

Abstract
Background
Depression is associated with poor adherence to medications and worse prognosis in patients with acute coronary syndrome (ACS).
Purpose
To determine whether cognitive, behavioral, and/or psychosocial vulnerabilities for depression explain the association between depression and medication adherence among ACS patients.
Methods
169 ACS patients who agreed to have their aspirin adherence measured using an electronic pill bottle for 3 months were enrolled within 1 week of hospitalization. Linear regression was used to determine whether depression vulnerabilities predicted aspirin adherence after adjustment for depressive symptoms, demographics, and comorbidity.
Results
Of the depression vulnerabilities, only role transitions (beta = −3.32; p=0.02) and interpersonal conflict (beta −3.78; p=0.03) predicted poor adherence. Depression vulnerabilities did not mediate the association between depressive symptoms and medication adherence.
Conclusions
Key elements of the psychosocial context preceding the ACS including major role transitions and conflict with close contacts place ACS patients at increased risk for poor medication adherence independent of depressive symptoms.
Keywords: medication adherence, depression, acute coronary syndrome, interpersonal conflict, role transitions
Background
Depression after acute coronary syndrome (ACS; unstable angina and myocardial infarction) is an established risk factor for poor prognosis. ACS patients with elevated depressive symptoms have approximately twice the risk of ACS recurrence or mortality.(1–3) One mechanism postulated to mediate the association between depression and prognosis after ACS is poor adherence to cardiovascular medications. There is a strong, consistent relationship between depression and poor medication adherence in cardiovascular(4, 5) and other medical populations.(6) Even patients with mild depressive symptoms are at risk for poor adherence.(4) Poor adherence to cardiovascular medications has been associated with poor prognosis(7, 8), and in one study, we have shown that poor adherence to aspirin appears to partially mediate the association between depression and prognosis after ACS.(9) Despite the strong association between depression and poor adherence, interventions to improve depressive symptoms have not led to reliable improvements in medication adherence, even when these interventions have successfully reduced depressive symptoms.(10, 11) Accordingly, there is still a need to better understand the association between depression and poor adherence to medications.
Depression is a multifaceted psychological disorder that arises from a combination of genetic, biological, and environmental factors in patients with underlying vulnerabilities.(12) These vulnerabilities can be grouped into behavioral, cognitive, and/or psychosocial elements that predispose individuals to developing depression. We have previously explored the intercorrelations and prevalence of these three categories of vulnerability in post-ACS patients. We showed that the intercorrelations between these vulnerabilities were low and that there was a higher prevalence of each vulnerability in depressed as compared to non-depressed patients.(13) Each of these more trait-like vulnerabilities has the potential to influence adherence behavior. For example, patients who are not sufficiently behaviorally activated to schedule pleasurable activities may have low overall motivation for self-care activities including medication adherence. Patients with maladaptive cognitive schema may hold dysfunctional attitudes about the risks and benefits of medications that in turn lead them to not adhere to their regimens. Finally, patients who experience vulnerabilities in their psychosocial milieu either in the form of interpersonal conflicts with their partners or major life events may have lower adherence due to limitations in social support or disruptions in habits that support medication adherence. A better understanding as to which of these underlying depression vulnerabilities is associated with adherence and whether they mediate the effect of depressive symptoms on adherence may inform the development of interventions to improve medication adherence among patients with depression.
Accordingly, we tested the association of depression to medication adherence with and without including depression vulnerabilities in a model predicting medication adherence. We hypothesized that when depression vulnerabilities were added to the model, the association between depression and adherence would be mediated, at least in part, by one or more of the depression vulnerabilities.
Methods
Patients
The current analyses utilized data from the Coronary Psychosocial Evaluation Studies (COPES), a series of multi-site observational cohort studies that concern the relationship between depression and prognosis after ACS.(14) To be included in COPES, patients had to be hospitalized for an ACS and have a score on the Beck Depression Inventory (BDI) of <5 or ≥10, ranges selected to delineate not depressed and depressed status at the time of hospitalization for an ACS. Patients were excluded if they lived in a nursing home, exhibited cognitive impairment, or engaged in alcohol or substance abuse. A subset of patients who were prescribed aspirin had their adherence assessed by an electronic pill cap (N=172), and these patients are included here. The study was approved by the Institutional Review Boards at each participating hospital and all patients provided informed consent prior to enrollment and data collection.
