

Abstract
The 7-valent pneumococcal protein conjugate vaccine (PCV7) has been shown to be highly efficacious against invasive pneumococcal diseases and effective against pneumonia and in reducing otitis media. The introduction of PCV7 has resulted in major changes in the epidemiology of pneumococcal diseases. However, pneumococcal vaccines induce serotype-specific immunity, and a relative increase in non-vaccine serotypes has been reported following the widespread use of PCV7, leading to a need for extended serotype coverage for protection. PCV10 and PCV13 have been licensed on the basis of noninferiority of immunogenicity compared to a licensed conjugate vaccine. In this article, we aimed to review important data regarding the efficacy and effectiveness of the extended-coverage PCVs published or reported thus far and to discuss future implications for pneumococcal vaccines in Korea. After the introduction of PCV10 and PCV13, within a short period of time, evidence of protection conferred by these vaccines against invasive and mucosal infections caused by most of the serotypes included in the vaccines is accumulating. The choice of vaccine should be based on the changes in the dynamics of pneumococcal serotype distribution and diseases in the region where the vaccines are to be used. Continuous surveillance is essential for the appropriate use of pneumococcal vaccines and evaluation of the impact of PCVs on pneumococcal diseases.
Keywords: Pneumococcal vaccines, 10-valent pneumococcal vaccine, 13-valent pneumococcal vaccine
Introduction
Streptococcus pneumoniae (pneumococcus) is an important cause of invasive bacterial infections, including bacteremia and meningitis and is also a common cause of mucosal infections such as acute otitis media (AOM), sinusitis, and pneumonia in children. The capsular polysaccharide is an important virulence factor, and more than 90 serotypes have been identified based on its antigenicity1). Virulence of pneumococci varies by serotype and immunity against pneumococci is serotype-specific. Serotype distribution varies according to age, socioeconomic status, and geographic area, etc. Before the introduction of pneumococcal conjugate vaccines (PCV), serotypes included in the 7-valent pneumococcal protein conjugate vaccine (PCV7) accounted for around 80% of invasive pneumococcal disease (IPD) among young children in the United States (US) and Canada and for 50% or more in other regions2,3). In Korea, common serotypes for pneumococcal diseases or carriage isolates in children included 4, 6A, 6B, 9V, 11, 19A, 19F, and 23F; among these, 6A, 6B, 9V, 14, 19A, 19F, and 23F showed high antibiotic resistance rates4,5,6,7).
PCV7 was licensed in 2000 in the US and has been proven to be safe and effective in preventing disease and deaths caused by pneumococcal serotypes included in the vaccine8). According to the Active Bacterial Core surveillance (ABCs) network, 5 years after introduction of PCV7, IPD declined by 77% among children in the US, with a 98% decline in IPD caused by vaccine serotypes9). However, after the introduction of PCV7, an increase in non-PCV7 serotypes has been reported10). In late 2008 and 2010, 10-valent (PCV10) and 13-valent (PCV13) vaccines were introduced, providing wider serotype coverage (Table 1).
Table 1.
Composition of pneumococcal protein conjugate vaccines

PCV7, 7-valent pneumococcal protein conjugate vaccine; PCV10, 10-valent pneumococcal protein conjugate vaccine; PCV13, 13-valent pneumococcal protein conjugate vaccine; CRM197, Corynebacterium diphtheria toxin mutant 197; NTHi, nontypable Haemophilus influenza protein D.
PCV10 and PCV13 were both approved for the prevention of IPD and AOM caused by the 10 and 13 vaccine serotypes in infants and young children11,12,13,14). These vaccines were licensed based on the World Health Organization (WHO) recommendations, which state that approval of new PCV against IPD should be based on the demonstration of immunologic noninferiority to the licensed PCV715). There were no efficacy or effectiveness data of the extended-valency PCVs at the time of licensure in the US or Europe. Yet publications regarding the efficacy and effectiveness of these vaccines are increasing. PCV7 was first introduced in Korea in November 2003 and has been used as an optional vaccine for children under 5 years of age; PCV10 and PCV13 were both introduced in Korea in July 2010 and replaced PCV7 by the end of the year. It is decided that PCV will be included in the national immunization program of Korea in 2014.
In this article, we aimed to review important data regarding the efficacy and effectiveness of the extended-coverage vaccines published or reported thus far and to discuss future implications for pneumococcal vaccines in Korea.
Nasopharyngeal carriage
Pneumococcus colonizes in the nasopharynx (NP), which serves as a reservoir, and colonized pneumococcus is an important source of person-to-person transmission. Pneumococcus colonized in the NP, especially newly acquired strains, can also spread to surrounding tissue and cause AOM and sinusitis or invade the bloodstream, leading to IPDs such as bacteremia and meningitis16).
With the introduction of PCV7, reduction in the colonization of vaccine-type (VT) strains has been observed in vaccinated subjects, and the resultant transmission reduction led to less colonization among nonvaccinated subjects17,18,19,20,21). Such decrease in VT colonization was accompanied by increase of non-vaccine-type (NVT) colonization in most carriage studies of PCV7, resulting in no significant changes in the overall carriage rates. Ghaffar et al.22) reported the impact of PCV7 in vaccinated subjects (3-dose primary series and booster) in children aged <2 years in a longitudinal study. More than 200 infants were enrolled at 2 months of age and serial NP samples were obtained. While the carriage rate remained at 24%-30% after age 6 months, the VT carriage rate decreased from 18% (12 months of age) to 9% (3 months after the booster). The direct and indirect effects of PCV7 were well studied in a phase III community-randomized efficacy trial of PCV7 among American Indians17). Decrease in VT carriage was shown not only in vaccinated subjects but also in nonvaccinated siblings if they lived in a household or community of PCV7-vaccinated infants and children. This study showed that PCV7 reduces VT colonization and colonization density with an increase in NVT colonization in both vaccinees and household contacts. Similar findings have also been reported in older children and adults who had no history of vaccination21,23).
There are not many studies on the long-term impact of PCV7 immunization on colonization pattern. However, a recent study compared NP carriage serotype distribution between 1995 and 2009 (after 8 years of routine PCV7 immunization) in Atlanta, US, before the introduction of PCV7 and PCV13, respectively24). PCV7 serotypes decreased substantially; however, there was an increase in non-PCV7 serotypes, with serotype 19A as the leading serotype. Forty percent of children in 1995 and 31% in 2009 were colonized with S. pneumoniae and 60% and 0.7% were PCV7 serotypes, respectively. Serotype 6C was the second most common NP carriage serotype in 2009.
After introduction of PCV13, a reduction in PCV13 serotypes was reported25,26,27). Cohen et al.25) reported the impact of PCV13 in France during the transitional period (2010-2011) from PCV7 to PCV13 (69.3% vaccinated with at least 1 dose of PCV13). NP carriage rates for serotypes 19A and 7F, 2 of 6 additional serotypes, were significantly lower in PCV13-vaccinated subjects than that in PCV7-vaccinated subjects. The reduction of serotype 6C, which is not included in PCV13, suggests cross-protection against pneumococcal disease by serotype 6C. Desai et al.26) reported NP carriage during the first 2 years after introduction of PCV13 in the US. From July 2010 to June 2012, findings were compared among the four 6-month study periods. During this period, the proportion of children vaccinated with ≥2 doses of PCV13 increased from 12.7% to 83.3%. Among NP carriage isolates, the proportion of PCV13 serotypes decreased from 29% in the first 6-month period to 10.0%-15.3% in the following periods. Serotype 19A decreased from 25.8% in the first period to 5.8%-10.2%, and non-PCV13 (except 6C) serotypes increased from 63% to 77%-83% in the following periods. Recently, a randomized double-blind trial in Israel directly comparing the impact of PCV13 versus PCV7 on NP colonization was reported27). This study showed that PCV13 reduced NP acquisition of PCV13 additional serotypes 1, 6A, 7F, and 19A, cross-reacting serotype 6C, and the common PCV7 serotype 19F. There were no differences between vaccine groups with the other PCV7 serotypes and serotype 3, and there were too few serotype 5 isolates for comparison. Immunoglobulin G (IgG) titers after vaccination were also measured in this study, and PCV13 elicited higher titers for PCV13 additional serotypes and serotype 19F, and similar or lower responses for the other PCV7 serotypes. The authors speculated that these findings suggest that immunogenic responses may serve as a predictor of vaccine effectiveness through both direct and indirect protection.
