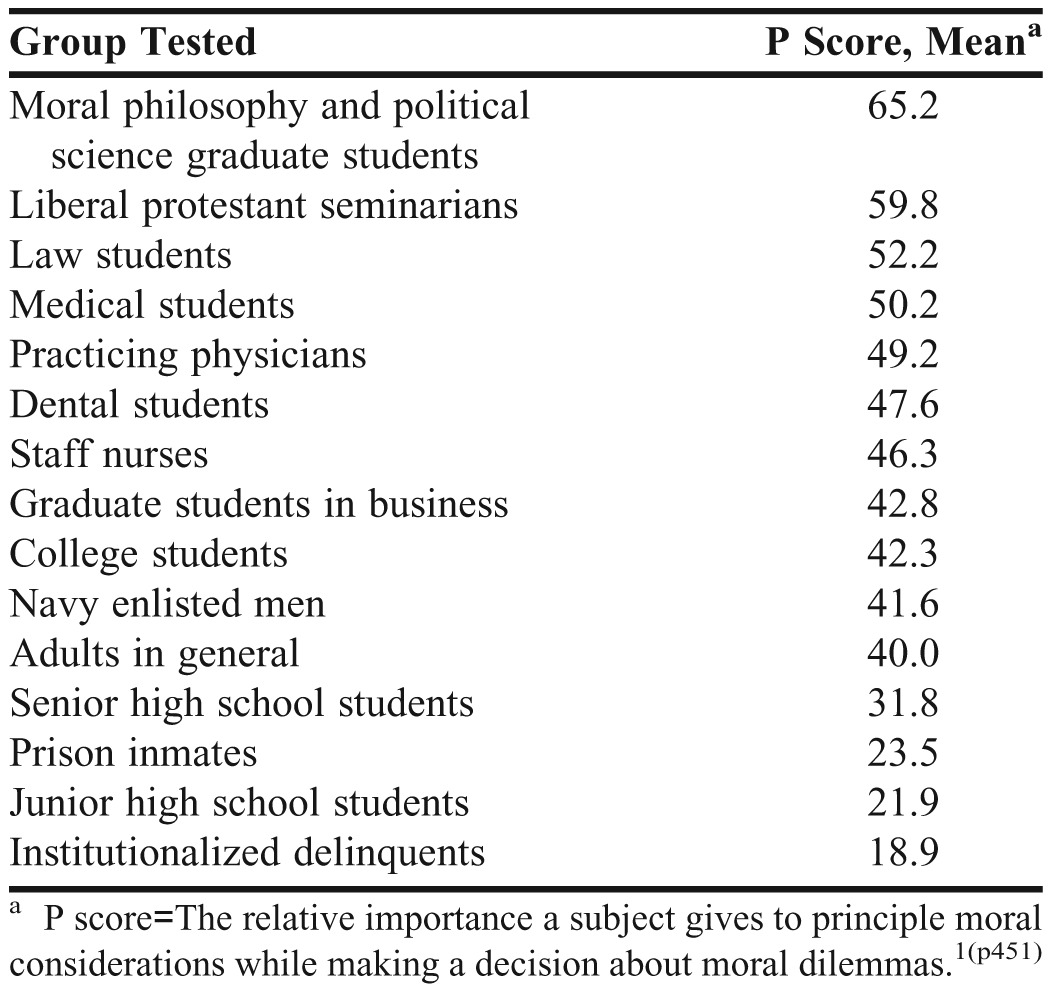
The mean principled (P) scores of different groups who have taken the DIT are shown in Table 1.15 The 1997 and 1998 pharmacy student cohorts in Latif and Berger’s13 study had a mean P score (37.6 and 35.7, respectively) that was above that of senior high school students and just below that of the general adult population.
Table 1.
Scores of Different Groups on the Moral Reasoning Portion of the Defining Issues Test
Much of the research on moral development of pharmacy students has been conducted in the United States. There is a general paucity of research on UK students’ moral development, especially that of pharmacy students. This study aimed to expand the research field by assessing first-year pharmacy students at the University of Central Lancashire, a university in the United Kingdom. We investigated the individual moral development of undergraduate pharmacy students over their first academic year. The purpose of our study was to investigate the moral reasoning of pharmacy students as they started their pharmacy education and again at the end of their first year of study. In particular, the following research question was considered: Does the moral development of pharmacy students increase or decrease throughout their first year of undergraduate study.
