

Abstract
Background:
Appropriate infant feeding is the key to optimum infant and child development and survival. This study investigates age-appropriate infant feeding practices and nutritional status of infants attending the immunization and child welfare clinic at Aminu Kano Teaching Hospital.
Materials and Methods:
Using a cross-sectional descriptive design, a sample of 300 sets of infants (age ≤12 months) and caregivers was systematically selected and studied. The data were analyzed using the MINITAB® 12.21 (USA) statistical software.
Results:
All the infants studied were still on breast milk. Most of the mothers demonstrated correct body positioning (89.9) and attachment (78.7%) during breastfeeding, and effective suckling was demonstrated in 77.0%. Interestingly, none of the infants was either exclusively breastfed for 6 months or currently on exclusive breastfeeding. Furthermore, only 64 (58.2%) of the 110 infants that were more than 6 months of age had appropriately been started on complementary feeding from 6 months of age. Overall, most caregivers (88.7%) had “fair” to “good” infant feeding practices. The practices were significantly associated with their level of education, and their relationship with the infants. Up to 40.0% and 73.7% of the infants had varying degrees of wasting and stunting respectively. Infant feeding practices and the age of the infants emerged as the only factors significantly associated with stunting, while both the caregivers’ practices and age of the infants emerged as significant predictors of wasting in the infants.
Conclusion and Recommendations:
Barely 3 years to the 2015 target of the millennium development goals (MDGs), infant feeding and nutritional status still poses a serious threat to the dream of realizing the MDG-4. The Ministry of Health and relevant developing partners in this region should as a matter of urgency, formulate and implement a strong community-based public health intervention program to improve the knowledge and practices of mothers on infant feeding.
Keywords: Age-appropriate feeding, infant feeding practices, Kano-Nigeria, nutritional status
INTRODUCTION
Good infant feeding and healthcare are critical for growth and development of children in the first few years of life. Optimal infant feeding practice recommended by World Health Organization (WHO) and United Nations Children's Fund involves exclusive breastfeeding for the first 6 months of life, followed by adequate complementary feeding, and breastfeeding until the child is at least 2 years old.[1] This feeding pattern is expected to supply the macro and micronutrients in adequate amounts required for optimal growth and development of the child.[1] Globally, an estimated 1.3 million lives are lost each year as a result of the lack of exclusive breastfeeding and another 600,000 from not continuing breastfeeding with proper complementary feeding.[2] Breastfeeding remains a pivotal factor between life and death for the vast majority of children in developing countries such as Nigeria, but the current data reveals that 55% of Nigerian mothers are ignorant of the importance of exclusive breastfeeding.[3] Also, the underlying factor of more than 50% of all childhood deaths in Nigeria is under-nutrition.[4]
Appropriate complementary feeding requires not only introducing foods too early or too late to infants, but also feeding infants and young children between 6 and 24 months foods considered safe and nutritionally adequate without discontinuing breastfeeding.[5] However, despite the unparalleled benefits of optimal infant feeding, less than 35% of infants worldwide are exclusively breastfed during first 6 months of life.[2] A study from Kano, Nigeria revealed that the proportion of mothers who exclusively breastfed their babies for 1 month, 3 months and 6 months after their last delivery were 26.0% 24.8% and 22.0% respectively.[6] A similar study from southern Nigeria also reported that more than 90% of mothers had adequate knowledge of exclusive breastfeeding, 21.2% practiced exclusive breastfeeding for all their children, 51.6% had never practiced exclusive breastfeeding with any child.[7]
Several changes have occurred in the traditional breastfeeding and weaning practices in sub-Saharan Africa over the years. These changes emanated from the introduction of alien cultures and values; and urbanization with the consequent changes in lifestyle. Furthermore, many mothers in sub-Saharan Africa do not know the appropriate time to initiate breastfeeding, have little knowledge of the proper positioning and attachment of infants to the breast for breastfeeding; or have little knowledge of when and what to introduce as complementary feeds. These deviations from what is appropriate during infancy and early childhood may result in irreversible faltering in linear growth and cognitive deficit. Growth during 1st year of life is greater than at any other time after birth and good nutrition during this period of rapid growth is vital to ensure that the infant develops both physically and mentally to the fullest potential.[8] Thus, appropriate feeding practice is an early investment towards the making of a healthy generation. This study was, therefore, to investigate the infant feeding practices of caregivers for the different age groups of infants attending the immunization and child welfare clinic at Aminu Kano Teaching Hospital (AKTH), and how this relates to their nutritional status. It was also to determine the correlates of the observed feeding practices and the nutritional status of the infants. It is envisaged that the information would be useful to policy makers and programme managers especially for the achievement of millennium development goals (MDG)-4, i.e., the reduction of child mortality.