Procedure
Details regarding enrollment into COPES have been described elsewhere.(5) Briefly, between May 1, 2003 and April 15, 2005, patients were recruited from 3 academic hospitals (Yale-New Haven Hospital and Hospital of St. Raphael in New Haven CT; Mount Sinai Hospital in New York City) within 1 week of hospitalization for an ACS, defined as either acute myocardial infarction (MI) or unstable angina using standard criteria.(15) A cardiologist confirmed ACS eligibility for all patients. In addition to depression eligibility being determined by BDI, patients completed questionnaire assessment of depression vulnerabilities and other key study measures. Upon hospital discharge, patients were provided with a 90-day supply of their prescribed aspirin in a Medication Event Monitoring System (MEMS; APREX Corp, Fremont, CA) bottle. At 3 month follow-up, patients returned the MEMS bottle cap.
Measures
Medication adherence
The MEMS device contains an electronic chip in the bottle cap that records the date and time whenever the bottle cap is opened. MEMS data were collected continuously over the 3 months following discharge for the index ACS event. The percentage of days the bottle cap was opened the correct number of times (once a day) was calculated.
Depression Vulnerabilities
1. Cognitive Vulnerability
We used the 24-item version of the Dysfunctional Attitudes Scale (DAS-24) to measure attitudes and beliefs that represent a cognitive vulnerability to depression.(16, 17) Sample items include: “If others dislike you, you cannot be happy” and “If a person asks for help, it is a sign of a weak person”. Items are rated on a 7-point scale ranging from 1 (totally agree) to 7 (totally disagree). Scores were recoded so that higher scores indicate higher levels of cognitive dysfunction. No time period for holding these attitudes is specified for this measure. The measure had good internal consistency (Cronbach α = 0.84).
2. Behavioral Vulnerability
We used the 20-item short version of the Pleasant Events Schedule for the Elderly (PES-E) to assess behavioral vulnerability to depression.(18) On the PES-E participants indicate how frequently they engaged in or had experienced each of 20 pleasant events during the past month. Answer options are 0 (not at all), 1 (1–6 times) and 2 (≥7 times). Missing items were coded as ‘0’ if at least 50% of the 20 items had been answered. Items were recoded so that higher scores indicate infrequency of pleasant events. There was good internal consistency with this measure (Cronbach α = 0.84).
3. Psychosocial Vulnerability
i. Role Transitions
We generated a list of role transitions based on the Interpersonal Problem Area Rating Scale(19) to assess social vulnerability to depression. Potential role transitions included geographic move, marriage or cohabitation, separation or divorce, graduation or new job, loss of job or retirement, and health problems other than coronary heart disease. Participants were asked to indicate whether they had experienced any of these events within the past year. They were also asked to name any other significant positive or negative events that had occurred within the past year. Items were summed to provide the total number of role transitions, not including heart disease, in the year prior to the ACS.
ii. Interpersonal Conflict
We used questions from the Dyadic Adjustment scale to assess interpersonal conflict.(20) Patients are asked to name the one person closest to them and to rate the extent to which they agreed or disagreed with that person on 15 important issues (e.g., handling finances, making major decisions, friends, or philosophy of life). Answers range from 1 (always disagree) to 6 (always agree). Scores were recoded such that higher scores reflected higher disagreement and a mean score was calculated so long as patients had provided responses to at least 6 items. The measure had good internal consistency (Cronbach α = 0.92).
Depressive Symptoms
We measured depressive symptoms using the Beck Depression Inventory (BDI).(21) The BDI consists of 21 items describing cognitive-affective and somatic depression symptoms. Patients rate the extent to which each symptom had been present in the prior week on a 4-point scale (0–3). The BDI has been used in prior studies of depression and ACS, and elevated scores predict shorter post-ACS event-free survival.(22) A score ≥ 10 is consistent with at least mild to moderate depression. The BDI had good internal reliability (Cronbach α = 0.90) in our sample.
Covariates
Baseline demographics and clinical variables, including the constituents of the Charlson comorbidity index, a validated measure of risk for death in patients with chronic illness,(23) were obtained by patient interview and chart abstraction at the time of enrollment.