METHODS
Ethical approval was granted by the Research Ethics Committee of the School of Pharmacy and Biomedical Sciences, University of Central Lancashire. The DIT is a multiple-choice test that can be group administered and scored electronically by the Office of the Study of Ethical Development at the University of Alabama. The most widely used and reliable score on the DIT is the P score. The P score is “the relative importance a subject gives to principle moral considerations while making a decision about moral dilemmas.”6(p451) “The P score indicates the percent of a person’s reasoning conducted at the highest level of Kohlberg’s model (postconventional).” 11(p452) According to Rest,6 an individual with a P score of >50 is thinking at the highest level of Kohlberg’s model of reasoning; the postconventional level of moral reasoning. Individuals who score <50 are not conceptualizing moral problems the way moral philosophers conceptualize them.
In this longitudinal study, the same students completed the DIT at 2 separate times. First-year pharmacy students completed the DIT at the beginning of their first pharmacy course (phase 1) and again at the end of the year (phase 2). Students were recruited for the study at the start of class, before the lecture began. An explanation of the study was given and students were advised that by completing the test, consent was implied. All students were given the opportunity to opt out of participating.
RESULTS
Of the 118 students who attempted to take the DIT in phase 1, 116 successfully completed it. The mean age of students in phase 1 was 20.1±3.7 years, with most participants (93%) between the ages of 18 and 25 years. Sixty-seven (58%) of the participants were female participants and 49 (42%) were male.
In the phase 2 administration of the DIT, 110 of 114 students within the same student cohort successfully completed the test. The mean age of students in phase 2 was 21.3±3.6 years, with 88 (89%) students between the ages of 18 and 25 years. The majority (62%) of the participants were female.
Descriptive and inferential statistics were conducted using SPSS, version 20(IBM, Armonk, NY). All tests conducted in phase 1 and phase 2 used independent t tests to analyze results. Paired t tests were used to distinguish any differences between variables in phase 1 compared to phase 2.
Of the 116 pharmacy students who completed the DIT in phase 1, the P score mean was 27.2±11.6. The moral reasoning scores were divided into the 3 groups as suggested by Rest,16 low (<27), middle (28 to 41), and high (>42). Students in phase 1 who were <25 years of age had a higher mean score (27.7±11.9) than those >26 years of age (18.5±12.8) (p=<0.05).
The mean P score for the students who took the DIT in phase 2 was 20.9±11.6, indicating that the moral development of the first-year pharmacy students decreased during the academic year. The difference in P scores between phase 1 (27.2±11.6) and phase 2 (20.9±11.6) was significant (p=<0.05).
There was no significant difference between the P score and the age categories for students in phase 2. However, unlike phase 1, there was a significant difference between P scores and gender (p=<0.05) in phase 2. Female students had a significantly higher P score than male students (25.1±12.3 compared to 20.2±11.9, respectively). There was a significant difference in the P score between the genders in the 2 phases (23.9±11.9 for female students and 28.3±11.3 for male students; p=0.05).
Although the mean P score for all students decreased between the 2 time periods, male pharmacy students’ moral development decreased significantly more and was significantly less in phase 2 compared to that of female students. Although female students scored significantly higher than male students, they still scored much lower than students from other disciplines as reported by Rest and Narvaez (Table 1).15
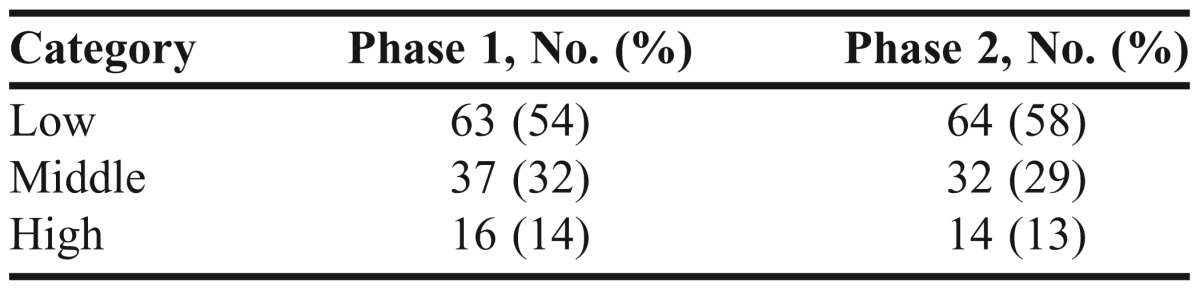
The pharmacy students’ age was significantly related to P score in phase 1 of the study but not in phase 2. At the start of the academic year (phase 1), pharmacy students aged <25 years had a significantly higher mean P score than those aged >26 years. This contradicts previous findings that moral development scores increase by age. Table 2 shows the percentage and number of participants per phase in each of the 3 P score categories: low, medium, and high.