MATERIALS AND METHODS
Kano is the largest commercial center in Northern Nigeria and the most populous state, according to the 2006 Nigeria Population Census. The majority of patients who come to this hospital are indigenous Hausa and Fulani, although members of other ethnic groups such as the Yoruba and Igbo also constitute a substantial part of the clientele. Most of the people of Kano state are traders, farmers, or civil servants; and the predominant religions are Islam and Christianity.
In the heart of Kano city is situated AKTH, a 500 bed tertiary hospital that provides health services to the population in Kano and the neighboring states. The immunization and child welfare clinic of the hospital offers immunization, nutrition services and treatment of minor ailments to children under the age of five. The clinic operates 5 times a week, attending to an average of 100 clients/day.
The study was cross-sectional descriptive in design. We studied a sample of 300 sets of infants (age ≤12 months) and their caregivers systematically selected over 1 month between September and October 2012. The required sample size was arrived at using an appropriate statistical formula for calculating minimum sample size for descriptive studies,[9] and prevalence of 75.6% for babies that were appropriately breastfed up to 18 months obtained from a past study.[10] The sample was selected using a sampling interval of two obtained by dividing the average monthly attendance of the clinic with the required sample size, i.e., 2000/300. Thus, one in every seven caregiver-infant sets was selected until the required sample was met. Informed consent was obtained from the caregivers before administering the questionnaire. Literate respondents indicated acceptance by signing the consent form while non-literate participants affixed their thumbprint. Data was collected using a pretested semi-structured interviewer administered questionnaire that provides for eliciting information on the socio-demographic profile of the caregivers and the infants, the infant feeding practices consisting of questions around the type, method and timing of feeds and a structured observation of breastfeeding for correctness of body positioning, attachment and effective suckling based on the WHO breastfeeding criteria;[11] and weights and heights of the infants. Babies that were more than 1 year old at the time of the study and those whose caregivers did not give consent for the study were excluded from the study. Ethical approval was obtained from the ethics committee of AKTH before conducting this study.
The collected data were analyzed using the MINITAB® 12.21 (USA) statistical software. Absolute numbers and simple percentages were used to describe categorical variables while quantitative variables were described using mean and standard deviation. Infant feeding practice was scored using a scoring and grading system adopted from a past study[12] where one point was accorded for any correct practice and zero was accorded for a wrong practice. Out of a maximum of 21 points, respondents that scored 0-7 points were considered to have poor practice of infant feeding while those that scored 8-14 or 15-21 points were adjudged to have fair or good practice respectively. Furthermore, the nutritional status of the infants was assessed by first comparing the infants’ weights and lengths with the median z scores of the WHO weight for length and length for age reference cards.[13] The Waterlow's classification of malnutrition was then used to determine wasting and stunting in the infants.[14] Thus, infants that had more than 95% of the median reference values of their length for age were considered to have normal nutrition status while those that had 87.5-95% and 80-87.5% of the reference values were considered to have moderate and mild stunting respectively. Those whose length for age values were less than 80% of the reference values were adjudged to have severe stunting. In the same vein, infants whose weight for length was more than 90% of the median reference values were considered to have normal nutrition status while those with 80-90% and 70-80% of the reference values were considered to have moderate and mild wasting respectively and those with less than 70% of the reference values were adjudged to have severe wasting.
The Chi-square test (χ2) was used to determine the association between categorical variables. Significance level of P was fixed at ≤0.05. Binary logistic regression was used to determine the associates of infant feeding practices and the nutrition status of the infants.