Analytic Plan
In cases of partial missing data on depression vulnerability scales, total scores were imputed from the subset of answered questions using a regression based approach so long as the total R-squared of the regression equation predicting the total score was >75%. This approach led to three participants missing data on the Dyadic Disagreement scale. One of these three participants was also missing data pertinent to role transitions. Only patients with data for all of the vulnerabilities were included in these analyses such that the total sample was comprised of 169 patients.
As per convention in cardiovascular adherence studies, patients were defined as poor adherers if they took their aspirin correctly on fewer than 80% of days monitored.(24) Patient characteristics were then compared according to adherence status, using chi-squared tests for proportions and t-tests for normally distributed continuous variables. Homogeneity of variance was assessed when determining whether data was normally distributed. In cases where continuous variables were not normally distributed, data transformation (e.g., square-root transformation) was applied. Mann-Whitney test was used to compare role transitions, the DAS, and Charlson scores as transforming these data did not fit a normal distribution.
Linear regression was used to determine whether depression vulnerabilities were significantly associated with a continuous measure of adherence. In the first step, sociodemographics (age, gender, race, partner status), comorbidity (Charlson), and depressive symptoms (BDI score) at baseline were entered into the model. Depression vulnerabilities were then entered individually. We also tested a model in which the depression vulnerabilities were entered concurrently. As the distribution of medication adherence was negatively skewed, we performed a sensitivity analysis in which we transformed our measure of adherence to a measure of non-adherence (i.e., 1 – adherence) and then applied a square root transformation such that our dependent variable (adherence) approached a normal distribution. There were no differences in the pattern of association between depressive symptoms and depression vulnerabilities with medication adherence when we transformed the adherence variable. Accordingly, for ease of interpretability, we only present data for the untransformed measure of adherence. We used Preacher and Hayes’ bootstrap method with 1,000 bootstrap samples to determine whether the depression vulnerabilities, as a group, mediated the association between depressive symptoms and medication adherence.(25) Two-tailed probability levels are reported for all analyses. All statistical analyses were performed using SPSS 20 (Chicago, Inc.).
Results
The mean age of participants was 59 years, 44% were women, 86% were white, and 65% had a partner or spouse. The majority of participants were hospitalized for a myocardial infarction (26% ST-elevation myocardial infarction; 33% non-ST elevation myocardial infarction, 41% unstable angina). Twenty-seven percent of participants had a prior history of MI. Thirty percent had a prior history of depression and 20% of participants were prescribed antidepressants at discharge. The majority of the sample had minimal depressive symptoms during ACS hospitalization (54% with BDI < 5), 27% had mild to moderate depressive symptoms (BDI 10–18), and 19% had moderate to severe depressive symptoms (BDI ≥19). Poor adherence to aspirin (took aspirin correctly on <80% of days) was observed for 23%. There were no significant differences in sociodemographic characteristics between patients who had poor (<80%) and good (≥80%) adherence to aspirin (Table 1). Compared to patients with good adherence, patients with poor adherence had increased comorbidity as measured by the Charlson score (1.6 SD 1.4 versus 1.2 SD 1.5, P=0.05) and poor adherers were more likely to be depressed (BDI score ≥10; 63% versus 41%, P=0.01).
Table 1.
Association between Sociodemographics, Comorbidities, and Depression Vulnerabilities with Adherence to Aspirin*
| Characteristic | Poor adherence (<80%) N=38 |
Good adherence (≥80%) N=131 |
P-value |
|---|---|---|---|
| Age, mean (SD), years | 58.5 (11.2) | 59.5 (12.4) | 0.64 |
| Female, % | 52.6 | 41.2 | 0.21 |
| White, % | 78.9 | 88.5 | 0.13 |
| Partner, % | 63.2 | 65.6 | 0.78 |
| Prior myocardial infarction, % | 42.1 | 22.6 | 0.02 |
| Charlson score, mean (SD) | 1.6 (1.4) | 1.2 (1.5) | 0.05a |
| Prior history of depression, % | 43.6 | 25.6 | 0.03 |
| Depressed during ACS hospitalization (BDI ≥ 10), % | 63.2 | 40.5 | 0.01 |
| Number of role transitions, mean (SD) | 1.3 (1.2) | 0.7 (0.9) | 0.01a |
| Interpersonal conflict (Dyadic Adjustment Scale), mean (SD) | 2.5 (1.1) | 2.1 (0.7) | 0.06a |
| Cognitive vulnerability (Dysfunctional Attitudes Scale), mean (SD) | 76.0 (18.5) | 78.7 (22.0) | 0.48 |
| Behavioral vulnerability (Pleasant Events Scale for the Elderly), mean (SD) | 0.3 (0.3) | 0.3 (0.2) | 0.47b |
Abbreviations: BDI, Beck Depression Inventory; SD, standard deviation.