The effect of PCV10 on NP carriage is of interest in 2 aspects: the impact on carriage of nontypable Haemophilus influenzae (NTHi) and the impact on S. pneumoniae. PCV10 consists of 10 pneumococcal polysaccharide antigens conjugated to NTHi-derived protein D (PD) as a carrier protein. After the introduction of PCV7, in a study of bacterial colonization other than pneumococcus, increases in NTHi and Staphylococcus aureus carriage were reported in vaccinated children and their parents.28) After the introduction of PCV10, Prymula et al.29) reported NP carriage in subjects who were fully vaccinated with a 2-dose primary series and booster. Compared with the control group, VT serotype carriage was reduced by 22%-35% in those vaccinated with PCV10. For carriage of any H. influenzae, subjects vaccinated with PCV10 showed a nonsignificant increase during the first year after booster vaccination (vaccine efficacy [VE], -3.5%; 95% confidence interval [CI], -30.7% to 18.0%) and a nonsignificant decrease for NTHi carriage (VE, 1.7%; 95% CI, -25.5% to 23.0%). Over the 12-month period during which NP carriage was evaluated, there was no consistent effect on H. influenzae or NTHi carriage. A randomized controlled trial on NP colonization was also reported, and infants (n=780) vaccinated with either PCV7 or PCV10 were followed until they reached 2 years of age30). PCV10 did not show a differential effect on NP NTHi colonization, acquisition, or density compared to PCV7 in healthy children aged up to 2 years. There was also no significant difference in the acquisition or colonization of pneumococci between PCV7 and PCV10 groups. Serotypes 1, 5, and 7F (which are known to be highly invasive with a high case-to-carrier ratio) were rarely detected (0.4% of all samples). Colonization rates of serotypes 6A and 19A were similar in both PCV7 and PCV10 groups. Throughout the follow-up period, 19A was the predominant colonizing serotype, ranging similarly in both groups from 6% to 11%, followed by 11A (2%-6%) and 16F (2%-4%). Although the study was focused on NTHi colonization in healthy children and effect of the vaccine during NTHi disease cannot be speculated, these results imply that PCV10 may not have a herd effect for NTHi.
Changes in circulation and prevalence of colonizing specific serotypes are not directly related to epidemiologic changes in IPD, as different serotypes have different invasiveness capacities21). However, monitoring NP carriage is important in assessing the impact of vaccines on pneumococcal carriage with respect to herd immunity and serotype replacement.
Otitis media
S. pneumoniae, H. influenzae, and Moraxella catarrhalis are among the most common bacterial pathogens that cause AOM31). Among these pathogens S. pneumoniae is the most common, being isolated from middle ear fluid in 20%-60% of patients32,33). Following the introduction of PCVs, numerous studies have evaluated the impact of PCVs on AOM.
Fletcher and Fritzell34) reviewed PCV trials that used otitis media as an endpoint. Five large clinical trials of the efficacy or effectiveness of PCV on AOM were conducted, all with different study designs. One study was conducted in the Northern California Kaiser Permanente (NCKP) Health Services among 23 medical centers in California from 1995 to 1998 using PCV735,36). Two studies were conducted in Finland (the FinOM study) among 8 clinics in 3 Finnish cities between 1995 and 1999 with 2 vaccines, PCV7 and PCV7-OMPC31,37). The Native American Trial was a double-blind, community randomized clinical trial conducted among Navajo and White Mountain Apache children from 1997 to 200038). The fifth study was conducted in the Czech Republic and Slovakia from 2000 to 2004, using the PCV11-PD vaccine (the POET study)39). In all studies, subjects were vaccinated with a 3-dose primary series and a booster dose.
All studies varied in methodology, such as primary endpoint definition (all episodes of AOM versus the first episode of AOM), age of follow-up (up to 2 years of age versus 3.5 years or until 4-5 years age), source of middle ear fluid for culture (tympanocentesis versus spontaneous rupture), and type of randomization (individual versus community-based randomization).
For the microbiological endpoint, the VE against VT-pneumococcal AOM was about 60% across trials. In contrast, the VE for the clinical endpoints varied substantially between trials. The VE was 7% (PCV7/NCKP), 6% (PCV7/FinOM), -1% (PCV7-OMPC/FinOM), and -0.4% (PCV7/Native American Trial). The VE was 34% against first-episode ear, nose, and throat specialist referral cases (PCV11-PD/POET study). This lack of VE against clinically diagnosed AOM episodes reflects the difficulty of assessing the effect of PCV on OM. Without a validated definition or diagnostic criteria, the diagnosis of OM differs widely among clinicians.
For follow-up through 2 years of age for the 5 trials and in long-term follow-up for 2 of the trials (PCV7/NCKP, until 3.5 years age; PCV7/FinOM, until 4-5 years age), the VE was higher in preventing recurrent AOM and reducing the need for tympanostomy tubes. Subjects who participated in the FinOM trial were followed until they reached 13 years of age to evaluate the long-term effect of the vaccine on tympanostomy tube placement40). The impact of the vaccine was age-dependent: from 2 to 5 years of age the VE was 34% (95% CI, 1% to 52%) for PCV7 and that for the age group of 6 to 12-13 years was -13% (95% CI, -137% to 46%). Thus, PCV7 reduced tympanostomy tube placement rates in children aged ≤5 years.
Larger values for VE in preventing recurrent AOM and the reduced need for tympanostomy suggest that prevention of early episodes of AOM through vaccination may prevent subsequent episodes of complicated OM35). Furthermore, a meta-analysis of PCV trials showed that vaccines have a greater impact on more severe forms of AOM41). The effect of PCV on AOM is difficult to estimate; however, rates of otitis-related outpatient medical visits in the US in children aged <2 years decreased by 20% two to three years after PCV7 introduction42). In Australia, within 2.5 years of PCV7 vaccination, myringotomy with ventilation tube insertion decreased by 23% in children <1 year of age43). However, according to a systematic review conducted by Taylor et al.44), physician visits for AOM began to decrease 3-5 years before PCV7 was introduced and continued to decline thereafter. Therefore, the vaccine does provide some protection against AOM, although other factors may have also contributed to the recent decline in AOM.
In the FinOM study, PCV7 was associated with an increase of AOM due to M. catarrhalis and H. influenzae. In contrast, in the POET study, NTHi-associated AOM showed a 35% decrease. However, the case definitions differed in each study, thus the results of these studies are not directly comparable.
A recent study in Spain analyzed the changes in S. pneumoniae isolated from spontaneous middle ear drainage over a 12-year period (1999-2010)45). The 3 most frequent serotypes were 19A (27.8%), 3 (11.2%), and 19F (9.0%). PCV7 serotypes decreased after the introduction of PCV7 in 2001 from 62.4% (1999-2001) to 2.2% (2009-2010). The prevalence of serotypes 1, 5, and 7F were low, but showed an increasing trend during the study period. Serotype 19A increased from 19.7% (1999-2001) to 37.9% (2008-2010), and serotype 3 increased from 5.1% (1999-2001) to 15.0% (2008-2010). AOM caused by 6A did not vary, but serotype 6C showed an increase over time.
A recent report of the efficacy of PCV10 against AOM in children in Panama showed a VE of 56% (95% CI, 13% to 78%) for first episodes of pneumococcal AOM, 67% (95% CI, 17% to 87%) for VT-pneumococcal AOM, and 15% (95% CI, -84% to 61%) for NTHi AOM46). Further surveillance data are needed regarding the epidemiologic changes of NTHi.
No clinical trials have assessed the efficacy of PCV13 on AOM. However, effectiveness data of PCVs against AOM are available from Israel. Three years after the introduction of PCV7, the yearly incidence of AOM caused by VT (PCV7+serotype 6A) decreased by 75% in children <24 months of age47). One year after the introduction of PCV13, the yearly incidence of AOM caused by 5 additional types (excluding serotype 6A) in PCV13 VT decreased by 85% in children in this age group48).
Pneumonia
S. pneumoniae is a leading cause of bacterial pneumonia; however, the definition of pneumonia may vary by physicians and it is difficult to determine the causative agent of pneumonia in children. Moreover, only a small proportion is identified as pneumococcal pneumonia and serotype information remains quite limited.