RESULTS
Socio-demographic characteristics of the respondents
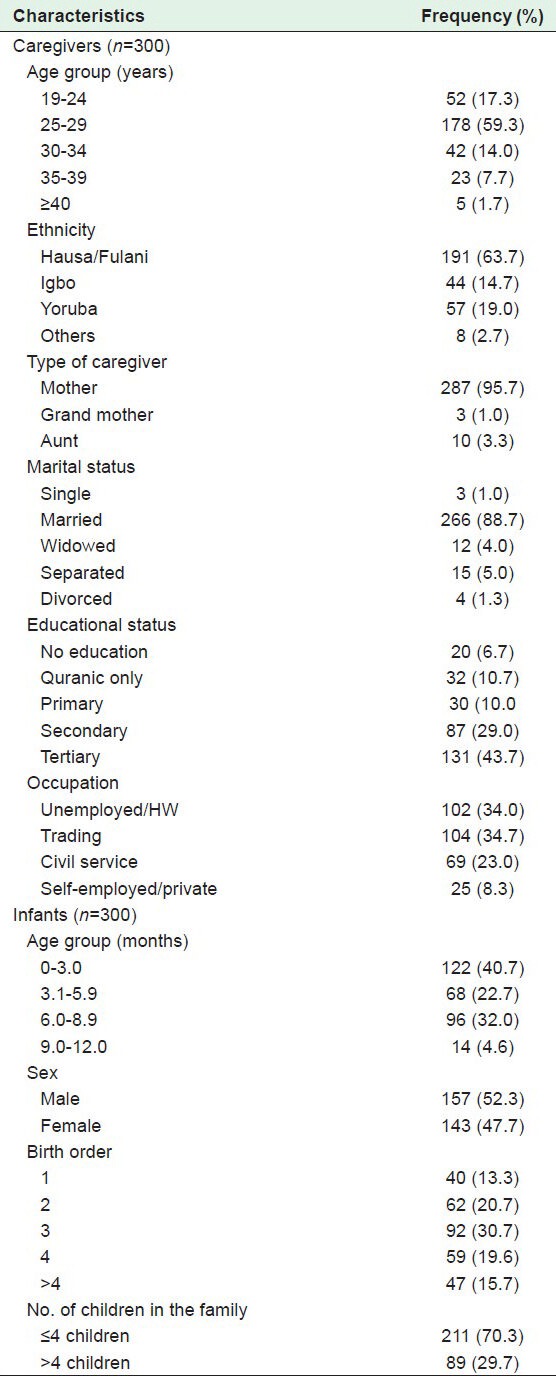
Three hundred questionnaires were administered to mothers at the immunization clinic and child welfare clinic of AKTH by trained interviewers. The age of the mothers ranged from 19 to 50 years with a mean of 28.0 ± 5.5 years. The majority (59.3%) were in the age group 25-29 years, Hausa and Fulani ethnic groups made up 63.7%, 95.7% were mothers of children; and 72.7% had at least secondary level of education. The mean age of the infants was 147 ± 99 days. More than half (52.3%) were males, and were 0-90 days (0-3 months old) as shown in Table 1.
Table 1.
Caregivers’ and infants’ biological and socio-demographic characteristics
Caregivers’ infant feeding practices
The majority of the infants 190 (63.3%) were aged 6 months and below while the remaining 110 (36.7%) were more than 6 months of age. All the infants studied were still on breast milk. More than half (65.0%) were put to the breast within an hour of delivery, and 63.3% had breast milk as their first feed. Most of the mothers demonstrated correct body positioning (89.9) and attachment (78.7%) during breastfeeding, and effective suckling was demonstrated in 77.0%. Interestingly, none of the infants was either exclusively breastfed for 6 months or is currently on exclusive breastfeeding. About a quarter (24.2%) of those infants who were younger than 6 months were already commenced on water, and the remaining 144 (75.8%) on a type of complementary feed in addition to water. Furthermore, only 64 (58.2%) of the 110 infants that were more than 6 months of age were appropriately commenced complementary feeding from 6 months of age. The type of complementary feeds used is as depicted in Figure 1. More than one-third (36.2%) used porridge or gruel made from a mixture of maize or sorghum flour and soya beans flour. The parameters that were used for the assessment of the infant feeding practices are summarized in Table 2.