For the PES-E scale, scores were recoded so that higher scores indicate infrequency of pleasant events. Higher scores on vulnerability scales indicate increased vulnerability. All displayed descriptive statistics represent values before any transformations were applied to the scales. Chi-squared tests were used to compare proportions and t-tests were used to compare differences in continuous measures except where specified otherwise.
Scores were square-root transformed prior to performing the t-test.
Mann-Whitney test used for comparison.
Depression Vulnerabilities
There was low correlation between our measures of depression vulnerabilities (correlation coefficients ranged from −0.07 to 0.21). In bivariate analyses (Table 1), there was a higher mean number of role transitions in the year prior to the ACS in patients with poor adherence as compared to patients with good adherence (1.3 SD 1.2 versus 0.7 SD 0.9; p=0.01). There was also a trend toward the measure of interpersonal conflict (Dyadic Adjustment scale) being associated with poor medication adherence (p=0.06). In contrast, there were no significant associations between dysfunctional attitudes or infrequency of pleasant events with medication adherence (p=0.47 and p=0.48, respectively).
The prevalence of different types of role transitions is shown in Figure 1. The most common role transitions included a new major health problem other than their cardiovascular disease, a geographic move, a new job or graduation, and a job loss or retirement. Overall, there was a higher prevalence of increased role transitions (>1) among patients with poor adherence as compared to patients with good adherence (41.0% versus 16.5%, P=0.001). Further, there was a graded association between the number of role transitions in the prior year and prevalence of poor adherence (Figure 2).
Figure 1.
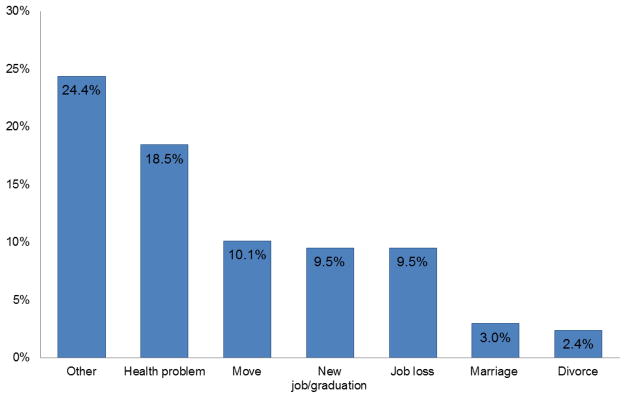
Prevalence of Role Transitions in Prior Year among Post-Acute Coronary Syndrome Patients (N=168)*
*Other major role transitions included events such as death or new major illness in a close family member or friend, arrival of a new child or grandchild, and arrival or departure of someone from the household
Figure 2.
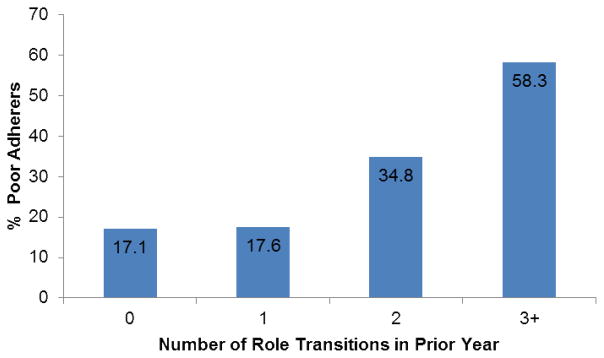
Graded Association between Number of Role Transitions and Percentage of Patients with Poor Adherence (<80%) to Aspirin after Acute Coronary Syndrome
In a model predicting aspirin adherence that included sociodemographics, comorbidity, and depressive symptoms, only depressive symptoms predicted poor medication adherence (Table 2). When the depression vulnerabilities were individually added to the model, only role transitions and interpersonal conflict significantly predicted medication adherence. In the model that included all the depression vulnerabilities simultaneously, both role transitions (beta coefficient (SE) −3.32 (1.38); P=0.02) and interpersonal conflict (beta coefficient (SE) −3.78 (1.74); P=0.03) were associated with poor medication adherence, whereas dysfunctional attitudes and infrequency of pleasant events were not. The beta coefficient for the contribution of depressive symptoms to adherence changed little (from −0.40 to −0.42) when all of the depression vulnerabilities were added to the model. A formal test of mediation using Preacher and Hayes’ bootstrap approach confirmed that there was no significant mediation by depression vulnerabilities of the effect of depressive symptoms on aspirin adherence after ACS.
