

Abstract
Background and Aim:
Iran's health sector has been engaging the services of physicians and midwives in healthcare centers since 2005, with the hope of improving the quantity and quality of family planning services. The aim of this study was to assess the effect of serving physicians and midwives on the quantity and quality of family planning services in the healthcare centers of Iran.
Materials and Methods:
The present cross-sectional study (Jan 2010 until Sep 2011) was carried out on 600 eligible families who were clients of healthcare centers of Tabriz, Azarshahr and Osku, cities of Northwest Iran from 2006 until 2011, in two groups (before and after). Some of the characteristics of the participants and the data on the quality and quantity of family planning services provided were grouped in a checklist of 16 variables by comparing the patients’ past medical histories.
Results:
In comparison with 3 years prior to engaging physician and midwife services in health care centers, the Couple Year Protection (CYP) and the quantity of family planning service indexes significantly increased among eligible families. The family size of participants declined significantly after family physicians and midwives became available in the healthcare centers (P < 0.005).
Conclusion:
Our findings showed some improvement in the quantity of services without any noticeable changes in the quality of services provided as a consequence of this huge intervention. Therefore, it is suggested that there should be proper oversight of the duties of the health team in order to keep a close watch on primary healthcare, design of proper mechanisms for collecting and maintaining performance reports and statistics, and continuously monitor and control the quality of services.
Keywords: Family planning, fertility, health services, healthcare services, reproductive ages, women of reproductive age
INTRODUCTION
Despite the development and availability of family planning services, the level of unmet need for family planning in many countries, continues to increase. This suggests that innovative approaches are needed to extend the access to family planning services for women and couples who want to limit their family size, but are currently not using contraceptive methods.[1,2] Demographic growth in the developing world will continue to increase the pressure on women of reproductive age for several decades. The former United Nations Secretary General, Kofi Annan regarded family planning as an essential means of achieving the Millennium Development Goals. It was also mentioned that as part of the fifth Millennium Development Goal targets, universal access to family planning was a key strategy for the improvement of maternal health.[3] A current, major problem in most developing countries is uncontrolled population growth, a serious threat, in terms of economic, health, and social burden to the international community.[4,5] For a variety of reasons family planning fails the millions of people who use it to avoid pregnancy. Some of these reasons could be the lack of or inadequate advice or instruction on proper use, inability to select a method suited to the couple, lack of information on side effects, or the lack of supplies. Help for these people is urgent, for the task of family planning will become even more arduous when, about 60 million girls and boys reach sexual maturity in the next 5 years. Generation after generation will need family planning and other healthcare.[6] There is a broad consensus among researchers, health educators, and healthcare managers that the provision of good quality family planning services encourages acceptance or continuation of contraceptive use.[7,8] Moreover, high-quality care is thought to affect the reproductive behavior of women who are ambivalent about their intentions or do not use services because of perceptions of poor quality. It also affects those who have discontinued the use of contraception because of poor quality service or discourteous treatment on the part of providers. The bulk of evidence from both developed and developing countries confirm that high-quality care can be expected to help in reducing the rate of discontinuation of the use of contraception and unintended pregnancies.
The identified system and organizational limiting bans of family planning presentations were grouped into five categories: Diversity of tasks and incompatibility with the providers’ own basic training; lack of supervision and management; little time spent on clients’ training; lack of privacy and appropriate materials for education and counseling; and inadequate opportunities for continuing education.[7,9,10]
Nurses play a key role in instructing women who come to family planning clinics looking for a method of contraception. These one-to-one encounters are opportunities for women to be taught effective use of contraceptive methods. However, very little is known about the nature of these consultations.[11] By providing free family planning services, the family planning program has presented good access to low-income couples to services that would otherwise be too expensive for most families in both rural and urban areas.[2,12] High-quality services ensure that clients receive the care they deserve, and several impact studies have shown that by improving the quality of reproductive health services, the use of contraception increases.[13] Iran's health system introduced the services of general practitioners and midwives in healthcare centers in 2005, with the aim of raising the quantity and quality of family planning and other primary health services. This study aimed at assessing the impact of the presence of general practitioners and midwives on the quantity and quality of family planning services in healthcare centers in Iran.