Figure 1.
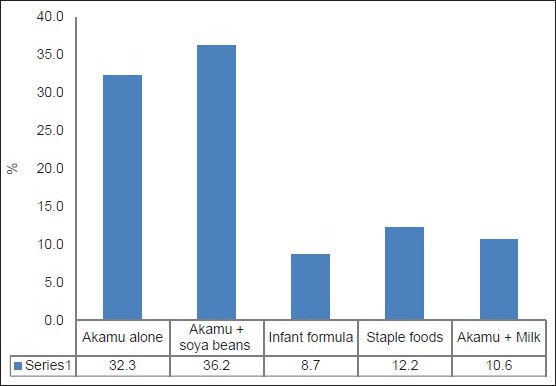
Type of complementary feeds given to infants (n=254). *Akamu is porridge or gruel made from ground maize or sorghum, traditionally or locally used as a complementary feed
Table 2.
Parameters for assessing the caregivers’ infant feeding practices
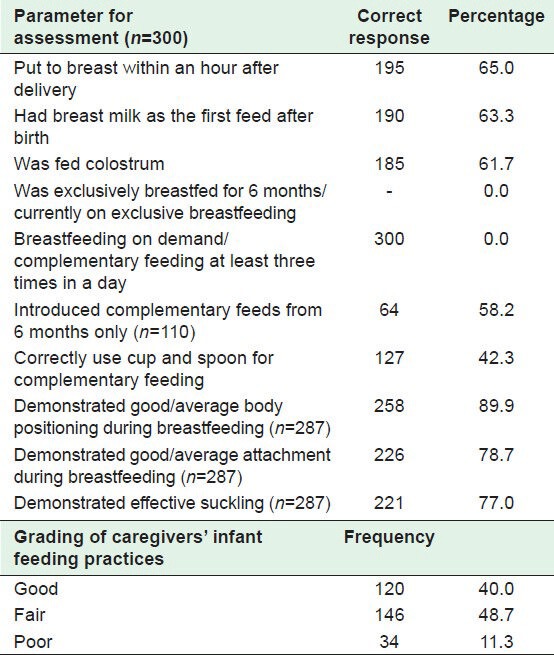
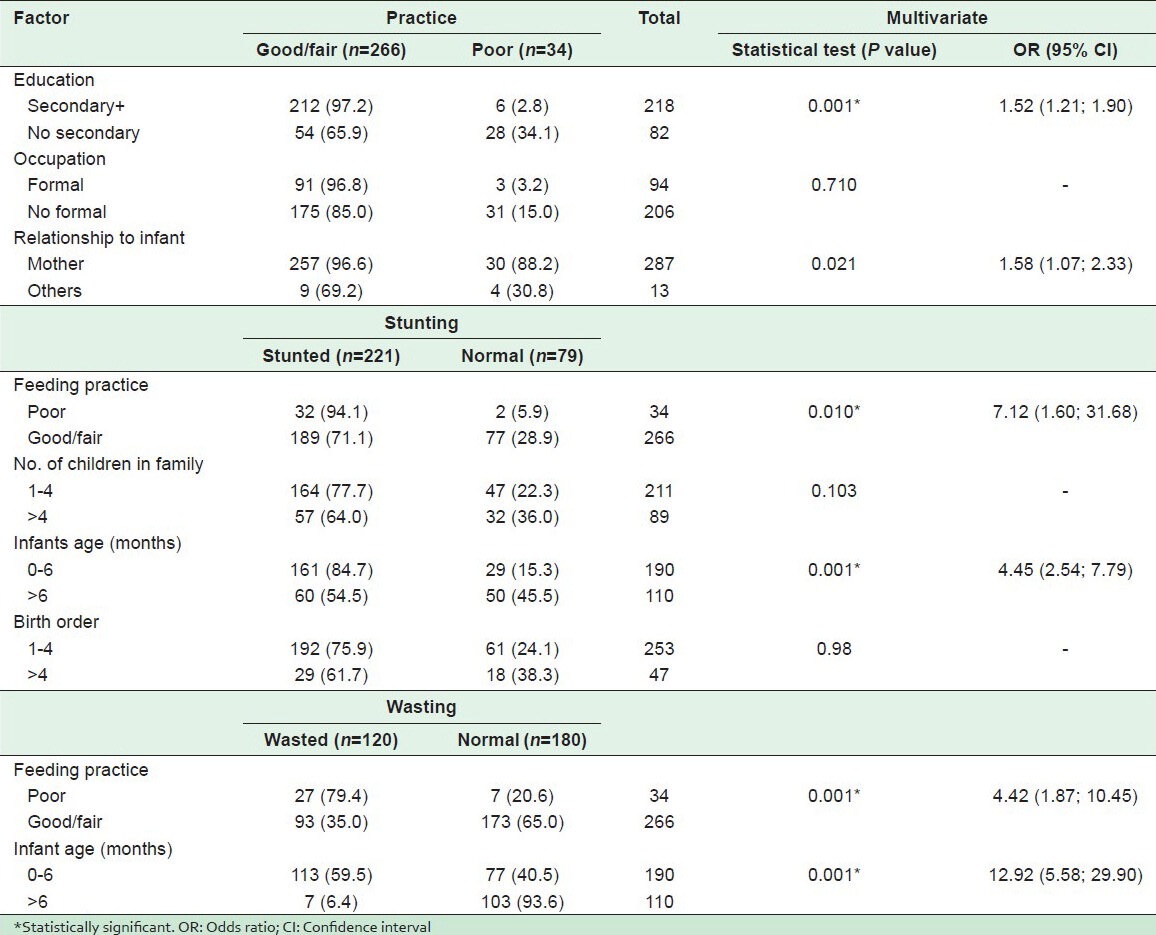
We graded the respondents based on their scores on the parameters we used to assess their infant feeding practices. We found that most (88.7%) had “fair” to “good” infant feeding practices [Table 2]. The caregivers’ practices were significantly associated with their education (χ2 = 58.4, P < 0.05), occupations (χ2 = 9.0, P < 0.05), and their relationship with infant (Fisher exact P < 0.05) but, not with their ages (Fisher exact P = 0.606), ethnicity (χ2 = 1.91, P = 0.167), marital status (Fisher exact P = 0.226), number of children in the family (χ2 = 0.114, P = 0.736); or with the ages (χ2 = 0.87, P = 0.351) and the birth order of the infants (χ2 = 0.87, P = 0.351). However, on binary logistic regression using a model comprising the three associated variables, level of education of the mothers (z = 3.65, P < 0.05) and relationship of the caregivers with the infant (z = 2.31, P < 0.05) emerged as the only predictors of the infants’ feeding practices. Caregivers that have at least secondary school level education were 1½ times more likely to have “fair to good” infant feeding practices compared to those without secondary school education (odds ratio [OR] =1.52, 95% confidence interval [CI] OR [1.21; 1.90]). Similarly, caregivers that were mothers of the infants were also 1½ times more likely to have “fair to good” practices of infant feeding (OR = 1.58) (95% CI OR [1.07; 2.33]) compared to the other categories of caregivers. None of the infant social or biological characteristics influenced the respondents’ practices [Table 3].