Table 2.
Predictors of Adherence to Aspirin after Acute Coronary Syndromes (N=169)*
| Characteristic | Model 1 Beta (SE) |
P-value | Model 2a Odds Ratio Beta (SE) |
P-value | Model 2b Beta (SE) |
P-value | Model 2c Beta (SE) |
P-value | Model 2d Beta (SE) |
P-value | Model 3 Beta (SE) |
P-value |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Beck Depression Inventory score | −0.40 (0.17) | 0.02 | −0.38 (0.17) | 0.03 | −0.32 (0.17) | 0.07 | −0.49 (0.18) | 0.007 | −0.41 (0.20) | 0.04 | −0.42 (0.20) | 0.04 |
| Number of role transitions | - | - | −3.43 (1.38) | 0.01 | - | - | - | - | - | - | −3.32 (1.38) | 0.02 |
| Interpersonal conflict | - | - | - | - | −3.65 (1.74) | 0.04 | - | - | - | - | −3.78 (1.74) | 0.03 |
| Dysfunctional attitudes | - | - | - | - | - | - | 0.10 (0.07) | 0.17 | - | - | 0.12 (0.07) | 0.08 |
| Lack of pleasant events | - | - | - | - | - | - | - | - | 0.61 (7.02) | 0.93 | 1.67 (6.91) | 0.81 |
Abbreviations: SE, Standard Error
All models were additionally adjusted for age, gender, race, partner status, and Charlson score; none of these covariates were significantly associated with aspirin adherence (all P>0.1).
Model 1 tests the extent to which depressive symptoms predicted aspirin adherence in the 3 months after hospitalization for an acute coronary syndrome; adjusted R2 = 0.03.
Models 2a – 2d test the extent to which depressive symptoms predicted aspirin adherence in the 3 months after hospitalization for an acute coronary syndrome after accounting for each depression vulnerability, individually.
Model 3 tests the extent to which depressive symptoms predicted aspirin adherence in the 3 months after hospitalization for an acute coronary syndrome after accounting for all of the depression vulnerabilities concurrently; adjusted R2 = 0.08.
Conclusions
The psychosocial context up to one year prior to an ACS - as measured by interpersonal conflict and the number of major role transitions - was associated with lower adherence to aspirin after ACS even after accounting for depressive symptoms, sociodemographics, and comorbidity characteristics. These findings expand upon prior literature showing that psychosocial factors play an important role in the way patients take their cardiovascular medications.(26) Prior studies have found an association between major life events and adherence to medications prescribed for medical illnesses including hypertension and human immunodeficiency virus.(27–29) Furthermore, when considered alongside the finding that a measure of interpersonal conflict also predicted worse adherence, the current study demonstrates that among the potential depression vulnerabilities, psychosocial factors may be the most impactful on medication adherence.