Table 2.
Participants in Each Phase and Category of Moral Reasoning Score
DISCUSSION
This study on UK undergraduate pharmacy students’ moral reasoning skills supports previous findings; in particular, those on US pharmacy students conducted by Latif 3,4,8,13,14 that pharmacy students have lower levels of moral development than other health professions students. The mean P score for first-year UK pharmacy students was lower than the mean scores for US pharmacy students and other US healthcare students. Some undergraduate courses may in fact reduce or inhibit moral development rather than enhance it. As Latif noted, moral development theory posits a positive relationship between years of education and moral development, yet research of healthcare professionals does not support this. Conversely, the research already cited suggests a negative relationship. Additionally, research suggests that pharmacy students have lower moral reasoning scores than other healthcare students. There are several possible explanations for these differences.
From the research by Self and colleagues on medical students, some courses inhibit rather than encourage moral reasoning because of the curriculum and structure of the education.11 In medical education, the environment promotes “convergent thinking,” which emphasizes the importance of getting the right answer and conforming, rather than exploring and questioning. They concluded that “maintenance of the rules and regulations of the system” was of great importance. This, according to cognitive moral development theory, reflects a “conventional level” moral ethos, which aligns with the apparent lack of moral development shown in the studies quoted. This might also be explained by the emphasis on relationships, which is a core element of healthcare professions, and again deemed to be at a lower level. This is in line with suggestions that Kohlberg, on whose theory the DIT is based, incorrectly assumed that a focus on relationships was a sign of lower levels of moral development. If this were true, then scoring at the conventional level would be a good thing for healthcare students, as a focus on relationships is an important aspect of their future practice.
This emphasis on relationships is also supported by research into the empathy levels of pharmacy students. In 1 sample of UK pharmacy students, third-year students had more empathy than first-year students.17 This increase in empathy of pharmacy students between the first and third year of education may indicate that pharmacy students are developing the skills necessary for patient-centered care, and prioritizing the norms of pharmacy, perhaps at the expense of more universal principles.
While these arguments may provide some explanation for the decrease in moral development in healthcare students, they do not address the difference between pharmacy students and other healthcare students. Much has been written of the changing role of the pharmacist with the move towards a more patient-centered practice, and it may be that the rapid pace of this change accounts for the differences in DIT scores. Rosenthal and colleagues18 suggested that pharmacy culture has traditionally been more akin to a scientific discipline than a healthcare discipline. The characteristics associated with pharmacy culture, anecdotal but familiar to many (risk aversion, rule following) are at the far end of the convergent thinking continuum, and may explain the measured differences.
The difference in P scores between pharmacy students in this UK study and US students (on whom most studies have focused) may be a feature of the differences in admissions requirements and educational context between countries. In the United States, students are generally expected to have completed at least 2 years of undergraduate study before being accepted into a doctor of pharmacy degree program, and, therefore, are likely to be older and have more undergraduate experience than pharmacy students in the United Kingdom.19 This difference in age and experience may account for the differences in scores.
The current study adds to the literature on student moral development from a UK perspective. What is particularly unique about the current research is that the study design is longitudinal. However, there are several limitations to this study. The sample size of students aged >26 years was small (n=11) when compared to the whole sample and needs to be taken into consideration when discussing the age-related findings. The sample was limited to 1 institution, so the findings cannot be generalized to other UK schools of pharmacy. A longer period of time between the 2 study phases, especially between the first and third years of study, would have enabled comparison with the empathy research findings. Also, the DIT is a US-developed survey instrument and may not be valid in the UK context. More research is needed on non-US pharmacy students to determine if there are any cultural differences in the moral development of pharmacy students as well as other healthcare students in the use of the DIT as a moral development measurement. For instance, The Professional Ethics in Pharmacy test (PEP) developed by Bouad Charr may be a more appropriate measure for pharmacy students.19
CONCLUSION
The moral development of pharmacy students in this study decreased during the first year of pharmacy education, suggesting that UK pharmacy students may not be as morally developed as students in other countries or health disciplines, including other health professions disciplines. While the discussion outlines several contextual reasons for this, there is still insufficient research on the moral development of pharmacy students in the UK and more research is needed.