Table 3.
Factors associated with infant feeding practices and nutrition status
Nutritional status of the infants
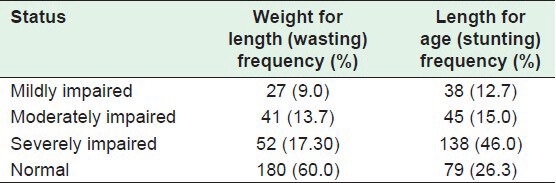
The nutritional status of the infants is as summarized in Table 4. Up to 40.0% and 73.7% of the infants assessed had varying degrees of wasting and stunting respectively. On bivariate analysis, the caregivers’ infant feeding practices (χ2 = 8.27, P < 0.05) and the number of children in the family (χ2 = 6.0, P < 0.05) were found to be significantly associated with stunting in the infants. The infants’ variables associated with stunting include age (χ2 = 32.7, P < 0.05) and birth order of the infants (χ2 = 4.1, P < 0.05). On multivariate analysis using a combination of the significant caregiver and infant variables, the caregivers’ infant feeding practices and the age of the infants were the only factors found to be significantly associated with stunting [Table 3]. In the same vein, an analysis of the factors that are associated with wasting in the infants revealed at the bivariate level that the caregivers’ infant feeding practices (χ2 = 24.8, P < 0.05) and age of the infants (χ2 = 81.9, P < 0.05) were the only factors significantly associated. The number of children in the family (χ2 = 2.09, P = 0.149) and birth order of the infants (χ2 = 0.82, P = 0.364) were not associated with wasting. On multivariate analysis, both the caregivers’ practices and age of the infants emerged as significant predictors of wasting in the infants [Table 3].