According to interpersonal theory, the psychosocial factors we measured – major role transitions and interpersonal conflict – have the potential to cause emotional distress, and this distress compromises a patients’ ability to handle social roles, which puts them at even more risk for further negative events.(30, 31) The mechanism(s) by which these interpersonal factors place patients at risk of poor medication adherence remains unknown, but we speculate that this cycle of distress leads to deficits in social support and an inability to maintain healthy habits such as medication adherence. Both social support and habit strength have been associated with medication adherence in prior studies.(32–36)
Interestingly, adding depression vulnerabilities to the model predicting medication adherence did not significantly reduce the association between depressive symptoms and medication adherence and our formal test of mediation confirmed that there was no mediation by these factors. This finding suggests that the measured psychosocial depression vulnerabilities (interpersonal conflict and major role transitions) impact medication adherence independent of depressive symptoms. Holt and colleagues similarly found that major life events, a measure of psychosocial depression vulnerability similar to our measure of role transitions, were associated with lower adherence to antihypertensive medications independent of depression.(27)
In contrast with psychosocial factors, demographic factors were not associated with medication adherence. This result is consistent with multiple studies that have shown demographic factors to have little role in predicting who will be adherent to medications.(37, 38)
A major strength of this study includes its use of the gold-standard measure of medication adherence – electronic measurement - and the careful collection of detailed information regarding psychological characteristics among patients with cardiovascular disease. There were also several limitations including a small sample size and the abbreviated range in depression symptoms for study participants (BDI scores of 5–9 excluded). Furthermore, the study only measured adherence to aspirin – hence the impact of these depression vulnerabilities on adherence to the full post-ACS medication regimen remains unknown.
Implications
The current findings highlight the potential importance for clinicians to assess the psychosocial milieu among post-ACS patients as a means of ascertaining risk of poor adherence to medications. Clinicians taking care of ACS patients should be mindful of obtaining histories about the psychosocial context that preceded the ACS event. A particular focus on recent major life transitions and interpersonal conflict with key members of the patient’s social network may alert clinicians to the potential for adherence problems. Future studies should seek to clarify the mechanisms through which role transitions and interpersonal conflict impact medication adherence. Interventions that focus on the resolution of interpersonal conflict and on the promotion of positive adjustment to role transitions should be formally evaluated to determine whether they can improve adherence to medications in the post-ACS setting. Approaches that seek to increase the automaticity of medication-taking behaviors may also be worth testing as they may help patients become more resilient to challenges from the psychosocial environment.(39)
Acknowledgments
Sources of Funding: This work was supported by grants HL08817 and HC25197 from the National Institutes of Health (NIH), Bethesda, MD. Dr. Kronish received supported by grant K23-HL098359 from the National Heart, Lung, and Blood Institute (NHLBI) and by a Scientist Development Grant (10SDG2600321) from the American Heart Association. Dr. Alcantara is supported by grant 3R01HL115941-01S1 from NHLBI.
Footnotes
Conflict of Interest Statement: The authors have no conflicts of interest to disclose.
Conflicts of Interest: Its contents are solely the responsibility of the authors and do not necessarily represent the official view of the National Center for Research Resources or the NIH. No funding bodies had any role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
References
- 1.Nicholson A, Kuper H, Hemingway H. Depression as an aetiologic and prognostic factor in coronary heart disease: a meta-analysis of 6362 events among 146 538 participants in 54 observational studies. Eur Heart J. 2006;27:2763–2774. doi: 10.1093/eurheartj/ehl338. [DOI] [PubMed] [Google Scholar]