Owing to these difficulties, a WHO working group developed a standardized definition for reporting evidence of alveolar consolidation on chest radiography49). The efficacy of PCV against pneumonia has been studied in clinical trials evaluating a 9-valent vaccine (PCV9) and a 11-valent vaccine (PCV11) as well as PCV7. PCV9 and PCV11 were experimental vaccines and included serotypes 1 and 5 (PCV9) and serotypes 1, 5, 3, 7F (PCV11) in addition to those included in PCV7. PCV9, and PCV7 vaccines used the nontoxic mutant of diphtheria toxoid, CRM197, as the carrier protein and PCV11 used tetanus toxoid and diphtheria toxoid as the carrier protein. An initial study conducted in the NCKP district showed a VE of 18% against radiologically confirmed pneumonia50), which subsequently increased to 27% after application of the WHO definition of pneumonia51). In studies conducted in Gambia and South Africa where PCV9 was vaccinated for 3 primary doses and no booster, the VE for pneumonia was estimated at 20%-37%52,53,54). In studies conducted in the Philippines where PCV11 was vaccinated with 3 primary doses and no booster, 22.9% reduction was observed55). Based on these studies of PCV7, PCV9, and PCV11, according to a Cochrane systematic review, the VE was 27% (95% CI, 15% to 36%) for WHO radiologically defined pneumonia56). Limited studies have evaluated the direct impact of PCV on pneumococcal pneumonia; however, there are a few reports from various countries that can provide insight on the impact of PCVs on pneumococcal pneumonia. An extensive analysis on the serotype changes of pneumococcal pneumonia from 2000 to 2004 in Uruguay was performed before the introduction of PCV57). Among a total of 387 pneumococcal isolates obtained from blood or pleural fluid, 48% were found in children <2 years of age and 81.1% were identified in children <5 years of age. Serotype 14 (30.5%) was the most prevalent, followed by serotypes 1 (19.9%), 5 (17.8%), and 3 (6.5%). According to this study, PCV7 would cover 60%, PCV10 would cover 83.8%, and PCV13 would cover 93.9% of the serotypes. Subsequently in Uruguay, PCV7 was introduced in March 2008 into the routine vaccination program (2+1 schedule), and PCV7 was replaced by PCV13 in April 2010. The incidence of pneumococcal empyema in children <14 years of age showed a 77% reduction in 2012, compared with the prevaccination period, 2005-200758) (Pirez MC, personal communication, Jun 12, 2013).
To evaluate the impact of PCV vaccination on pneumococcal pneumonia, extensive studies have analyzed changes in hospitalizations associated with all-cause pneumonia. Shortly after the introduction of PCV7 in the US by 2004, hospitalizations for pneumococcal pneumonia in children <2 years of age decreased by 65% and those for all-cause pneumonia decreased by 39%59). Reductions in childhood pneumonia have been reported in other countries after the introduction of PCV7. Within 30 months of PCV7 introduction in Australia, all-cause pneumonia decreased by 36% in children <2 years age60). In correlation with the plateau in the incidence of IPD, declines in childhood hospitalizations due to pneumonia were also sustained during the decade after 2000 when PCV7 was introduced in the US61).
One study reported the impact of PCV13 on pneumonia. A prospective population-based study was conducted in Southern Israel and assessed hospital use for alveolar pneumonia in young children aged <2 years before and after implementation of PCV13. In this area, PCV7 was introduced into the national immunization program of Israel in 2008 and was replaced by PCV13 in 2010. The monthly incidence, which was 19.5-22.4 per 1,000 population before the introduction of PCV7, decreased to 11.4 per 1,000 population when more than 70% of infants received more than 2 doses of PCV13 (Dagan R, personal communication, Jun 12, 2013).
Afonso et al.62) reported the effectiveness of PCV10 on pneumococcal pneumonia in Brazil. Before the introduction of PCV10 in September 2010, no PCV had been incorporated into the routine immunization system. Hospitalization rates among children 2-24 months of age with all-cause pneumonia were analyzed in 5 Brazilian cities. Within 1 year of PCV10 introduction, significant reductions (23.3%-28.7%) were noted in 3 cities; however, vaccination coverage was lower in the other 2 cities.
Invasive pneumococcal diseases
The overall estimated protection conferred by PCV7 against IPD was evaluated in randomized controlled trials among children aged <2 years before licensure36,38). In a clinical efficacy trial including 37,868 healthy children in California, the efficacy of PCV7 against VT IPD in the fully vaccinated group was 97.4% (95% CI, 82.7% to 99.9%)36). A group randomized trial among subjects from the Navajo and White Mountain Apache Indian reservations was performed in 8,292 children, and the VE was 76.8% (95% CI, -9.4% to 95.1%)38). Two clinical efficacy trials were conducted in Africa: the South African trial53) and the Gambia trial53). A 9-valent investigational PCV was administered as a 3-dose schedule without a booster dose. The VE for VT IPD in these studies was 85% (95% CI, 32% to 98%) in the human immunodeficiency virus (HIV)-negative children and 77% (95% CI, 51% to 90%).
The Cochrane Collaboration performed a systematic review to analyze the VE of PCVs, including PCV7 and the experimental 9- and 11-valent formulations56). From data based on 5 randomized controlled clinical trials including 113,044 children under <2 years of age, the overall VE for VT IPD was 80% (95% CI, 58% to 90%) and 58% (95% CI, 29% to 75%) for all serotypes56). After the introduction of PCV7, the IPD incidence decreased substantially throughout the US. Data from the ABCs showed that the overall incidence of IPD in children <5 years age decreased from 99 cases per 100,000 population (1998-1999) to 21 cases per 100,000 population (2008)9,11). This decrease was attributable to a 99% reduction in IPD due to the PCV7 serotypes and serotype 6A, thus resulting in an overall decrease of 79% for all IPD. The vaccine-related herd immunity resulted in a reduction of IPD in other age groups. This observation was more evident in specific age groups: during 1998-2007, the incidence of IPD due to the PCV7 serotypes in infants aged <2 months showed a 94% (95% CI: 52% to 99%) decrease and a 92% reduction of IPD was observed in subjects aged ≥65 years63).
However, after a dramatic decline following PCV7 introduction, the overall rates of IPD plateaued and remained at 22-25 cases per 100,000 children aged <5 years in the US. This is attributable to increases of NVT serotypes, particularly 19A64,65,66,67). The incidence of IPD due to serotype 19A increased for all ages, and is currently the most common serotype in all US age groups. However, the magnitude of the increase in NVT diseases was small compared to the decrease of VT diseases. According to 2008 ABCs data, 61% of IPD cases in children aged <5 years were due to PCV13 serotypes (serotype 19A for 43% of cases; PCV7 serotypes accounted for <2% of cases). Serotypes 19A, 7F, and 3 accounted for 99% of PCV13-additional serotypes, serotypes 1 and 5 accounted for 0.5%, and serotype 6A caused 0.6% of IPD cases11).
This change in epidemiology in IPD has been reported in other countries as well (Table 2). In Australia, the overall incidence of IPD between 2002 to 2007 decreased by 74.9% in all children <2 years of age after PCV7 introduction in 2005, with an increase in NVT IPD, serotype 19A being the most prevalent66,67). In Calgary area, Canada, the incidence of IPD has been stable among young children aged 0-23 months since 2004, with a 94% decrease in IPD due to PCV7 serotypes and 79% decrease in overall cases of IPD in 2007 after PCV7 introduction in 2002, compared with the 1998-2001 period. The incidence of IPD due to NVT serotypes in children (aged <16 years) increased by 109% in the same period68).
Table 2.
Studies demonstrating effectiveness of pneumococcal protein conjugate vaccines in invasive pneumococcal diseases in children
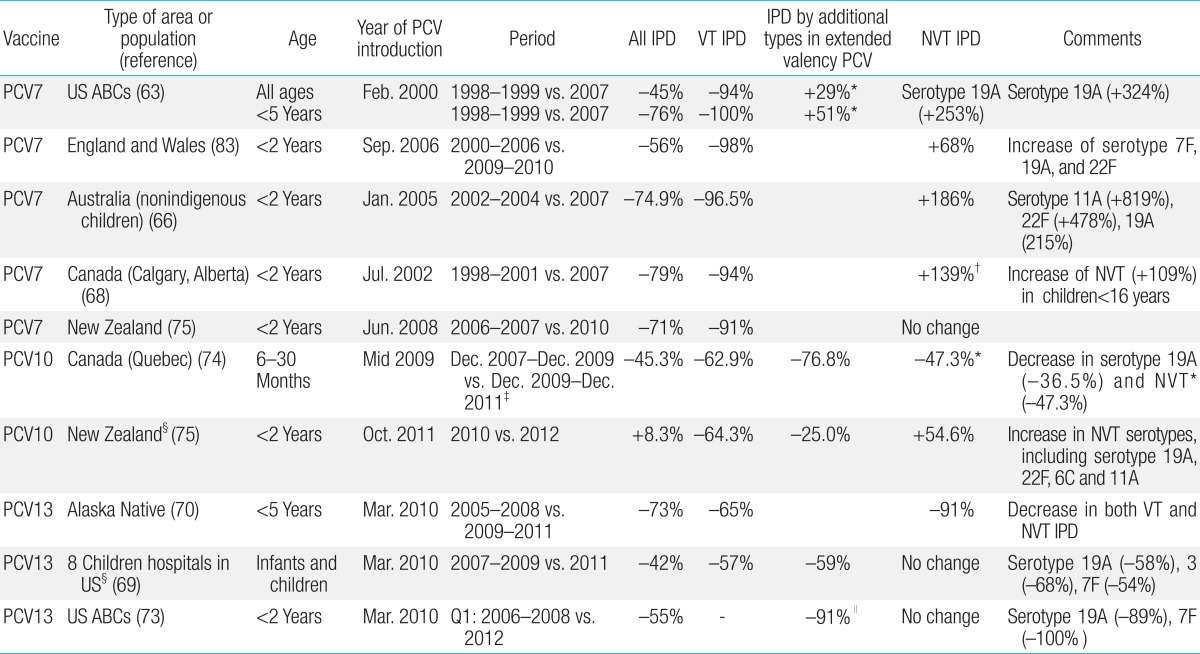
PCV, pneumococcal protein conjugate vaccine; IPD, invasive pneumococcal disease; VT, vaccine type; NVT, nonvaccine type; ABCs, Active Bacterial Core surveillance (ABCs) network; Q, Quarter.