Table 4.
Nutritional status of infants
DISCUSSION
We observed in this study that many of the mothers initiated breastfeeding within 1 h of delivery, but sadly none of them was practicing exclusive breastfeeding at the time of the study. These mothers started well, but as noted in previous studies, introduced other liquids with or without solids resulting in declining prevalence of exclusive breastfeeding; almost approaching zero before and at 6 months.[15,16] The strong cultural myth in Africa that infants must be given water to prevent dehydration may have contributed to the non-practice of exclusive breastfeeding as noted amongst mothers in this study and similar African studies.[7,17,18,19] Studies from Nigeria[7,20] including the 2011 “Saving Newborn Lives” maternal, newborn, child health survey reported that Nigeria was one of the countries with the lowest rates of exclusive breastfeeding on the African continent. Recent data indicates that the percentage of infants exclusively breastfed to the age of 6 months declined from 17% in 2003 to 13% in 2008.[21] The zero prevalence observed in this study may suggest a further decline in the practice. The situation becomes more alarming because the study was conducted in a tertiary health institution where the majority of the clients presumably were of a high socioeconomic background as demonstrated in this study. However, the developed world has also noted a less than optimal prevalence rate of the practice of exclusive breastfeeding[16] A zero awareness of breastfeeding had been noted in some rural areas of Nigeria some years ago.[5]
Infant feeding practice is a major determinant of nutritional status of infants as shown in this study. Although the majority (88.7%) of the care givers had fair/good infant feeding practice, there was evidence of long term poor infant feeding (stunting) in about three-quarters of the children. This is a pointer to the fact that malnutrition begins early in life with poor infant feeding practices such as the lack of exclusive breastfeeding, and the institution of complementary feeds earlier than recommended as this study indicates. The high prevalence of wasting and stunting observed in the infants studied may have resulted from the early introduction of complementary feeds, possibly of poor quality and perhaps augmented by the frequent bouts of diarrhea associated with contamination of the feeds. A Malawian study showed that infants that were commenced early on complementary feeds progressively had lower weight for age from as early as 2 months,[22] corroborating the fact that breast milk is the full diet required by the human baby at that early stage of development. Interestingly, despite the low practice of exclusive breastfeeding reported from Nairobi, Kenya (5.2%), the figures for underweight (6.5%), wasted (6.3%) and stunted (11.7%) children were much lower than observed in our study. This could be the result of differences in the pattern of complementary feeding according to the local norms and culture.[23] Furthermore, a retrospective survey of mildly wasted children admitted to the community program on nutrition in Nias Island, Indonesia, revealed that only 12% of the 215 children examined were exclusively breastfed for up to 6 months of age. Supplementary liquids were given besides breast milk within the first 7 days of life by 74% of mothers, and 79% of infants were given solid, semi-solid or soft foods as complementary feeds before 6 months.[24]
We observed that caregivers with at least secondary education, formal occupation and who were mothers of the infants were significantly better in their infant feeding practices. Education plays a beneficial role in many health seeking behaviors, and has been noted to be a major determinant in achieving positive health outcomes for mothers, promoting child survival and improving the health of the family as a whole.[16,24,25] Furthermore, it is acknowledged that better education usually connotes better health.[26] The preliminary finding on bivariate analysis that caregivers with formal occupation had better infant feeding practices is not surprising as occupational status is often linked to educational status. Better educated individuals are more likely to be employed in the formal sector and practices such as good infant feeding may be common to both groups. On the other hand, working mothers may not always be available to their children and this can adversely affect breastfeeding. A Canadian study noted that women with formal employment were less likely to exclusively breast feed their infants for 6 months. This was attributed to their early return to work post-partum.[16] In addition, caregivers who were mothers of the infants had better feeding practices as seen in this study since perhaps maternal health is intertwined with child health.[4] Efforts directed at attaining MDG-5, that is, a reduction of maternal mortality and ensuring that mothers stayed alive to care for their own children may be one of the surest means of attaining MDG-4, as care given by a mother to her infant may not be comparable to what other care givers will provide.