MATERIALS AND METHODS
This cross-sectional study (Jan 2010-Sept 2011) was carried out on families who were covered by the healthcare centers of three cities (Tabriz, Osku, and Azarshahr) in northwest Iran, where, family physicians and midwives had been introduced into the system 3 years before. A number of related indexes of the years from 2004 until 2006 compared with those of 2008 until 2010 (before and after the introduction of family physician and midwives into the system) were used. Inclusion criteria consisted of women of reproductive age, without any history of infertility. To calculate and compare general indexes such as birthrate, family planning coverage (couples using contraception methods), continuing of annual coverage, and all women of reproductive age were selected as research sample (full counting). Data relating to general indexes were gathered from statistical documents of the health centers. Six hundred women under coverage (100 women for each year) were selected in a randomized quota cluster method from the family health profile of health centers as a sample for qualitative analysis and efficiency of services. Data relating to this section were gathered by a checklist of 16 variables extracted from family documents. A questionnaire was prepared with the following 16 variables: Family size, current age of the woman, age at marriage, age at first delivery, number of abortions, the number of stillbirths, number of children alive, type of contraceptive methods (pill, condom, and intrauterine device (IUD), female tubal ligation (TL), and injection) before and after the introduction of a physician and a midwife in the healthcare center, the number of received blisters (oral contraceptive pills (OCPs)) from the healthcare centers, the number of injections in a year, frequency of IUD control by physicians or midwives in a year, modification of the method of contraception, reason for change, pregnancy despite the use of contraceptive methods, periodic genital examinations, and Pap smear. Validity and reliability of the questionnaire were approved by six healthcare specialists and executive managers from Tabriz University of Medical Sciences. All the mentioned variables in the questionnaire were obtained through family health profiles. Data were analyzed using Statistical Package for Social Sciences (SPSS) software version 16 and descriptive statistics including percentage, mean, median, standard deviation (SD) and a statistical comparison analysis including comparison and independent t-test were done. P ≤ 0.05 was considered statistically significant.
Ethical consideration
Permission to undertake the study was obtained from the Ethics Committee of Tabriz University of Medical Sciences and also from the authorities at the local health center and the health posts. For the study, informed consent was obtained from all clients before being observed or interviewed.
RESULTS
Most of characteristics of participants significantly changed prior to and after the engagement of family physicians or midwives in the healthcare centers [Table 1]. The family size of the participants significantly declined after family physicians or midwives were introduced in the healthcare centers (P < 0.005). The age of marriage and the age of first parturition declined, but they were not significant. Couple Year Protection (CYP) significantly increased among eligible families after the family physician or midwife came to the healthcare centers [Table 2]. Comparisons of CYP per year and the use of contraceptive methods during both phases: Before and after the introduction of the family physician and midwife in the healthcare centers are presented in Table 2. The results of each contraceptive method are presented in Table 3. As shown in Table 3, the use of every contraceptive method except injection increased significantly after the introduction of a physician or a midwife in the healthcare centers (P < 0.05).
Table 1.
Participant's characteristics, before and after presence of physician and midwife in healthcare centers

Table 2.