Given the movement in the United Kingdom and other countries for pharmacists to provide more healthcare and medication advice to patients, it may be time to look more closely at education for moral development. Pharmacy students in the United Kingdom and United States may not be as ethically developed as they should and, perhaps, could be. Future research should investigate possible educational interventions to aid the ethical development of pharmacy students.
ACKNOWLEDGMENTS
The authors thank the School of Pharmacy and Biomedical Sciences (University of Central Lancashire) for their funding support for this project.
REFERENCES
- 1.Wilkinson TJ, Wade WB, Knock LD. A blueprint to assess professionalism: results of a systematic review. Acad Med. 2009;84(5):551–558. doi: 10.1097/ACM.0b013e31819fbaa2. [DOI] [PubMed] [Google Scholar]
- 2.Bebeau MJ. Promoting Ethical Development and Professionalism: Insights from Educational Research in the Professions. Univ St. Thomas Law J. 2008;5(2):366. [Google Scholar]
- 3.Latif DA. Cognitive moral development and pharmacy education. Am J Pharm Educ. 2000;64(1):451–454. [Google Scholar]
- 4.Latif DA. The relationship between ethical dilemma discussion and moral development. Am J Pharm Educ. 2001;64(1):126–133. [Google Scholar]
- 5.Kohlberg L. Stage and sequence: the cognitive developmental approach to socialization. In: Goslin D, editor. Handbook of Socialisation Theory and Research. Chicago, IL: Rand McNally; 1969. pp. 347–480. Rest JR. Development in Judging Moral Issues. Minneapolis, MN: University of Minnesota Press; 1979. [Google Scholar]
- 6.Rest JR. Development in Judging Moral Issues. Minneapolis, MN: University of Minnesota Press; 1979. [Google Scholar]
- 7.King PM, Mayhew MJ. Moral judgement development in higher education: insights from the defining issues test. J Moral Educ. 2002;31(3):247–270. [Google Scholar]
- 8.Latif DA. An assessment of the ethical reasoning of the United States pharmacy students: a national study. Am J Pharm Educ. 2004;68(2):1–10. [Google Scholar]
- 9.Borkowski SC, Urgas YJ. Business students and ethics: a meta-analysis. J Bus Ethics. 1998;17(3):1117–1127. [Google Scholar]
- 10.Weeks WA, Moore CW, McKinney JA, Longenecker JG. The effects of gender and career stage on ethical judgment. J Bus Ethics. 1999;27(4):301–313. [Google Scholar]
- 11.Self DJ, Schrader DE, Baldwin DC, Wolinsky FD. The moral development of medical students: a pilot study of the possible influence of medical education. Med Educ. 1993;27(1):26–34. doi: 10.1111/j.1365-2923.1993.tb00225.x. [DOI] [PubMed] [Google Scholar]
- 12.Patenaude J, Niyonsenga T, Fafard D. Changes in students’ moral development during medical school: a cohort study. CMAJ. 2003;168(7):840–844. [PMC free article] [PubMed] [Google Scholar]
- 13.Latif DA, Berger BA. Cognitive moral development and clinical performance: implications for pharmacy education. Am J Pharm Educ. 1999;63(1):20–27. [Google Scholar]
- 14.Latif DA. An assessment of the level of moral development of American and Canadian pharmacy students. Int J Pharm Pract. 2002;10(3):153–160. [Google Scholar]
- 15.Rest JR, Narvaez D. Moral Development in the Professions: Psychology and Applied Ethics. Hillsdale, NJ: Lawrence Erlbaum Associates; 1994. [Google Scholar]
- 16.Rest JR. DIT Manual. 3rded. Minneapolis, MN: Center for the Study of Ethical Development; 1990. [Google Scholar]
- 17.Prescott J, Wilson S, Becket G. Empathy levels in 1st and 3rd year students in health and non-health disciplines. Am J Pharm Educ. 2012;76(2):Article 24. doi: 10.5688/ajpe76224. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Rosenthal M, Austin Z, Tsuyuki RT. Are pharmacists the ultimate barrier to pharmacy practice change? Can Pharm J. 2010;143(1):37–42. [Google Scholar]
- 19.Bouad Charr B. Professional ethics in pharmacy practice: developing a psychometric measure of moral reasoning. Pharm World Sci. 2009;31(2):439–449. doi: 10.1007/s11096-009-9292-1. [DOI] [PubMed] [Google Scholar]