The 2015 target for the achievement of the MDGs is only 3 years away, but the key to infant and child development and survival in Kano as measured by the infant feeding and nutritional status still poses a serious threat to the realization of these goals. The ministry of health and the relevant developing partners in this region should as a matter of urgency develop and implement a good community-based Public health intervention program to improve the knowledge and practices of mothers on infant feeding.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Azubuike N, Nkanginieme KE. 2nd ed. Port Harcourt (Nig): University of Port Harcourt Press; 2007. Infant feeding. Paediatrics and Child Health in a Tropical Region; pp. 224–67. [Google Scholar]
- 2.Geneva: WHO; 2003. [Last accessed on 2012 Dec 13]. WHO/UNICEF. Global Strategy for Infant and Young Child Feeding; pp. 5–10. Available from: http://www.books.google.com.ng/books?id=biABXOXrajYC and printsec=frontcover and source=gbs_ge_summary_r and cad=0#v=onepage and q and f=false . [Google Scholar]
- 3.Ibadan (Nig): IITA; 2004. [Last accessed on 2012 Dec 13]. International Institute of Tropical Agriculture. Nigeria Food Consumption and Nutrition Survey: 2001-2003; pp. 46–9. Available from: http://www.pdf.usaid.gov/pdf_docs/PNADC880.pdf . [Google Scholar]
- 4.UNICEF. Maternal and child health. [Last accessed on 2013 Jan 2]. Available from: http://www.unicef.org/nigeria/children_1926.html .
- 5.Frongillo EA. Undertaking challenges of improving complimentary feeding of infants and young children. SCN News. 2006;27:41–2. [Google Scholar]
- 6.Iliyasu Z, Kabir M, Abubakar IS, Galadanchi NA. Current knowledge and practice of exclusive breastfeeding among mothers in Gwale local government area of Kano State. Niger Med Pract. 2005;48:50–5. [Google Scholar]
- 7.Uchendu UO, Ikefuna AN, Emodi IJ. Factors associated with exclusive breast feeding among mothers seen at the University of Nigeria teaching hospital. J Child Health. 2009;3:14–9. [Google Scholar]
- 8.Alamu TO, Atawodi SE, Edokpayi JN. Nutritional status of infants attending infant welfare clinic of Ahmadu Bello University, health service Samaru. Adv Appl Sci Res. 2011;2:58–64. [Google Scholar]
- 9.Lwanga SK, Lemeshow S. Geneva, Switzerland: Publication of World Health Organization; 1991. Sample Size Determination in Health Studies: A Practical Manual; pp. 1–3. [Google Scholar]
- 10.Iliyasu Z, Kabir M, Abubakar IS, Galadanci NA. Current knowledge and practice of exclusive breast feeding among breast feeding mothers in gwale local government area of Kano State. Niger Med Pract. 2005;48:50–5. [Google Scholar]
- 11.Goyal RC, Banginwar AS, Ziyo F, Toweir AA. Breastfeeding practices: Positioning, attachment (latch-on) and effective suckling-A hospital-based study in Libya. J Family Community Med. 2011;18:74–9. doi: 10.4103/2230-8229.83372. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Lawan UM, Abubakar S, Gambo MD. HIV risk behaviors and knowledge of HIV/AIDS and its prevention among unmarried adolescents in Kano metropolis, Northwestern Nigeria. J Behav Health. 2012;1:252–9. [Google Scholar]
- 13.WHO/UNICEF. WHO child growth standards and the identification of severe acute malnutrition in infants and children. [last accessed on 2012 Dec 13]. Available from: http:// www.who.int/nutrition/publications/severemalnutrition/9789241598163_eng.pdf .