- 2.van Melle JP, de Jonge P, Spijkerman TA, et al. Prognostic association of depression following myocardial infarction with mortality and cardiovascular events: a meta-analysis. Psychosom Med. 2004;66:814–822. doi: 10.1097/01.psy.0000146294.82810.9c. [DOI] [PubMed] [Google Scholar]
- 3.Whang W, Shimbo D, Kronish IM, et al. Depressive symptoms and all-cause mortality in unstable angina pectoris (from the Coronary Psychosocial Evaluation Studies [COPES]) Am J Cardiol. 2010;106:1104–1107. doi: 10.1016/j.amjcard.2010.06.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Gehi A, Haas D, Pipkin S, Whooley MA. Depression and medication adherence in outpatients with coronary heart disease: findings from the Heart and Soul study. Arch Intern Med. 2005;165:2508–2513. doi: 10.1001/archinte.165.21.2508. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Rieckmann N, Gerin W, Kronish IM, et al. Course of depressive symptoms and medication adherence after acute coronary syndromes: an electronic medication monitoring study. J Am Coll Cardiol. 2006;48:2218–2222. doi: 10.1016/j.jacc.2006.07.063. [DOI] [PubMed] [Google Scholar]
- 6.DiMatteo MR, Lepper HS, Croghan TW. Depression is a risk factor for noncompliance with medical treatment: meta-analysis of the effects of anxiety and depression on patient adherence. Arch Intern Med. 2000;160:2101–2107. doi: 10.1001/archinte.160.14.2101. [DOI] [PubMed] [Google Scholar]
- 7.Rasmussen JN, Chong A, Alter DA. Relationship between adherence to evidence-based pharmacotherapy and long-term mortality after acute myocardial infarction. JAMA. 2007;297:177–186. doi: 10.1001/jama.297.2.177. [DOI] [PubMed] [Google Scholar]
- 8.Spertus JA, Kettelkamp R, Vance C, et al. Prevalence, predictors, and outcomes of premature discontinuation of thienopyridine therapy after drug-eluting stent placement: results from the PREMIER registry. Circulation. 2006;113:2803–2809. doi: 10.1161/CIRCULATIONAHA.106.618066. [DOI] [PubMed] [Google Scholar]
- 9.Rieckmann N, Burg MM, Kronish IM, et al. Aspirin adherence, depression and one-year prognosis after acute coronary syndrome. Psychother Psychosom. 2011;80:316–318. doi: 10.1159/000323168. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Katon WJ, Lin EH, Von Korff M, et al. Collaborative care for patients with depression and chronic illnesses. N Engl J Med. 2010;363:2611–2620. doi: 10.1056/NEJMoa1003955. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Kronish IM, Rieckmann N, Burg MM, et al. The effect of enhanced depression care on adherence to risk-reducing behaviors after acute coronary syndromes: findings from the COPES trial. Am Heart J. 2012;164:524–529. doi: 10.1016/j.ahj.2012.07.024. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Davidson KW, Rieckmann N, Lesperance F. Psychological theories of depression: potential application for the prevention of acute coronary syndrome recurrence. Psychosom Med. 2004;66:165–173. doi: 10.1097/01.psy.0000116716.19848.65. [DOI] [PubMed] [Google Scholar]
- 13.Rieckmann N, Burg MM, Gerin W, et al. Depression vulnerabilities in patients with different levels of depressive symptoms after acute coronary syndromes. Psychother Psychosom. 2006;75:353–361. doi: 10.1159/000095441. [DOI] [PubMed] [Google Scholar]
- 14.Kronish IM, Rieckmann N, Halm EA, et al. Persistent depression affects adherence to secondary prevention behaviors after acute coronary syndromes. J Gen Intern Med. 2006;21:1178–1183. doi: 10.1111/j.1525-1497.2006.00586.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Cannon CP, Battler A, Brindis RG, et al. American College of Cardiology key data elements and definitions for measuring the clinical management and outcomes of patients with acute coronary syndromes. A report of the American College of Cardiology Task Force on Clinical Data Standards (Acute Coronary Syndromes Writing Committee) J Am Coll Cardiol. 2001;38:2114–2130. doi: 10.1016/s0735-1097(01)01702-8. [DOI] [PubMed] [Google Scholar]
- 16.Power MJ, Katz R, Mcguffin P, et al. The Dysfunctional Attitude Scale (DAS) - a comparison of Form-A and Form-B and proposals for a new subscaled version. J Res Pers. 1994;28:263–276. [Google Scholar]
- 17.Sanz JVC. Adaptacion espanola de la escala de actitudes disfuncionales (DAS) de Beck. Propiedad Psicometr Clin. 1993;19:707–750. [Google Scholar]
- 18.Teri L, Lewinsohn P. Modification of the Pleasant and Unpleasant Events Schedules for use with the elderly. J Consult Clin Psychol. 1982;50:444–445. doi: 10.1037//0022-006x.50.3.444. [DOI] [PubMed] [Google Scholar]