Frequencies of using contraceptive methods after presence of physician and midwife in healthcare centers
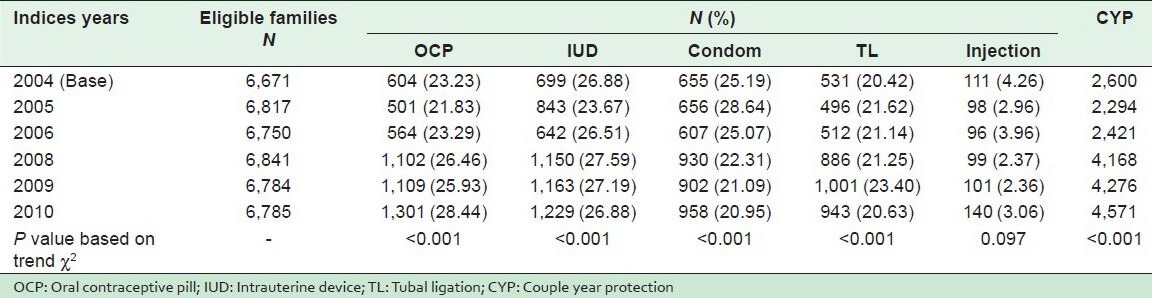
Table 3.
Contraceptive users before and after presence of physician and midwife in healthcare centers

DISCUSSION
The aim of present study was to assess the impact of a serving physician and a midwife in the quantity and quality of family planning services provided in healthcare centers of Iran. Family size and the age of families who were eligible to make use of family planning services has significantly declined in the last 3 years that physicians and midwives have provided family planning services compared with the 3 years previous to the employment of physicians and midwives in the healthcare centers. The findings of the present study reveal the effectiveness of the presence of a physician and a midwife in improving the quantity and quality of family planning services, resulting in an increase in CYP. These findings, which are supported by other studies, indicate a positive impact of quality improvement interventions on the compliance of providers with clinical standards and their performance in service delivery. The mean of CYP was significantly increased with the presence of physicians and midwives in the healthcare centers (P < 0.05). Vahidnia in a study in Iran in 2007, reported that the involvement of midwives was an important measure taken by the government to promote family planning and reproductive health services in the rural areas because it has been very effective in reducing maternal and child mortality, and increased the prevalence rates of contraceptive use.[14] Another study indicated that the prevalence rate of contraception increased from 49.6% in 1989 to 73.8% in 2000 in Iran. This could be related to the increased level of literacy of women, which plays an important role in improving maternal health, since educated women tend to postpone childbearing and increase the gap between children.[15] In conflict with ours and some studies mentioned, a review article revealed that the average program effort levels have remained constant in most countries. This means that there are some flaws, and many countries have not yet achieved the goal of universal access to a variety of contraceptive choices, both in the short- and long-term.[16]
The quantity of family planning services including the mean of OCP users was significantly increased among the participants after the provision of a serving physician and midwife in comparison with the 3 previous years in selected healthcare centers (P < 0.05). The increasing number of OCP users is in agreement with the Ehsanpour et al., research. Findings of the study which was carried out among 378 women revealed the highest frequency of the attitude scores toward the low-dose estrogen (LD) pills method (60.8%) which was associated with unfavorable attitude of the women in the responses of the participants. It is possible that the fear expressed was the result of the side effects of the pills due to their hormonal combination effect, although a large number of the participants believed that the pill was an effective contraceptive method.[17] Furthermore, research worldwide recommends that when properly administered, the pill would be preferable in spite of its potential risks. Using the pill would be safer than pregnancy and labor though women never think of pregnancy as carrying a lot of risks. In addition, the doses of estrogen and progesterone contained in the pill are now low, therefore an experienced physician and/or a midwife would be the perfect choice to provide family planning services and inform clients about all contraceptive methods, including their benefits and disadvantages. This would increase the quality of family planning services and reduce unintended pregnancies and their effect on women and their families.