*Except serotype 19A. †P>0.05. ‡Comparison between cohorts of PCV7- vs. PCV10-vaccinated subjects (3+1 schedule). §Based on number of cases. ∥Serotypes 1, 3, 5, 7F, and 19A.
After the introduction of PCV13, a decrease of IPD due to additional serotypes in the PCV13 has been demonstrated in several studies. The US Pediatric Multicenter Pneumococcal Surveillance Groups included 8 children hospitals that prospectively collected IPD cases since September 1993 (Fig. 1)69). Compared with the mean number of cases for 2007-2009, IPD cases decreased by 42% overall and 53% for children aged <24 months in 2011. PCV13 serotype isolates decreased by 57% during these same time periods: 19A, 7F, and 3 decreased by 58%, 54%, and 68%, respectively. The number of infections caused by serotypes 1 and 6C also decreased in 2011. The most common non-PCV13 serotypes in 2010 and 2011 were 33F, 22F, 12, 15B, 15C, 23A, and 11. Among 124 IPD cases in 2011, 12 with PCV13 vaccination were from serotype 19A.
Fig. 1.

Changes in invasive pneumococcal disease incidence among 8 children's hospitals in the United States after the introduction of the 13-valent pneumococcal protein conjugate vaccine (PCV13). PCV7, 7-valent pneumococcal protein conjugate vaccine; PCV10, 10-valent pneumococcal protein conjugate vaccine. Adapted from Kaplan SL, et al. Pediatr Infect Dis J 2013;32:203-769).
The incidence of IPD among Alaskan Native children is of interest, as IPD rates in this population are 10-fold higher than that in non-Alaskan Native children. After introduction of PCV7, among children aged <5 years in the Yukon Kuskokwim Delta (YKD) region, overall IPD incidence decreased by 73% with a 98% decline of PCV7 serotype disease during 2001-2004. However, IPD incidence in YKD children increased during 2005-2007 owing to an increase in non-PCV7 serotypes, predominantly 7F and 19A, which caused 31% and 24% of IPD cases in children <5 years age. PCV13 was first introduced in this area as a part of a phase III clinical trial in 2009. PCV13 was soon licensed in March 2010, and nearly 90% of YKD children <5 years age received at least 1 dose of PCV13 within 12 months of licensure. After introduction of PCV13 with catch-up vaccination in subjects aged <5 years, the overall IPD incidence showed a 73% decrease, PCV13 type IPD decreased by 65%, and a 91% decrease of non-PCV13 IPD was observed by August 201170). This study was performed in a small population and considering the concurrent decrease in non-PCV13 serotypes, further observation of the changes after the introduction of the vaccine is warranted.
The effect of PCV13 is also well described in the weekly surveillance data of England and Wales71). Within 1 year of vaccination in 2011, the effect of PCV13 was shown at the population level, and IPD cases due to additional serotypes in PCV13 (+serotype 6C) in children <2 years of age decreased by 50%. For children aged <13 months, vaccine effectiveness for 1 priming dose was 38% (95% CI, -218% to 89%) and effectiveness for 2 priming doses was 78% (95% CI, -18% to 96%). Effectiveness for a single dose in the second year of life was 73% (95% CI, 29% to 90%) and 77% (95% CI, 38% to 91%) when those who had also received ≥1 PCV13 dose in the first year were included. In this analysis, 6C was included in the vaccine serotype on the basis of evidence of cross-protection from 6A. Vaccine effectiveness was 70% for serotype 19A (95% CI, 10% to 90%) and 76% for serotype 7F (95% CI, 21% to 93%) for ≥1 dose. The incidence of IPD in England and Wales decreased continuously through July 2013 and was observed in both vaccinated and nonvaccinated subjects72).
Preliminary data from the ABCs in the US show the early impact of PCV13 on IPD73). When comparing the same first quarter (January-March) of 2006-2008 with 2012, all IPD cases decreased by 55% in children <2 years of age. In the same age group, IPD due to 5 additional PCV13 serotypes, 1, 3, 5, 7F, and 19A (excluding serotype 6A, which may be cross-protected by serotype 6B), decreased by 91%. In the serotype-specific analysis, IPD caused by serotypes 19A and 7F showed statistically significant decreases of 89% and 100%, respectively. A decrease was also observed for all IPD cases in other age groups such as children aged 2-4 years, adults, and the elderly.
In the province of Quebec, Canada, the PCV7 program was launched in December 2004, and a 2+1 dose schedule (2, 4, and 12 months) was recommended for low-risk infants with catch-up for children aged <5 years. PCV10 was introduced in the summer of 2009, and PCV13 replaced PCV10 in January 2011. Transition to a new vaccine was recommended regardless of the number of doses of another vaccine already administered. Through a comparison of birth cohorts, ecologic analysis of the effectiveness of PCV7 versus PCV10 was possible. The incidence of IPD among infants vaccinated with PCV7 with a primary series and booster was 56.3/100,000 in children 6-30 months of age compared to 30.8 in children vaccinated with PCV10 (rate ratio, 0.55; P=0.02)74). The incidence of 19A-related disease was lower in the PCV10 group; however, the incidence of diseases caused by serotypes other than PCV10 (excluding serotype 19A) and 19A was also lower in the PCV10 group. Thus, it is uncertain whether the lower incidence of serotype 19A disease is associated with cross-protection by 19F included in PCV10. There was no difference in the incidence of IPD caused by serotype 19A between the cohort vaccinated with PCV7 as a primary series and booster and the cohort vaccinated with PCV7 as a primary series and PCV10 as a booster dose (17.6 vs. 16.9).
The effectiveness of PCV10 is also described in the Invasive Pneumococcal Disease Reports of New Zealand, where IPD became a notifiable disease in October 2008. PCV7 was introduced in New Zealand in June 2008 and was replaced with PCV10 in the national immunization program in October 2011. Within 2 years of PCV7 introduction, IPD showed a 71% decrease in children <2 years of age with a 91% decrease in IPD due to PCV7 serotypes75). PCV10 showed a further 64.3% decrease in PCV10 serotypes within 1 year of introduction (2010 vs. 2012); however, there was an increase in NVT serotypes, including serotypes 19A, 22F, 6C, and 11A75). In 2013, number of serotype 19A cases decreased to pre-PCV10 period.
Recently, a controlled, cluster-randomized, double-blind field trial was performed in Finnish healthcare centers to evaluate the effectiveness of PCV10 against IPD in 30,527 subjects76). Vaccine effectiveness was compared with a PCV10 3+1, PCV10 2+1, and control 3+1, control 2+1 group. During a 25-month observation period, 26 cultures confirmed IPD; among these, 13 culture-confirmed VT cases of IPD were detected, with 0 in the PCV10 3+1 group, 1 in the PCV10 2+1 group, and 12 in the control groups. Vaccine effectiveness of PCV10 3+1 was 100% (95% CI, 83% to 100%) and that of PCV10 2+1 was 92% (95% CI, 58% to 100%) for VT IPD. Vaccine effectiveness was demonstrated for the most common serotypes, 6B and 14; however, serotype-specific effectiveness was not applicable for serotypes 1, 5, and 7F owing to a low number of cases, and there were was only 2 cases of serotype 19A in the control group (including 1 case that was excluded from the analysis because of assignment error).
Impact of PCV on pneumococcal diseases in Korean children
IPD is not yet included as a nationally notifiable disease in Korea and population-based incidence data on pneumococcal diseases are not available. Thus, it is difficult to determine the impact of PCV in terms of effectiveness and efficacy in Korea. However, there are reports on pneumococcal diseases, which provide insight into changes of pneumococcal diseases after introduction of PCVs in Korea.