- 19.Markowitz JC, Leon AC, Miller NL, et al. Rater agreement on interpersonal psychotherapy problem areas. J Psychother Pract Res. 2000;9:131–135. [PMC free article] [PubMed] [Google Scholar]
- 20.Spanier GB. Measuring dyadic adjustment - new scales for assessing quality of marriage and similar dyads. J Marriage Fam. 1976;38:15–28. [Google Scholar]
- 21.Beck A, Steer RA. Manual for the Beck Depression Inventory. San Antonio: Psychological Corporation; 1993. [Google Scholar]
- 22.Strik JJ, Honig A, Lousberg R, Denollet J. Sensitivity and specificity of observer and self-report questionnaires in major and minor depression following myocardial infarction. Psychosomatics. 2001;42:423–428. doi: 10.1176/appi.psy.42.5.423. [DOI] [PubMed] [Google Scholar]
- 23.Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40:373–383. doi: 10.1016/0021-9681(87)90171-8. [DOI] [PubMed] [Google Scholar]
- 24.Ho PM, Bryson CL, Rumsfeld JS. Medication adherence: its importance in cardiovascular outcomes. Circulation. 2009;119:3028–3035. doi: 10.1161/CIRCULATIONAHA.108.768986. [DOI] [PubMed] [Google Scholar]
- 25.Preacher KJ, Hayes AF. SPSS and SAS procedures for estimating indirect effects in simple mediation models. Behav Res Methods Instrum Comput. 2004;36:717–731. doi: 10.3758/bf03206553. [DOI] [PubMed] [Google Scholar]
- 26.Osterberg L, Blaschke T. Adherence to medication. N Engl J Med. 2005;353:487–497. doi: 10.1056/NEJMra050100. [DOI] [PubMed] [Google Scholar]
- 27.Holt EW, Muntner P, Joyce C, et al. Life events, coping, and antihypertensive medication adherence among older adults: the Cohort Study of Medication Adherence among Older Adults. Am J Epidemiol. 2012;176 (Suppl 7):S64–71. doi: 10.1093/aje/kws233. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Bottonari KA, Safren SA, McQuaid JR, Hsiao CB, Roberts JE. A longitudinal investigation of the impact of life stress on HIV treatment adherence. J Behav Med. 2010;33:486–495. doi: 10.1007/s10865-010-9273-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Leserman J, Ironson G, O’Cleirigh C, Fordiani JM, Balbin E. Stressful life events and adherence in HIV. AIDS Patient Care STDS. 2008;22:403–411. doi: 10.1089/apc.2007.0175. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Joiner T, Coyne JC, editors. The interactional nature of depression: advances in interpersonal approaches. Washington, D.C: American Psychological Association; 1999. [Google Scholar]
- 31.Gotlib IH, Hammen CL. Psychological aspects of depression: toward a cognitive-interpersonal integration. Oxford: Wiley; 1992. [Google Scholar]
- 32.DiMatteo MR. Social support and patient adherence to medical treatment: a meta-analysis. Health Psychol. 2004;23:207–218. doi: 10.1037/0278-6133.23.2.207. [DOI] [PubMed] [Google Scholar]
- 33.Molloy GJ, Perkins-Porras L, Strike PC, Steptoe A. Social networks and partner stress as predictors of adherence to medication, rehabilitation attendance, and quality of life following acute coronary syndrome. Health Psychol. 2008;27:52–58. doi: 10.1037/0278-6133.27.1.52. [DOI] [PubMed] [Google Scholar]
- 34.Bolman C, Arwert TG, Vollink T. Adherence to prophylactic asthma medication: habit strength and cognitions. Heart Lung. 2011;40:63–75. doi: 10.1016/j.hrtlng.2010.02.003. [DOI] [PubMed] [Google Scholar]
- 35.Voils CI, Maciejewski ML, Hoyle RH, et al. Initial validation of a self-report measure of the extent of and reasons for medication nonadherence. Med Care. 2012;50:1013–1019. doi: 10.1097/MLR.0b013e318269e121. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Phillips LALH, Leventhal EA. Assessing theoretical predictors of long-term medication adherence. Patients’ treatment-related beliefs, experiential feedback and habit development. Psychol Health. doi: 10.1080/08870446.2013.793798. In press. [DOI] [PubMed] [Google Scholar]
- 37.Mann DM, Woodward M, Muntner P, Falzon L, Kronish I. Predictors of nonadherence to statins: a systematic review and meta-analysis. Ann Pharmacotherapy. 2010;44:1410–1421. doi: 10.1345/aph.1P150. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Chan DC, Shrank WH, Cutler D, et al. Patient, physician, and payment predictors of statin adherence. Med Care. 2010;48:196–202. doi: 10.1097/MLR.0b013e3181c132ad. [DOI] [PubMed] [Google Scholar]
- 39.O’Carroll RE, Chambers JA, Dennis M, Sudlow C, Johnston M. Improving adherence to medication in stroke survivors: a pilot randomised controlled trial. Ann Behav Med. 2013 doi: 10.1007/s12160-013-9515-5. Epub ahead of print. [DOI] [PubMed] [Google Scholar]