- 14.Park K. Park's Textbook of Preventive and Social Medicine. 18th ed. India: M/s Banarsidas Bhanot Publishers; 2005. Nutritional problems in public health; pp. 462–8. [Google Scholar]
- 15.Petrova A, Ayers C, Stechna S, Gerling JA, Mehta R. Effectiveness of exclusive breastfeeding promotion in low-income mothers: A randomized controlled study. Breastfeed Med. 2009;4:63–9. doi: 10.1089/bfm.2008.0126. [DOI] [PubMed] [Google Scholar]
- 16.Al-Sahab B, Lanes A, Feldman M, Tamim H. Prevalence and predictors of 6-month exclusive breastfeeding among Canadian women: A national survey. BMC Pediatr. 2010;10:20. doi: 10.1186/1471-2431-10-20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Awogbenja MD. Factors influencing breastfeeding practice. PAT. 2010;6:126–38. [Google Scholar]
- 18.Kakute PN, Ngum J, Mitchell P, Kroll KA, Forgwei GW, Ngwang LK, et al. Cultural barriers to exclusive breastfeeding by mothers in a rural area of Cameroon, Africa. J Midwifery Womens Health. 2005;50:324–8. doi: 10.1016/j.jmwh.2005.01.005. [DOI] [PubMed] [Google Scholar]
- 19.Anigo KM, Ameh DA, Ibrahim S, Danbauchi SS. Infant feeding practices and nutritional status of children in North Western Nigeria. Asian J Clin Nutr. 2009;1:12–22. [Google Scholar]
- 20.Oche MO, Umar AS, Ahmed H. Knowledge and practice of exclusive breastfeeding in Kware, Nigeria. Afr Health Sci. 2011;11:518–23. [PMC free article] [PubMed] [Google Scholar]
- 21.Abuja, Nigeria: 2011. Jan, [Last accessed on 2013 Apr 28]. Federal Ministry of Health. Saving Newborn Lives in Nigeria: Newborn Health in the Context of the Integrated Maternal Newborn, and Child Health Strategy. Available from: http://www.countdown2015 mnch.org/countdown-news/28-saving-newborn-lives-in-nigeria-newborn-health-in-the-context-of-the-integrated-maternal-newbornnd-child-health-strategy . [Google Scholar]
- 22.Kalanda BF, Verhoeff FH, Brabin BJ. Breast and complementary feeding practices in relation to morbidity and growth in Malawian infants. Eur J Clin Nutr. 2006;60:401–7. doi: 10.1038/sj.ejcn.1602330. [DOI] [PubMed] [Google Scholar]
- 23.University of Nairobi. Infant feeding practices and nutritional status of children aged 0-12 months among Somali community in Eastleight Estate, Nairobi Kenya. Postgraduate student project for the year. [Last accessed on 2013 Apr 28]. Available from: http://www.uonbi.ac.ke/faculties/postgrad-student-projects-details.php?project_id=5722 and fac_code=21 .
- 24.Inayati DA, Scherbaum V, Purwestri RC, Hormann E, Wirawan NN, Suryantan J, et al. Infant feeding practices among mildly wasted children: A retrospective study on Nias Island, Indonesia. [Last accessed on 2013 Apr 28];Int Breastfeed J. 2012 7:3. doi: 10.1186/1746-4358-7-3. Available from: http://www.internationalbreastfeedingjournal.com/content/7/1/3 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Nankabirwa V, Tylleskär T, Tumwine JK, Sommerfelt H Promise-ebf Study Group. Maternal education is associated with vaccination status of infants less than 6 months in Eastern Uganda: A cohort study. BMC Pediatr. 2010;10:92. doi: 10.1186/1471-2431-10-92. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Bicego GT, Boerma JT. Maternal education and child survival: A comparative study of survey data from 17 countries. Soc Sci Med. 1993;36:1207–27. doi: 10.1016/0277-9536(93)90241-u. [DOI] [PubMed] [Google Scholar]