1. Nasopharyngeal carriage
Several NP carriage studies have been reported among children in Korea. A study conducted among healthy children aged 18-59 months in 2008 reported NP carriage among fully vaccinated subjects (PCV7 3-dose primary series with a booster)5). PCV7 serotypes accounted for 11.1% of all serotypes and serotype 6C (16.7%) was the most common serotype, followed by serotypes 6A (13.9%) and 19A (11.1%). The same study reported NP carriage in nonvaccinated control subjects, where PCV7 serotypes accounted for 52.4% of all serotypes, and frequent serotypes included serotypes 14 (14.3% of the isolates), 6B and 23F (12.7% each), and 19F (11.1%). Cho et al.4) studied NP isolates obtained from children with respiratory symptoms during 2009-2010 and compared serotype distribution with isolates from 1997-2002, the period before PCV7 introduction in Korea. The proportion of PCV7 serotypes was 61.9% during 1997-2002, whereas during 2009-2010 the proportion of PCV7 serotypes accounted for 23.8 % of the isolates, PCV10 did not show additional coverage, and PCV13 accounted for 55.0%. During the 2009-2010 period, the most common serotypes were 19A (15.9% of isolates), 6A (15.2%), 19F (11.3%), 15C, and 35B (6.0% each). No studies have been reported to date after the introduction of PCV10 and PCV13.
2. Otitis media
A few studies have reported the serotype distribution of pneumococcus associated with OM. One study reported pneumococcal isolates obtained from ear discharge in children with OM between 2001 and 200677). Among 54 pneumococcal isolates, the predominant serotypes were 19A (44%), 19F (28%), 6B (7%), 6A (4%), 9V (4%), and 1 (4%). PCV7 serotypes accounted for 43%, and 19A and 19F accounted for 72% of isolates.
3. Invasive pneumococcal diseases
Two retrospective multicenter studies were conducted for causative agents of invasive bacterial infections in children at 2 different study periods. The first study was performed during 1996-2005 among subjects aged <15 years involving 18 university hospitals78). IPD accounted for 23.4% (179/766) of all invasive bacterial infections, and in children aged 3 months to <5 years, 45.3% (140/309) were due to pneumococcus. In the following study, which collected data from subjects <18 years of age during 2006-2010 involving 25 university or general hospitals, IPD accounted for 23.2% of invasive bacterial infections in Korean children and 54% in children aged 3 months to <5 years79).
A hospital-wide surveillance study conducted from 1991 to 2006 included 158 invasive pneumococcal isolates. During 2001-2003, just before PCV7 was introduced in Korea, PCV7 serotypes accounted for 54% of all IPD isolates. The proportion of serotype 19A isolates increased from 0% (0/40) during 1991-1994 to 18% (7/39) during 2001-2003, suggesting that serotype 19A began to increase before the introduction of PCV7 in Korea. This increase was associated with the emergence of a highly resistant clone, ST320, related with pressure of antibiotic use7). During this period, the most prevalent serotypes were 23F, 14, 19F, 6B, and 19A. PCV7 serotypes accounted for 60.7%, PCV10 serotypes for 62.7%, and PCV13 serotypes for 81.0% of IPD cases.
A retrospective multicenter study including 8 university hospitals during 2006-2010 reported 140 cases of IPD in children <18 years of age (Fig. 2)80). PCV7 serotypes decreased from 62.5% in 2006 to 21.4% in 2010, and 3 PCV13-specific types (3, 6A, and 19A) increased from 18.8% in 2006 to 42.9% in 2010. The proportion of the 3 additional serotypes in PCV10 was relatively small (0%-7.1%). During this period, PCV vaccination rates for a 3-dose primary series increased from 40% (2005) to 73.8% (2010)81).
Fig. 2.

Distribution of serotypes among 140 invasive pneumococcal isolates in children in Korea by year, 2006-2010. In the trend analysis, PCV7 serotypes significantly decreased over time (from 62.5% to 21.4%, P=0.002), whereas 3 PCV13-specific serotypes increased (from 18.8% to 42.9%, P=0.016). PCV7, 7-valent pneumococcal protein conjugate vaccine; PCV10, 10-valent pneumococcal protein conjugate vaccine; PCV13, 13-valent pneumococcal protein conjugate vaccine. Adapted from Cho EY, et al. Diagn Microbiol Infect Dis Forthcoming 201480).
After the introduction of PCV10 and PCV13 in Korea, a prospective multicenter study including 75 IPD cases in children aged <18 years during 2011-2013 showed that PCV7 serotypes accounted for 9.3% of the IPD cases, no cases were found for the additional PCV10 serotypes, and PCV13 showed coverage for 53.3% of cases82). Serotype 19A was the most common serotype responsible for 32.0% of all isolates and serotype 6A accounted for 5.3%. Other common serotypes were 10A, 15A, 15B, 15C, 23A, and 11A.
Conclusions
After the introduction of PCV, major changes have occurred in the epidemiology of pneumococcal diseases. PCV7 has been shown to be highly efficacious against VT IPD and effective against pneumonia and in reducing OM episodes and related medical care visits in vaccinated subjects11). PCV7 not only showed decreases in disease in vaccinated subjects but also an indirect herd effect in unvaccinated subjects. On the other hand, pneumococcal vaccines induce serotype-specific immunity, and after the widespread use of PCV7, a relative increase in nonvaccine serotypes has been reported, leading to a need for extended serotype coverage for protection. PCV10 and PCV13 have been licensed on the basis of noninferiority of immunogenicity compared to a licensed conjugate vaccine. Following the introduction of PCV10 and PCV13 in 2009 and 2010, within a short period of time, evidence of protection of these vaccines against invasive and mucosal infections caused by pneumococcal serotypes included in the vaccines is accumulating. Vaccine selection should be based on the experience of changes in the dynamics of pneumococcal serotypes and diseases. Continuous surveillance is essential for the appropriate use of pneumococcal vaccines and evaluation of the impact of PCVs on pneumococcal diseases.
Footnotes
Lee H has received research grants from Boryung Biopharma, GlaxoSmithKline Korea Ltd., Green Cross Company, Novartis Korea Ltd., Pfizer Inc., and Sanofi-Pasteur. Choi EH has received research grants from Abbott, GlaxoSmithKline Korea Ltd., and Pfizer Inc.
References
- 1.Henrichsen J. Six newly recognized types of Streptococcus pneumoniae. J Clin Microbiol. 1995;33:2759–2762. doi: 10.1128/jcm.33.10.2759-2762.1995. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Advisory Committee on Immunization Practices. Preventing pneumococcal disease among infants and young children. Recommendations of the Advisory Committee on Immunization Practices (ACIP) MMWR Recomm Rep. 2000;49(RR-9):1–35. [PubMed] [Google Scholar]
- 3.Johnson HL, Deloria-Knoll M, Levine OS, Stoszek SK, Freimanis Hance L, Reithinger R, et al. Systematic evaluation of serotypes causing invasive pneumococcal disease among children under five: the pneumococcal global serotype project. PLoS Med. 2010;7(10):e1000348. doi: 10.1371/journal.pmed.1000348. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Cho EY, Kang HM, Lee J, Kang JH, Choi EH, Lee HJ. Changes in serotype distribution and antibiotic resistance of nasopharyngeal isolates of Streptococcus pneumoniae from children in Korea, after optional use of the 7-valent conjugate vaccine. J Korean Med Sci. 2012;27:716–722. doi: 10.3346/jkms.2012.27.7.716. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Kim KH, Hong JY, Lee H, Kwak GY, Nam CH, Lee SY, et al. Nasopharyngeal pneumococcal carriage of children attending day care centers in Korea: comparison between children immunized with 7-valent pneumococcal conjugate vaccine and non-immunized. J Korean Med Sci. 2011;26:184–190. doi: 10.3346/jkms.2011.26.2.184. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Ahn JG, Choi SY, Kim DS, Kim KH. Enhanced detection and serotyping of Streptococcus pneumoniae using multiplex polymerase chain reaction. Korean J Pediatr. 2012;55:424–429. doi: 10.3345/kjp.2012.55.11.424. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Choi EH, Kim SH, Eun BW, Kim SJ, Kim NH, Lee J, et al. Streptococcus pneumoniae serotype 19A in children, South Korea. Emerg Infect Dis. 2008;14:275–281. doi: 10.3201/eid1402.070807. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.WHO Publication. Pneumococcal vaccines WHO position paper - 2012 - recommendations. Vaccine. 2012;30:4717–4718. doi: 10.1016/j.vaccine.2012.04.093. [DOI] [PubMed] [Google Scholar]