The number of other contraceptive users including IUD and TL has increased after physicians and midwives came to serve in the healthcare centers though not significantly. In total, contraceptive prevalence rate (CPR) increased among eligible families after family planning services in the healthcare centers were augmented with physicians and midwives. In a research in this field in 2011, Mekonnen and Worku reported that the 25.4% (95% CI: 24.2, 26.5) CPR among married women in Butajira district in 2009 is comparable to the regional and national CPR of 25.8 and 28.6, respectively in 2011 and similar to the present study. They also confirmed that the increase in acceptability of contraception in recent years could be attributed to the improvement and expanding health services.[18] In this study, issues that are still debatable are the low percentages of the use of condoms, injective contraception (depot medroxy-progestrone acetate), and TL users before and after employing physicians and midwives in the healthcare centers. Similar results were reported in a study on factors affecting the quality of care in family planning clinics in Iran, which revealed serious flaws in the provision of family planning care in healthcare facilities, resulting mostly from inadequacies in counseling and dissemination of information. That study recommended training or retraining providers in the following key aspects of family planning:
Education of healthcare professionals (especially college-educated nurses and midwives) in the more practical aspects of primary healthcare delivery
Training of physicians as ‘supervisors’ of service delivery on the preparation of mechanisms and strategies for effective supervision
Emphasis on other means of disseminating information, such as booklets and audiovisual material. As other countries have experienced, this may have a great impact on improving clients’ knowledge, promoting contraceptive use, and dispelling fears and misconceptions.[19,20]
The changes in Iran (declining of population growth) confirm that commitment to policy and financial support, easy availability of family planning services, and high demand can ensure a swift increase in the use of contraceptive methods and a decline in fertility. To improve the quality of care for clients, there must be an awareness of their cultural values, previous experiences, and their perceptions of the role of the health system. In addition, the reproductive health service providers and the community should come together to map out a shared vision of quality. Creating a vision on improving the quality of care requires that program managers, service providers, researchers, and consumer advocates perceive that improved health services is necessary for improving the quality of life. Health specialists continue to formulate the definition and measurement of quality of care, even as women's groups and nongovernmental organizations encourage clients and communities to ask for good quality healthcare services. Every effort should be made to motivate providers, improve their performance, and support them in their role of improving of access to quality family planning and reproductive healthcare services.
With time and determination, it is hoped that, the current effort to improve the quality of care will have a positive influence on services so that standards are raised to a degree that is high enough to satisfy the needs of both clients and providers around the world. As Ross and Smith recommended,[16] international and regional agencies have outstanding roles to play by monitoring mechanisms such as effort indicators, which can help to sallocate resources, understand program deficiencies and identify cost-effective means to strengthen programs.
CONCLUSION
In essence, these findings show some changes in the quantity of services and lack of sensible changes in the quality of services provided as a consequence of this huge intervention. These results were in accord with those of a few studies conducted on family physicians in Iran; the success achieved is moderate in spite of expectations from the notable presence of physicians and midwives in family physician teams. It is, therefore, suggested the duties of the health team be properly supervised in order to fend off an attitude of delivering services that are purely therapeutic and pay greater attention to primary care, design proper mechanisms for collecting and maintaining performance reports and statistics, monitor and control quality of services, with computerization of family documents. Similar studies should also be conducted periodically through interviews to determine the quality of services.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Kuhlmann AS, Gavin L, Galavotti C. The integration of family planning with other health services: A literature review. Int Perspect Sex Peprod Health. 2010;36:189–96. doi: 10.1363/3618910. [DOI] [PubMed] [Google Scholar]