- 9.Centers for Disease Control and Prevention (CDC) Invasive pneumococcal disease in children 5 years after conjugate vaccine introduction--eight states, 1998-2005. MMWR Morb Mortal Wkly Rep. 2008;57:144–148. [PubMed] [Google Scholar]
- 10.Centers for Disease Control and Prevention (CDC) Invasive pneumococcal disease in young children before licensure of 13-valent pneumococcal conjugate vaccine - United States, 2007. MMWR Morb Mortal Wkly Rep. 2010;59:253–257. [PubMed] [Google Scholar]
- 11.Centers for Disease Control and Prevention (CDC) Licensure of a 13-valent pneumococcal conjugate vaccine (PCV13) and recommendations for use among children - Advisory Committee on Immunization Practices (ACIP), 2010. MMWR Morb Mortal Wkly Rep. 2010;59:258–261. [PubMed] [Google Scholar]
- 12.Vaccines, Blood & Biologics. Prevnar 13 (pneumococcal 13-valent conjugate vaccine) [Internet] Silver Spring (MD): U.S. Food and Drug Administration; c2014. [cited 2013 Aug 5]. Available from: http://www.fda.gov/BiologicsBloodVaccines/Vaccines/ApprovedProducts/ucm201667.htm. [Google Scholar]
- 13.U.S. Food and Drug Administration. Prevnar 13: clinical review of new product license application. Silver Spring (MD): U.S. Food and Drug Administration; 2010. [Google Scholar]
- 14.Synflorix, pneumococcal polysaccharide conjugate vaccine (adsorbed): summary of product characteristics [Internet] London: European Medicines Agency; c1995-2014. [cited 2013 Aug 5]. Available from: http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/000973/WC500054346.pdf. [Google Scholar]
- 15.Expert Committee on Biological Standardization, Geneva, 19 to 23 October 2009. Recommendations to assure the quality, safety and efficacy of pneumococcal conjugate vaccines. Replacement of: TRS 927, Annex 2 [Internet] Geneva: World Health Organization; c2009. [cited 2013 Aug 5]. Available from: http://www.who.int/biologicals/areas/vaccines/pneumo/Pneumo_final_23APRIL_2010.pdf?ua=1. [Google Scholar]
- 16.Simell B, Auranen K, Kayhty H, Goldblatt D, Dagan R, O'Brien KL, et al. The fundamental link between pneumococcal carriage and disease. Expert Rev Vaccines. 2012;11:841–855. doi: 10.1586/erv.12.53. [DOI] [PubMed] [Google Scholar]
- 17.O'Brien KL, Millar EV, Zell ER, Bronsdon M, Weatherholtz R, Reid R, et al. Effect of pneumococcal conjugate vaccine on nasopharyngeal colonization among immunized and unimmunized children in a community-randomized trial. J Infect Dis. 2007;196:1211–1220. doi: 10.1086/521833. [DOI] [PubMed] [Google Scholar]
- 18.Parra EL, De La Hoz F, Díaz PL, Sanabria O, Realpe ME, Moreno J. Changes in Streptococcus pneumoniae serotype distribution in invasive disease and nasopharyngeal carriage after the heptavalent pneumococcal conjugate vaccine introduction in Bogota, Colombia. Vaccine. 2013;31:4033–4038. doi: 10.1016/j.vaccine.2013.04.074. [DOI] [PubMed] [Google Scholar]
- 19.Neves FP, Pinto TC, Correa MA, dos Anjos Barreto R, de Souza Gouveia Moreira L, Rodrigues HG, et al. Nasopharyngeal carriage, serotype distribution and antimicrobial resistance of Streptococcus pneumoniae among children from Brazil before the introduction of the 10-valent conjugate vaccine. BMC Infect Dis. 2013;13:318. doi: 10.1186/1471-2334-13-318. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Davis SM, Deloria-Knoll M, Kassa HT, O'Brien KL. Impact of pneumococcal conjugate vaccines on nasopharyngeal carriage and invasive disease among unvaccinated people: Review of evidence on indirect effects. Vaccine. 2013 Dec 17; doi: 10.1016/j.vaccine.2013.05.005. [Epub]. http://dx.doi.org/10.1016/j.vaccine.2013.05.005. [DOI] [PubMed] [Google Scholar]
- 21.Flasche S, Van Hoek AJ, Sheasby E, Waight P, Andrews N, Sheppard C, et al. Effect of pneumococcal conjugate vaccination on serotype-specific carriage and invasive disease in England: a cross-sectional study. PLoS Med. 2011;8:e1001017. doi: 10.1371/journal.pmed.1001017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Ghaffar F, Barton T, Lozano J, Muniz LS, Hicks P, Gan V, et al. Effect of the 7-valent pneumococcal conjugate vaccine on nasopharyngeal colonization by Streptococcus pneumoniae in the first 2 years of life. Clin Infect Dis. 2004;39:930–938. doi: 10.1086/423379. [DOI] [PubMed] [Google Scholar]
- 23.Moore MR, Hyde TB, Hennessy TW, Parks DJ, Reasonover AL, Harker-Jones M, et al. Impact of a conjugate vaccine on community-wide carriage of nonsusceptible Streptococcus pneumoniae in Alaska. J Infect Dis. 2004;190:2031–2038. doi: 10.1086/425422. [DOI] [PubMed] [Google Scholar]
- 24.Sharma D, Baughman W, Holst A, Thomas S, Jackson D, da Gloria Carvalho M, et al. Pneumococcal carriage and invasive disease in children before introduction of the 13-valent conjugate vaccine: comparison with the era before 7-valent conjugate vaccine. Pediatr Infect Dis J. 2013;32:e45–e53. doi: 10.1097/INF.0b013e3182788fdd. [DOI] [PubMed] [Google Scholar]
- 25.Cohen R, Levy C, Bingen E, Koskas M, Nave I, Varon E. Impact of 13-valent pneumococcal conjugate vaccine on pneumococcal nasopharyngeal carriage in children with acute otitis media. Pediatr Infect Dis J. 2012;31:297–301. doi: 10.1097/INF.0b013e318247ef84. [DOI] [PubMed] [Google Scholar]
- 26.Desai AP, Sharma D, Crispell E, Baughman W, Thomas S, Holst A. Pneumococcal nasopharyngeal carriage in children in Atlanta, Georgia in the post-PCV13 era; IDWeek 2012 Advancing Science, Improving Care; 2012 Oct 17-21; San Diego (CA), USA. [Google Scholar]
- 27.Dagan R, Patterson S, Juergens C, Greenberg D, Givon-Lavi N, Porat N, et al. Comparative immunogenicity and efficacy of 13-valent and 7-valent pneumococcal conjugate vaccines in reducing nasopharyngeal colonization: a randomized double-blind trial. Clin Infect Dis. 2013;57:952–962. doi: 10.1093/cid/cit428. [DOI] [PubMed] [Google Scholar]
- 28.Spijkerman J, Prevaes SM, van Gils EJ, Veenhoven RH, Bruin JP, Bogaert D, et al. Long-term effects of pneumococcal conjugate vaccine on nasopharyngeal carriage of S. pneumoniae, S. aureus, H. influenzae and M. catarrhalis. PLoS One. 2012;7:e39730. doi: 10.1371/journal.pone.0039730. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Prymula R, Hanovcova I, Splino M, Kriz P, Motlova J, Lebedova V, et al. Impact of the 10-valent pneumococcal non-typeable Haemophilus influenzae Protein D conjugate vaccine (PHiD-CV) on bacterial nasopharyngeal carriage. Vaccine. 2011;29:1959–1967. doi: 10.1016/j.vaccine.2010.12.086. [DOI] [PubMed] [Google Scholar]
- 30.van den Bergh MR, Spijkerman J, Swinnen KM, Francois NA, Pascal TG, Borys D, et al. Effects of the 10-valent pneumococcal nontypeable Haemophilus influenzae protein D-conjugate vaccine on nasopharyngeal bacterial colonization in young children: a randomized controlled trial. Clin Infect Dis. 2013;56:e30–e39. doi: 10.1093/cid/cis922. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Eskola J, Kilpi T, Palmu A, Jokinen J, Haapakoski J, Herva E, et al. Efficacy of a pneumococcal conjugate vaccine against acute otitis media. N Engl J Med. 2001;344:403–409. doi: 10.1056/NEJM200102083440602. [DOI] [PubMed] [Google Scholar]
- 32.Block SL, Hedrick J, Harrison CJ, Tyler R, Smith A, Findlay R, et al. Community-wide vaccination with the heptavalent pneumococcal conjugate significantly alters the microbiology of acute otitis media. Pediatr Infect Dis J. 2004;23:829–833. doi: 10.1097/01.inf.0000136868.91756.80. [DOI] [PubMed] [Google Scholar]
- 33.Bluestone CD, Stephenson JS, Martin LM. Ten-year review of otitis media pathogens. Pediatr Infect Dis J. 1992;11(8 Suppl):S7–S11. doi: 10.1097/00006454-199208001-00002. [DOI] [PubMed] [Google Scholar]
- 34.Fletcher MA, Fritzell B. Pneumococcal conjugate vaccines and otitis media: an appraisal of the clinical trials. Int J Otolaryngol. 2012;2012:312935. doi: 10.1155/2012/312935. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Fireman B, Black SB, Shinefield HR, Lee J, Lewis E, Ray P. Impact of the pneumococcal conjugate vaccine on otitis media. Pediatr Infect Dis J. 2003;22:10–16. doi: 10.1097/00006454-200301000-00006. [DOI] [PubMed] [Google Scholar]
- 36.Black S, Shinefield H, Fireman B, Lewis E, Ray P, Hansen JR, et al. Northern California Kaiser Permanente Vaccine Study Center Group. Efficacy, safety and immunogenicity of heptavalent pneumococcal conjugate vaccine in children. Pediatr Infect Dis J. 2000;19:187–195. doi: 10.1097/00006454-200003000-00003. [DOI] [PubMed] [Google Scholar]
- 37.Kilpi T, Ahman H, Jokinen J, Lankinen KS, Palmu A, Savolainen H, et al. Protective efficacy of a second pneumococcal conjugate vaccine against pneumococcal acute otitis media in infants and children: randomized, controlled trial of a 7-valent pneumococcal polysaccharide-meningococcal outer membrane protein complex conjugate vaccine in 1666 children. Clin Infect Dis. 2003;37:1155–1164. doi: 10.1086/378744. [DOI] [PubMed] [Google Scholar]
- 38.O'Brien KL, Moulton LH, Reid R, Weatherholtz R, Oski J, Brown L, et al. Efficacy and safety of seven-valent conjugate pneumococcal vaccine in American Indian children: group randomised trial. Lancet. 2003;362:355–361. doi: 10.1016/S0140-6736(03)14022-6. [DOI] [PubMed] [Google Scholar]
- 39.Prymula R, Peeters P, Chrobok V, Kriz P, Novakova E, Kaliskova E, et al. Pneumococcal capsular polysaccharides conjugated to protein D for prevention of acute otitis media caused by both Streptococcus pneumoniae and non-typable Haemophilus influenzae: a randomised double-blind efficacy study. Lancet. 2006;367:740–748. doi: 10.1016/S0140-6736(06)68304-9. [DOI] [PubMed] [Google Scholar]
- 40.Sarasoja I, Jokinen J, Lahdenkari M, Kilpi T, Palmu AA. Long-term effect of pneumococcal conjugate vaccines on tympanostomy tube placements. Pediatr Infect Dis J. 2013;32:517–520. doi: 10.1097/INF.0b013e31827c9bcc. [DOI] [PubMed] [Google Scholar]
- 41.De Wals P, Erickson L, Poirier B, Pepin J, Pichichero ME. How to compare the efficacy of conjugate vaccines to prevent acute otitis media? Vaccine. 2009;27:2877–2883. doi: 10.1016/j.vaccine.2009.02.102. [DOI] [PubMed] [Google Scholar]
- 42.Grijalva CG, Poehling KA, Nuorti JP, Zhu Y, Martin SW, Edwards KM, et al. National impact of universal childhood immunization with pneumococcal conjugate vaccine on outpatient medical care visits in the United States. Pediatrics. 2006;118:865–873. doi: 10.1542/peds.2006-0492. [DOI] [PubMed] [Google Scholar]
- 43.Jardine A, Menzies RI, Deeks SL, Patel MS, McIntyre PB. The impact of pneumococcal conjugate vaccine on rates of myringotomy with ventilation tube insertion in Australia. Pediatr Infect Dis J. 2009;28:761–765. doi: 10.1097/INF.0b013e31819e9bc5. [DOI] [PubMed] [Google Scholar]
- 44.Taylor S, Marchisio P, Vergison A, Harriague J, Hausdorff WP, Haggard M. Impact of pneumococcal conjugate vaccination on otitis media: a systematic review. Clin Infect Dis. 2012;54:1765–1773. doi: 10.1093/cid/cis292. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Alonso M, Marimon JM, Ercibengoa M, Perez-Yarza EG, Perez-Trallero E. Dynamics of Streptococcus pneumoniae serotypes causing acute otitis media isolated from children with spontaneous middle-ear drainage over a 12-year period (1999-2010) in a region of northern Spain. PLoS One. 2013;8:e54333. doi: 10.1371/journal.pone.0054333. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Sáez-Llorens X, Castrejon MM, Rowley S, Wong D, Calvo A, Rodriguez M, Troitino M, et al. Efficacy of 10-valent pneumococcal non-typable Haemophilus influenzaeprotein D conjugate vaccine (PHID-CV) against acute otitis media in children in Panama; The 9th International Symposium on Antimicrobial Agents and Resistance; 2013 Mar 13-15; Kuala Lumpur, Malaysia. [Google Scholar]
- 47.Dagan R, Givon-Lavi N, Leibovitz E, Greenberg D. Incidence dynamics of culture-proven otitis media 4 years before and 3 years after introduction of pneumococcal conjugate vaccines (PCVs) in Southern Israel; IDWeek 2012 Advancing Science, Improving Care; 2012 Oct 17-21; San Diego (CA), USA. [Google Scholar]
- 48.Dagan R, Greenberg D, Leibovitz E, Raiz S, Ben-Shimol S, Givon-Lavi N. Trends in serotype-specific pneumococcal carriage in children visiting pediatric emergency room (PER) post PCV7 and PCV13 introduction correlate with trends in serotype-specific otitis media (OM) incidence; IDWeek 2013 Advancing Science, Improving Care; 2013 Oct 2-6; San Fransisco (CA), USA. [Google Scholar]
- 49.Cherian T, Mulholland EK, Carlin JB, Ostensen H, Amin R, de Campo M, et al. Standardized interpretation of paediatric chest radiographs for the diagnosis of pneumonia in epidemiological studies. Bull World Health Organ. 2005;83:353–359. [PMC free article] [PubMed] [Google Scholar]
- 50.Black SB, Shinefield HR, Ling S, Hansen J, Fireman B, Spring D, et al. Effectiveness of heptavalent pneumococcal conjugate vaccine in children younger than five years of age for prevention of pneumonia. Pediatr Infect Dis J. 2002;21:810–815. doi: 10.1097/00006454-200209000-00005. [DOI] [PubMed] [Google Scholar]
- 51.Hansen J, Black S, Shinefield H, Cherian T, Benson J, Fireman B, et al. Effectiveness of heptavalent pneumococcal conjugate vaccine in children younger than 5 years of age for prevention of pneumonia: updated analysis using World Health Organization standardized interpretation of chest radiographs. Pediatr Infect Dis J. 2006;25:779–781. doi: 10.1097/01.inf.0000232706.35674.2f. [DOI] [PubMed] [Google Scholar]
- 52.Cutts FT, Zaman SM, Enwere G, Jaffar S, Levine OS, Okoko JB, et al. Efficacy of nine-valent pneumococcal conjugate vaccine against pneumonia and invasive pneumococcal disease in The Gambia: randomised, double-blind, placebo-controlled trial. Lancet. 2005;365:1139–1146. doi: 10.1016/S0140-6736(05)71876-6. [DOI] [PubMed] [Google Scholar]
- 53.Klugman KP, Madhi SA, Huebner RE, Kohberger R, Mbelle N, Pierce N, et al. A trial of a 9-valent pneumococcal conjugate vaccine in children with and those without HIV infection. N Engl J Med. 2003;349:1341–1348. doi: 10.1056/NEJMoa035060. [DOI] [PubMed] [Google Scholar]
- 54.Madhi SA, Kuwanda L, Cutland C, Klugman KP. The impact of a 9-valent pneumococcal conjugate vaccine on the public health burden of pneumonia in HIV-infected and -uninfected children. Clin Infect Dis. 2005;40:1511–1518. doi: 10.1086/429828. [DOI] [PubMed] [Google Scholar]
- 55.Lucero MG, Nohynek H, Williams G, Tallo V, Simoes EA, Lupisan S, et al. Efficacy of an 11-valent pneumococcal conjugate vaccine against radiologically confirmed pneumonia among children less than 2 years of age in the Philippines: a randomized, double-blind, placebo-controlled trial. Pediatr Infect Dis J. 2009;28:455–462. doi: 10.1097/INF.0b013e31819637af. [DOI] [PubMed] [Google Scholar]
- 56.Lucero MG, Dulalia VE, Nillos LT, Williams G, Parreno RA, Nohynek H, et al. Pneumococcal conjugate vaccines for preventing vaccine-type invasive pneumococcal disease and X-ray defined pneumonia in children less than two years of age. Cochrane Database Syst Rev. 2009;(4):CD004977. doi: 10.1002/14651858.CD004977.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Hortal M, Sehabiague G, Camou T, Iraola I, Estevan M, Pujadas M. Pneumococcal pneumonia in hospitalized Uruguayan children and potential prevention with different vaccine formulations. J Pediatr. 2008;152:850–853. doi: 10.1016/j.jpeds.2007.11.008. [DOI] [PubMed] [Google Scholar]