- 2.Khayyati F, Motlagh ME, Kabir M, Kazemeini H, Gharibi F, Jafari N. The role of family physician in case finding, referral, and insurance coverage in the rural areas. Iran J Public Health. 2011;40:136–9. [PMC free article] [PubMed] [Google Scholar]
- 3.Tsui AO, McDonald-Mosley R, Burke AE. Family planning and the burden of unintended pregnancies. Epidemiol Rev. 2010;32:152–74. doi: 10.1093/epirev/mxq012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Fathizadeh N, Bafghi RK, Boroumandfar K, Savabi M. Comparing the effects of Yasmin ® and LD™(low-dose estrogen) as contraceptive methods on menstrual cycle changes in women referred to the health care centers of Isfahan. Iran J Nurs Midwifery Res. 2010;15:252–8. [PMC free article] [PubMed] [Google Scholar]
- 5.Moin M, Rezaei N, Yeganeh M. UNESCO Chair in Health Education: A step toward public health improvement. Iran J Public Health. 2006;35:1–6. [Google Scholar]
- 6.Johns Hopkins Bloomberg School of Public Health/Center for Communication Programs and World Health Organization. 2011 Update; [Cited on 2 February 2013]. Family Planning: A Global Handbook for Providers. Available from: http://whqlibdoc.who.int/publications/2011/9780978856373_eng.pdf?ua=1 . [Google Scholar]
- 7.Mohammad-Alizadeh C, Wahlström R, Vahidi R, Nikniaz A, Marions L, Johansson A. Barriers to high-quality primary reproductive health services in an urban area of Iran: Views of public health providers. Midwifery. 2009;25:721–30. doi: 10.1016/j.midw.2008.01.002. [DOI] [PubMed] [Google Scholar]
- 8.Rasoulynejad S. Patient views for self-referral to specialists. Iran J Public Health. 2007;36:62–7. [Google Scholar]
- 9.Mohammad-Alizadeh S, Marions L, Vahidi R, Nikniaz A, Johansson A, Wahlström R. Quality of family planning services at primary care facilities in an urban area of East Azerbaijan, Iran. Eur J Contracept Reprod Health Care. 2007;12:326–34. doi: 10.1080/13625180701475723. [DOI] [PubMed] [Google Scholar]
- 10.Mohammad-Alizadeh S, Wahlstrom R, Vahidi R, Johansson A. Women's perceptions of quality of family planning services in Tabriz, Iran. Reprod Health Matters. 2009;17:171–80. doi: 10.1016/S0968-8080(09)33441-2. [DOI] [PubMed] [Google Scholar]
- 11.Hayter M. The structure of contraceptive education and instruction within nurse led family planning clinics: A grounded theory study. J Clin Nurs. 2009;18:2656–67. doi: 10.1111/j.1365-2702.2008.02651.x. [DOI] [PubMed] [Google Scholar]
- 12.Roudi F. Iran's revolutionary approach to family planning. Popul Today. 1999;27:4–5. [PubMed] [Google Scholar]
- 13.Creel LC, Sass JV, Yinger NV. Overview of quality of care in reproductive health: Definitions and measurements of quality. New Perspect Qual Care. 2002;1:1–7. [Google Scholar]
- 14.Vahidnia F. Case study: Fertility decline in Iran. Popul Environ. 2007;28:259–66. [Google Scholar]
- 15.Vakilian K, Mirzaii K. NajmAbadi. Reproductive health in Iran: International conference on population and development goals. Oman Med J. 2011;26:143–7. doi: 10.5001/omj.2011.36. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Ross J, Smith E. Trends in national family planning programs, 1999, 2004 and 2009. Int Perspect Sex Reprod Health. 2011;37:125–33. doi: 10.1363/3712511. [DOI] [PubMed] [Google Scholar]
- 17.Ehsanpour S, Mohammadifard M, Shahidi S, Nekouyi NS. A comparative study on attitude of contraceptive methods users towards common contraceptive methods. Iran J Nurs Midwifery Res. 2010;15(Suppl 1):363–70. [PMC free article] [PubMed] [Google Scholar]
- 18.Mekonnen W, Worku A. Determinants of low family planning use and high unmet need in Butajira District, South Central Ethiopia. Reprod Health. 2011;8:37. doi: 10.1186/1742-4755-8-37. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Shahidzadeh-Mahani A, Omidvari S, Baradaran HR, Azin SA. Factors affecting quality of care in family planning clinics: A study from Iran. Int J Qual Health Care. 2008;20:284–90. doi: 10.1093/intqhc/mzn016. [DOI] [PubMed] [Google Scholar]
- 20.Ghojazadeh M, Naghavi-Behzad M, Fardi-Azar Z, Saleh P, Ghorashi S, Pouri AA. Parental knowledge and attitudes about human papilloma virus in Iran. Asian Pac J Cancer Prev. 2012;13:6169–73. doi: 10.7314/apjcp.2012.13.12.6169. [DOI] [PubMed] [Google Scholar]