- 58.Sánchez Varela M, Chiarella M, Helios M, Facal J, Pirez MC, Algorta G. Impact of children universal pneumococcal vaccination (PCV7V/PCV13V) on hospitalizations for pneumonia and pneumococcal invasive disease in the British hospital, Uruguay; The 8th International Symposium on Pnuemococci and Pneumococcal Diseases; 2012 Mar 11-15; Iguacu Falls, Brazil. [Google Scholar]
- 59.Grijalva CG, Nuorti JP, Arbogast PG, Martin SW, Edwards KM, Griffin MR. Decline in pneumonia admissions after routine childhood immunisation with pneumococcal conjugate vaccine in the USA: a time-series analysis. Lancet. 2007;369:1179–1186. doi: 10.1016/S0140-6736(07)60564-9. [DOI] [PubMed] [Google Scholar]
- 60.Jardine A, Menzies RI, McIntyre PB. Reduction in hospitalizations for pneumonia associated with the introduction of a pneumococcal conjugate vaccination schedule without a booster dose in Australia. Pediatr Infect Dis J. 2010;29:607–612. doi: 10.1097/inf.0b013e3181d7d09c. [DOI] [PubMed] [Google Scholar]
- 61.Griffin MR, Zhu Y, Moore MR, Whitney CG, Grijalva CG. U.S. hospitalizations for pneumonia after a decade of pneumococcal vaccination. N Engl J Med. 2013;369:155–163. doi: 10.1056/NEJMoa1209165. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Afonso ET, Minamisava R, Bierrenbach AL, Escalante JJ, Alencar AP, Domingues CM, et al. Effect of 10-valent pneumococcal vaccine on pneumonia among children, Brazil. Emerg Infect Dis. 2013;19:589–597. doi: 10.3201/eid1904.121198. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Pilishvili T, Lexau C, Farley MM, Hadler J, Harrison LH, Bennett NM, et al. Sustained reductions in invasive pneumococcal disease in the era of conjugate vaccine. J Infect Dis. 2010;201:32–41. doi: 10.1086/648593. [DOI] [PubMed] [Google Scholar]
- 64.Weinberger DM, Malley R, Lipsitch M. Serotype replacement in disease after pneumococcal vaccination. Lancet. 2011;378:1962–1973. doi: 10.1016/S0140-6736(10)62225-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Changing epidemiology of pneumococcal serotypes after introduction of conjugate vaccine: July 2010 report. Wkly Epidemiol Rec. 2010;85:434–436. [PubMed] [Google Scholar]
- 66.Williams SR, Mernagh PJ, Lee MH, Tan JT. Changing epidemiology of invasive pneumococcal disease in Australian children after introduction of a 7-valent pneumococcal conjugate vaccine. Med J Aust. 2011;194:116–120. doi: 10.5694/j.1326-5377.2011.tb04192.x. [DOI] [PubMed] [Google Scholar]
- 67.Lehmann D, Willis J, Moore HC, Giele C, Murphy D, Keil AD, et al. The changing epidemiology of invasive pneumococcal disease in aboriginal and non-aboriginal western Australians from 1997 through 2007 and emergence of nonvaccine serotypes. Clin Infect Dis. 2010;50:1477–1486. doi: 10.1086/652440. [DOI] [PubMed] [Google Scholar]
- 68.Kellner JD, Vanderkooi OG, MacDonald J, Church DL, Tyrrell GJ, Scheifele DW. Changing epidemiology of invasive pneumococcal disease in Canada, 1998-2007: update from the Calgary-area Streptococcus pneumoniae research (CASPER) study. Clin Infect Dis. 2009;49:205–212. doi: 10.1086/599827. [DOI] [PubMed] [Google Scholar]
- 69.Kaplan SL, Barson WJ, Lin PL, Romero JR, Bradley JS, Tan TQ, et al. Early trends for invasive pneumococcal infections in children after the introduction of the 13-valent pneumococcal conjugate vaccine. Pediatr Infect Dis J. 2013;32:203–207. doi: 10.1097/INF.0b013e318275614b. [DOI] [PubMed] [Google Scholar]
- 70.Singleton R, Wenger J, Klejka JA, Bulkow LR, Thompson A, Sarkozy D, et al. The 13-valent pneumococcal conjugate vaccine for invasive pneumococcal disease in Alaska native children: results of a clinical trial. Pediatr Infect Dis J. 2013;32:257–263. doi: 10.1097/INF.0b013e3182748ada. [DOI] [PubMed] [Google Scholar]
- 71.Miller E, Andrews NJ, Waight PA, Slack MP, George RC. Effectiveness of the new serotypes in the 13-valent pneumococcal conjugate vaccine. Vaccine. 2011;29:9127–9131. doi: 10.1016/j.vaccine.2011.09.112. [DOI] [PubMed] [Google Scholar]
- 72.Health Protection Agency. Current epidemiology of invasive pneumococcal disease (IPD) [Internet] London: Immunisation Department, Public Health England; [cited 2013 Aug 23]. Available from: http://www.hpa.org.uk/Topics/InfectiousDiseases/InfectionsAZ/Pneumococcal/EpidemiologicalDataPneumococcal/CurrentEpidemiologyPneumococcal/InPrevenar7/pneumo03Cummulativeweekly5INPrevenar7vacc/ [Google Scholar]
- 73.Moore M, Link-Gelles R, Farley MM, Schaffner W, Thomas A, Reingold A, et al. Impact of 13-valent pneumococcal conjugate vaccine on invasive pneumococcal disease, U.S, 2010-11; ID Week 2012 Advancing Science, Improving Care; 2012 Oct 17-21; San Diego (CA), USA. [Google Scholar]
- 74.De Wals P, Lefebvre B, Markowski F, Deceuninck G, Defay F, Boulianne N. Invasive pneumococcal disease in birth cohorts vaccinated with PCV7 and/or PHiD-CV in Quebec: an update; The 31st Meeting of the European Society for Paediatric Infectious Diseases; 2013 May 28-June 1; Milan, Italy. [Google Scholar]
- 75.Institute of Environmental Science and Research Ltd, New Zealand. Invasive Pneumococcal Disease Reports [Internet] Wellington (NZ): Population and Environmental Health Institute of Environmental Science & Research Limited Kenepuru Science Centre; [cited 2014 Jan 30]. Available from: http://www.surv.esr.cri.nz/surveillance/IPD.php. [Google Scholar]
- 76.Palmu AA, Jokinen J, Borys D, Nieminen H, Ruokokoski E, Siira L, et al. Effectiveness of the ten-valent pneumococcal Haemophilus influenzae protein D conjugate vaccine (PHiD-CV10) against invasive pneumococcal disease: a cluster randomised trial. Lancet. 2013;381:214–222. doi: 10.1016/S0140-6736(12)61854-6. [DOI] [PubMed] [Google Scholar]
- 77.Lee TJ, Chun JK, Kim KH, Kim KJ, Kim DS. Serotype distribution of pneumococcus isolated from the ear discharge in children with otitis media in 2001-2006. Korean J Pediatr Infect Dis. 2008;15:44–50. [Google Scholar]
- 78.Lee JH, Cho HK, Kim KH, Kim CH, Kim DS, Kim KN, et al. Etiology of invasive bacterial infections in immunocompetent children in Korea (1996-2005): a retrospective multicenter study. J Korean Med Sci. 2011;26:174–183. doi: 10.3346/jkms.2011.26.2.174. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79.Cho EY, Kim YJ, Eun BW, Kim YK, Cho DS, Lee HS, et al. Causative pathogens among childhood bacterial invasive infection in Korea; a multicenter study, 2006-2010; The 2012 Annual Meeting of the Korean Society of Pediatric Infectious Diseases; 2012 Nov 10; Seoul, Korea. [Google Scholar]
- 80.Cho EY, Lee H, Choi EH, Kim YJ, Eun BW, Cho YK, et al. Serotype and antibiotic resistance of Streptococcus pneumoniaeisolates from invasive infectionsafter optional use of the 7-valent conjugate vaccinein Korea, 2006-2010. Diagn Microbiol Infect Dis. doi: 10.1016/j.diagmicrobio.2013.12.016. Forthcoming 2014. http://authors.elsevier.com/sd/article/S0732889314000066. [DOI] [PubMed] [Google Scholar]
- 81.Choe YJ, Yang JJ, Park SK, Choi EH, Lee HJ. Comparative estimation of coverage between national immunization program vaccines and non-NIP vaccines in Korea. J Korean Med Sci. 2013;28:1283–1288. doi: 10.3346/jkms.2013.28.9.1283. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Cho EY, Choi EH, Lee H, Kang JH, Kim KH, Lee HJ, et al. Multicentric approach for analysis of serotypes of pneumococcus isolated from invasive infections in Korean children. Korea [abstract]; The 2013 Annual Meeting of the Korean Society of Pediatric Infectious Diseases; 2013 Nov 9; Seoul, Korea. [Google Scholar]
- 83.Miller E, Andrews NJ, Waight PA, Slack MP, George RC. Herd immunity and serotype replacement 4 years after seven-valent pneumococcal conjugate vaccination in England and Wales: an observational cohort study. Lancet Infect Dis. 2011;11:760–768. doi: 10.1016/S1473-3099(11)70090-1. [DOI] [PubMed] [Google Scholar]